Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
CLIN.CHEM.39/7,
1398-1403
(1993)
On the Calculation of Reference Change Values, with Examples from a Long-Term
Study
Jos#{233}
M. Queralt#{243},’
James C. Boyd,2’3 and Eugene K. Harris2
Reference change values (sometimes called critical differences) indicate statistically important changes between test values obtained on two occasions. They are
commonly computed from the median (or mean) withinsubject variance observed in repeated test measurements on a number of subjects. With this computational
all observed within-subject variances are assumed to be estimates of a constant true variance, the
same for all individuals. Moreover, any possible correlation between successive values is almost always ignored.
This simplified methodology differs from the method origapproach,
inally proposed for computing reference change values,
which accounts for variability in true variances and for
serial correlation. From data obtained from repeated
measurements over 2 to 5 years in 72 physically healthy
subjects, we computed and compared reference change
values in 18 serum analytes, using the simplified method
and the originally proposed procedure. Although the original method is more complicated and requires a computer
program, we believe that it produces more-reliable reference change values than those obtained by the simplified
approach. The former are generally larger, but remain
sensitive to clinically important changes in the individual.
Information about within-subject variation may also
provide an objective basis for deciding on the best analytical approach to a clinical problem (1,2) or for determining
general analytical
goals in clinical chemistry (3, 4). Another use for data on within-subject variabffity is in the
development of “reference change” values (or “critical
differences”) to judge the significance
of an observed
change between successive test results. Reference change
criteria were originally proposed by Harris and Brown (5).
They used a previously published formula (6) for estimating the standard deviation across individuals of the true
within-person variances for any analyte. Then, assuming
that these true variances were log-normally distributed,
as indicated by the distribution of observed variances, they
discussed the computation of reference changes with examples based on weekly measurements
of serum analytes
in 37 healthy British men. This methodology was applied
again several years later (7) to data on serum calcium and
alkaline phosphatase in a much larger sample of men and
women examined semiannually over a 7- to 9-year period
at a health
maintenance
organization
in Japan. In a later
addendum (8), a simpler formula for computing reference
change values was validated, and this is the method used
here.
IndexIng Terms:
variation
statistics
data handling
.
within-subject
Laboratory data interpretation
is guided by the comparison of the result(s) obtained in one individual with
those obtained for the same analyte(s)
in a population
having known clinical characteristics.
In a different but
complementary
way, one may compare the current
result with past data from the same individual.
In the
first approach,
estimated parameters of the population,
e.g., the mean and standard deviation, are used to define
reference limits or, in a well-defined clinical
situation,
the predictive value or the likelihood ratio of a specified
analytical
result. In the individual
approach, interpretation is based on parameters
such as within-person
variability,
which define the behavior of the analyte
over time. The implied assumption here is that, so long
as the individual remains in a steady state, repeated
test results will show a homogeneous pattern over time,
reflecting that individual’s customary variabffity. This
stationary pattern will be modified if the steady state is
interrupted,
e.g., by a disease.
‘Servei de Bioquimica, Hospital de la Santa Creu I Sant Pau,
Barcelona, Spain.
2ent
of Pathology,
Box 214, University of Virginia
Health Sciences Center, Charlottesville, VA 22908.
3Author for correspondence.
Received July 8, 1992; accepted February 12, 1993.
1398
CUNICAL CHEMISTRY, Vol. 39,
No. 7, 1993
More recently,
several
studies to develop reference
change values in apparently healthy individuals have
been published (9-18). To simplify practical application,
the authors have generally assumed that the true within-subject variance for any analyte was the same in all
persons, implying that the observed variation in withinsubject variances represented only statistical
sampling
fluctuations around a constant true value. They recommend using the median (or mean) observed withinsubject variance. However, Costongs et al. (9) presented
critical differences based on the use of both the median
and the 90th percentile
of observed variances, noting
that the former
offers greater sensitivity (a smaller
critical difference) and the latter, greater specificity.
H#{246}lzel
(13, 14) recognized that true within-subject variances may well vary from person to person and tested
for this possibffity through Bartlett’s test, finding that
significant
variation occurred in none or very few of the
analytes examined.
The assumption of constant withinsubject variance, when invalid, can produce too small a
reference change value, increasing the probability
of
false alarms,
as noted by Costongs et al. (9).
To further simplify calculations,
the referenced authors (9-18) also assumed that successive test results
are statistically
uncorrelated.
When the interval be-
tween measurements is at least a month, or perhaps
even a week for most analytes, this assumption seems
reasonable, although it is rarely checked. When the
interval is only 1 or 2 days, however, as might be
common among inpatient groups, the assumption of zero
serial correlation is likely to be invalid. For example, in
a study on the use of reference change values to monitor
inpatient laboratory values, Boyd and Harris (19) found
average serial correlations (r) as high as 0.5-0.6 in daily
test results from patients in surgical
intensive care
units. The original proposal (5) for calculating reference
change values based the procedure on an autoregressive
model that allowed serial correlation.
Here we examine serial data for 18 serum analytes in a
sample of physically healthy individuals. Our primary
purpose is not merely to present another set of possible
reference change values. Rather, we are chiefly interested
in examining the differences between reference change
values computed according to the original proposal [with
the formula as modified by Harris (8)1 and those obtained
under the now common “practical” methodology.
AnalyticalMethods
The chemical assays were performed on a Hitachi 737
automated analyzer with standard
methodology (Table
1). Reagents were purchased from Boehringer
Mannheim GmbH, Mannheim, Germany.
Statistical Procedures and Results
Materials and Methods
Subjects and Specimens
This data base consists of results from 72 physically
subjects, 34 men and 38 women, ages 18-78,
who regularly attended the affective diseases clinic of
the Psychiatric Department of the Hospital de la Santa
Creu I Sant Pau in Barcelona to monitor lithium chloride preventive treatment of their affective disorder.
Lithium treatment does not interfere in vitro with the
analytical
assay of the serum constituents studied (20).
From 16 to 51 specimens (median: 30) of venous blood
were collected from each patient at intervals of 1 to 2
months (median: 40 days) over periods ranging from 21
to 67 months. Specimens (20 mL) of blood from an
antecubital
vein were collected into Vacutainer Tubes
(Becton Dickinson, Rutherford, NJ) between 0900 and
1100 after an overnight fast with no special restrictions
imposed. To minimize stress and standardize
for the
healthy
effect of posture, subjectswere recumbent for 20-30 miii
before the blood was drawn. When necessary, a tourniquet was used for <2 mm. The same experienced phlebotomist drew samples throughout the study. Clinical
interrogation and physical examination were performed
at every phlebotomy.
Specimens were allowed to clot at room temperature,
and serum was obtained after centrifugation
(3000 x g
for 15 mm at 18-22 #{176}C)
within 2 h of collection and
separation. Analysis was performed the same day or,
rarely, the next day after storage at 4#{176}C.
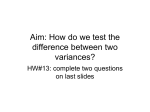
Except for serum y-glutamyltransferase, observed
within-person variances conformed to log-normal distributions, although outliers often appeared. xamp1es are
shown in Figure 1. Assuming
log-normality,
robust
estimates of the mean and variance of the logarithms of
observed within-subject variances for each analyte were
obtained through Healy’s trimming
procedure
(21),
which eliminated three extreme values in each tail of
the distribution.
These estimates were converted to their counterparts in
original
units, Mean 5j2 and Var 2, by using standard
formulas relating the mean and variance of a log-normal
variable to the mean and variance of its logarithm, i.e.,
Mean
Var
,2
sj2
=
=
exp[Mean
log 2
+ (Var log 2)I2]
(Mean s2)2[exp( Var
log 2)
-
1]
Table 1. Analytes and Methods
Method
Analyte
Albumin,gIL
Alk. phosphatase,U/L
ALT, UIL
AST, U/L
Calcium,mmol/L
Chloride,mmol/L
Cholesterol,mmol/L
Creatinine,moI/L
GGT, U/L
Glucose, mmol/L
LDH, U/L
Phosphate,mmol/L
Potassium,mmol/L
Protein,g/L
Sodium,mmol/L
Triglyceride, mmol/L
Uricacid,n,ol/L
Urea,mmol/L
Tables
1-4:
ALT, alanine aminotransferase;
Bromcresol
green,end point,600 nm
p-Nltrophenylphosphate,diethanolamine,kinetic,415 nm, 37#{176}C
Standardkineticmethodwithout pyndoxalphosphate,
340 nm, 37#{176}C
Standardkineticmethod without pyridoxalphosphate,340 nm, 37#{176}C
o-Cresolphthalein,8-hydroxyquinoline,546 nm
Ion-selectiveelectrode
Cholesteroloxidase-peroxidase,end point,505 nm
Jaff#{233}
withoutdeproteinizatlon,kinetic,505 nm
L-p-Glutamyl-3-carboxy-4-anilide,
kinetic,415 nm, 37#{176}C
Hexokinase,glucose-6-phosphatedehydrogenase,340 nm
Standardkineticmethod:pyruvateto lactate,kinetic,340 nm, 37#{176}C
Ammoniummolybdate,340 nm
Ion-selectiveelectrode
Biuret,546 nm
Ion-selectiveelectrode
Lipase,glycerolkinase,glycerol-phosphate
dehydrogenase,
perioxidase,
endpoint,505 nm
Uricase-peroxidase,
endpoint,505 nm
Urease,glutamate dehydrogenase,kinetIc,340 nm
AS1 aspartate aniinotransferase;GGT, y-glutamyftransferase;LDH, lactate dehydrogenase.
CUNICAL CHEMISTRY,
Vol.39, No. 7, 1993 1399
Distribution of Albumin
Log Variances
Distribution
r
0.995
0.900
80O
0.990
0.980,
0.950.
0.900
0.800
.70or
0.700
0.800
0.950
-
.-.
-#{176}-
0.400
0.300
0200
D.30O
,00
0.100
-,
r#{176}
0.500
-
Log Variances
0.999
#{176}#{149}#{176}
8:F
of Cholesterol
__:-
0.100
0.050
08
0.020 0.010
005 r
0.001:
0.60
__
.-
-
0.005
nmi
0.80
1.00
1.20
1.40
1.60
1.80
2.00
log V,5J109
-3.0
2.20
Distribution
Distribution of Alkaline Phosphatase Log Variances
v,
0.950
0.999
0.995
0.993
0.950
0.950
0.900
-
0.9001
‘
0.800
0.700
.i(”
§:
t
0.300i
0.200(
of Potassium
.
0.00
log vanss,oe
Log Variances
-
-
0.800
0.700
..3
-1.0
-2.0
8:
0.
-
=
-
0.300
0200
0.100
0.100
0.050
0.020
0.010,_-
H
-
0
22
-
v.v’u
0.005
0.001
4.00
5.00
6.00
7.00
8.00
09
9.00
-3.1
-2.9
-2.7
-2.5
-2.3
-2.1,
log varsrce
-1.9
FIg. 1. Plots of the cumulative distributions of log-transformed observedwithin-personvariances for four representative analytes: albumin,
alkalinephosphatase,cholesterol,and potassium
The ordinatevalues have beentransformedto a probabilityscale.The observed within-person variances generally conformed to log-normal distributions as seen
in the linear cumulative distribution plots shown, although outliers were oftenobserved(seetext)
Then, the standard deviation (SD) of the true withinsubject variances was estimated by using the previously
mentioned formula
(6):
Estimated SD of Q2
([Var
Here
sj2
-
1)1 (n
-
1)I(n + 1)}h/2 (3)
refer to the observed and true withinsubject variance, respectively, for a given analyte in the
ith individual,
and n is the average number of samples
per subject. The estimated mean of 2 over all individuals is the same as the (trimmed) mean of s2. When the
true within-subject variance is, in fact, constant for all
persons tested, the right-hand side of equation 3 will be
negative (or zero), and the SD of o2 may then be
assumed equal to zero.4 The median and estimated CV
of true variances are given in Table 2. We note that
there appears to be considerable variation among individuals in their true variances o2 for all the analytes
5j2
and
2(Mean sj2)2/(n
-
=
2
4A simpler but less sensitive test of the homogeneity of true
variances
is provided by an “index of heterogeneity” (22, 23),
defined as the ratio of the observed CV of a set of within-person
variances to the theoretical
CV, [2/(n - 1)J”. If the difference
between this ratio and its expected value of unity exceeds, say,
twice its standard deviation of 1/(2n)” under the hypothesis of
homogeneity, then the true variances should be considered heter-
ogeneous.
1400
studied (even electrolytes),
ranging from an estimated
CV of 9.8% for chloride to 356% for y-glutamyltransferase. A log-normal distribution
of the observed variances for a given analyte implies a log-normal distribution (but with a smaller variance, of course) for the
underlying true variances.
CUNICAL CHEMISTRY, Vol. 39, No. 7, 1993
AnalyticalVariance
Estimates
of combined within-day and long-term analytical
variance were obtained from a representative
6-month period of day-to-day results for samples provided by the Spanish Society of Clinical
Chemistry as
part of a nationwide proficiency survey. Although
knowledge of the analytical
variance is not required
to
compute reference change values, it may be of general
interest to examine the ratios of analytical
to average
within-subject
standard
deviations (with the latter including analytical variation).
These ratios are listed in
Table 2.
It has been widely proposed that the ratio of analytical to average biological standard deviation not exceed
one-half. This translates
to a ratio of analytical
to
overall within-person
variation
45%. Most of the ratios listed in Table 2 are at or below this proposed limit,
but a few substantially
exceed it (aspartate amunotransferase and, typically,
calcium, sodium, and chloride).
Note, however, that the analytical variation referred to
Table 2. EstImated
Parameters of True WithIn-Subject
Variances
Analyt.
Median uf
CV (of), %
Albumin
Alk phos.
4.5
567
42.7
17.0
0.018
11.4
0.24
78.4
37.7
129
29.3
169
34.5
101
23.2
9.8
72.2
18.4
ALT
AST
Calcium
Chloride
Cholesterol
Creatinine
GOT
Glucose
LDH
Phosphate
Potassium
Protein
0.33
3050
0.018
0.081
8.4
8.7
Sodium
Triglyceride
Uric acid
Urea
a’
30.2
0.099
1370
0.91
(./m.dIan
o,),
%
Table 3. Mean Serial Correlation Coefficient (7) and the
Number of individual Coefficients (r,)for Which rAn,)
Is >2, by Analyte
r
Analyts
0.17
0.43
50.6
Albumin
Alk. phosphatase
ALT
52.7
AST
0.18
80.6
0.24
25.5
24.3
Calcium
Chloride
Cholesterol
Creatinine
51.6
61.7
19.1
20.1
GGT
Glucose
35.9
33.3
LDH
21.4
22.2
15.3
36.9
Phosphate
Potassium
Protein
356
193
41.3
45.6
45.9
18.3
32.6
0.24
0.18
0.17
0.21
0.31
0.26
0.32
0.15
Sodium
0.12
0.21
TriglycerIde
0.16
16
20.4
Uric acid
0.20
0.17
21
11
in Table 2 includes both long-term and within-day
whereas the proposed goal refers only to
short-term (e.g., within-run)
analytical
variation.
Serial Correlation(Autocorrelation)
Before calculating
reference change values, the possibility of serial correlation between test results should be
explored.
Because successive observations
were, on the
average, -40 days apart, one might expect the average
correlation
between them to be zero for all analytes.
Assuming zero true correlation between successive values in the ith individual, the standard deviation of an
observed serial correlation r1 based on n observations is
given by 1In”.
Then, the product r(n)
should be
distributed
as a standard normal deviate over all individuals. That is, 95% of the values of this product for any
analyte should lie within the limits mean ± 1.96. Given
72 subjects,no more than four observed values of r(n)
should have an absolute value >2. However, as shown in
Table 3, this condition did not hold for any analyte. The
average observed values of r are also listed in Table 3.
Reference Change Values
For any given difference D between two successive
test results, we can calculate the proportion of individuals for whom that difference is statistically
significant
at the 0.05 probability level. Under the common method
of computing reference change values, i.e., using the
median observed within-subject
variance, this proportion is set at 50%. The original proposal selected a much
higher proportion, 90% or 95% of the true within-subject
variances o2, to avoid the problem of many false alarms.
proportion
at any given value,
24
28
9
11
12
21
0.12
Urea
a Total number of indMduals was 72.
=
variabffity,
this
29
67.4
8.4
17.7
combined within-day and long-term analytical standard deviation.
Setting
implies
13
42
25
16
20
11
16
15
say, p,
using o,2, the pth percentile of the distribution
of 2, to calculate the reference change value, say, DC.
The formula may be written
2.77[oj,2
(1
-
where F is the average serial correlation
coefficient.
Table 4 includes several possible values of DC: (a) as
commonly done, using 8052 (the median observed variance) and assuming zero autocorrelation;
(b) using s092
(the 90th percentile of the distribution of observed variances) and again assuming zero autocorrelation; and (c)
Table 4. Reference Change Values (RCV5) Computed
by Using (a) Median s, (b) oee2, (c) 0o.ee2 and P
RCV by each appreach and psrc.ntag.
dlffarsnces .xc..dlng the RCV
Analyte
Albumin
Aik phos.
ALT
AST
Calcium
ChlorIde
Cholesterol
Creatinlne
GGT
Glucose
WH
Phosphate
Potassium
Protein
SodIum
Triglyceride
Uricacid
Urea
MedIan
5.8
67
17
11
f
(4.g)b
(2.8)
(8.1)
(7.3)
0.36 (3.7)
9.4 (2.9)
1.4
(4.8)
25
(3.5)
12
(11.3)
1.5
(5.7)
151
(4.4)
0.37 (4.4)
0.81 (3.6)
8.2
(3.2)
8.3
(2.9)
0.84 (8.0)
102
2.7
(4.1)
(4.4)
o.2,
2
8.0
129
of
(1.5)
6.8
(0.4)
38
19
(2.0)
(2.5)
0.45 (1.8)
11
(1.6)
2.1 (0.8)
30
(0.6)
61
(1.1)
2.3 (1.2)
217
(1.6)
94
33
18
0.37
9
1.9
25
36
1.9
181
?
(2.7)
(1.3)
(1.3)
(2.5)
(2.9)
(2.2)
(4.7)
0.95 (1.5)
9.7 (2.1)
(1.5)
(3.5)
(2.6)
(2.5)
0.43 (2.9)
0.85 (2.9)
8.7 (2.7)
9.6 (2.0)
8.8 (5.3)
0.48 (1.9)
1.8 (1.4)
134 (0.9)
3.3 (2.1)
1.8 (1.4)
118
(2.0)
3.2 (2.6)
From Table 3.
Values in parenthesesrepresent the percentage of consecutive differencesthatexceededtherespectiveROy in the population of patients studied.
a
CLINICAL CHEMISTRY, Vol. 39,
No. 7,
1993
1401
using the method recommended
here, i.e., using equation 4 with the estimated 90th percentile of true variances oO9
and F values given in Table 3. As stated
above, the distribution of o2 is assumed to be lognormal with the mean equal to the mean of observed
within-subject variances (after trimming) and standard
deviation computed through equation 3. It is not difficult, therefore, to determine any desired percentile of
the distribution of o2, again using equations 1 and 2 but
now solving for the mean and variance on the log scale.
A BASIC program for computing D is available on
request. To provide information regarding the practical
implications of the different approaches, the reference
change values derived by each method were applied
retrospectively to all the successive differences observed
in each patient. The percentages of consecutive
differences in the population of patients studied that exceeded
the reference change values derived by each method are
also reported in Table 4.
Discussion
We have gone through a series of statistical procedures to extract reference change values, that is, critical
values for judging the clinical importance of an observed
difference between two successive measures of a blood
constituent in a patient of a certain type. The values
obtained
are naturally
dependent on the characteristics
of the population
sampled-in
this case, physically
healthy but mentally affected patients on lithium treatment, being seen as outpatients about every 40 days at
a Spanish clinic. Some of the reference change values
(Table 4) may seem too high, especially for such electrolytes as sodium, chloride, or calcium. This may be due,
in part, to the effects of chronic lithium treatment
in
these particular
subjects and to the relatively
period of time during which they were studied,
long
both
factors inducing larger within-subject variances than
may be seen in other groups.
Chronic lithium administration is known to induce endocrine syndromes of
primary
hyperparathyroidism and hypothyroidism in
some of the patients so treated (24). Lithium administration also exerts various renal tubular effects, manifesting as mild increases in serum creatinine (25) and
lower concentrations of sodium (26) and uric acid (27). A
few patients develop nephrogenic
diabetes insipidus
(24) secondary to lithium treatment. Any of these syndromes and their corresponding
effects on laboratory
values could lead to observation of larger than expected
within-subject
variances.
More important
in our view is the substantial variability among (true) within-subject
variances shown by
these subjects for every one of the analytes studied,
especially the enzymes and cholesterol. This is hardly
unexpected and is likely to manifest itself in any group
of subjects studied over a reasonable length of time. For
the sake of simplicity or convenience, this variation has
been ignored in most recent studies supposed to be
developing
reference
change
values
for clinical
use.
Clearly, a reference change value based on the median
observed variance will be too small (less than statisti1402
CUNICAL CHEMISTRY, Vol. 39,
No. 7, 1993
cally significant) for those subjects whose true withinsubject variances are greater than the median value of
the group.
A compensating factor, however, is a positive correlation between successive values. This acts to reduce the
reference change value, as indicated by the (1 F) term
in equation 4. This influence,
plus the fact that the
distribution
of true variances will be narrower than the
-
distribution of observed variances, explains
why the
reference change values in column c of Table 4 are often
(although not always) considerably smaller than the
corresponding values in column b, based on the 90th
percentile of observed variances but ignoring any correlation between values. In general, however, the reference change values in column c are, as expected, larger
than those in column a, which were obtained by using
the simplified method. Interesting exceptions were chloride, creatinine, and sodium, for which the reference
change values in column c were either less than or did
not exceed the values in column a.
Related contrasts were seen for each test in the
percentages of differences in the patient population
studied that exceeded the reference change values derived by each of the approaches. Except for sodium, the
largest percentages of differences outside the respective
reference change values were seen in column a, demonstrating the oversensitivity
of the median observed
within-subject variance approach. The percentages in
column c-except for aspartate aminotransferase, alkaline aminotransferase,
and triglyceride-were
larger
than those in column b, showing the influence of accounting for existing serial correlation and true withinsubject variances. In general, the variability
observed in
the percentages of consecutive differences that exceeded
the corresponding
reference change values is less in the
third column than in the first two columns, indicating
the greater reliability of the method recommended
here
for computing reference change values.
We recommend
that the reference change value
should take account of existing serial correlation,
as
equation 4 indicates, and should be based on the 90th
percentile of o2 (if the CV of Oj2 exceeds zero), thus
assuring that the reference change value will be statistically significant (at the P = 0.05 level) in the large
majority (90%) of patients who are similar to the ones
studied. Past experience [e.g., (7)] has shown that a
reference change value based on the median observed
within-subject
variance (without
testing whether
the
true variance varies from person to person) and assuming zero autocorrelation
is essentially the same guideline as could be obtained from a much less expensive
delta-check
study utilizing
pairs of successive values
from (e.g.) existing records of a selected set of hospital
outpatients. We see little point in carrying out a special
long-term study that involves taking repeated samples
from each subject if the hard-won information on the
distribution of true variances and autocorrelations is
ignored.
Surely
the cost of the statistical analysis required cannot begin to compare to the overall cost of
obtaining
this information in the first place.
We gratefully acknowledge the assistance of the technical and
medical staff of the Departments
of Psychiatry and Biochemistry of
the Hospital deIa Santa Creu I Sant Pau.
References
1. Boyle CEL, Cummings ST, Fraser CG. Amylase versus lipase
activity assays:considerations from biological variation. Ann Cliii
Biochem 1987;24(Suppl 1):37-8.
2. Howey JEA, Browning MK, Fraser CG. Is early morning spot
urinary albumin concentration the best means of estimating
albumunuria? Ann Cliii Biochem 1987;24(Suppl 1):127-8.
3. Harris EK Statistical
principles underlying analytical goal
setting in clinical chemistry.Am J Clin Pathol 1979;72:374-82.
4 Fraser CG, Hyltoft Petersen P, Lytken Larsen M. Setting goals
for random analytical error in specific clinical monitoring situations.Clin Chem 1990;36:1625-8.
5. Harris EK, Brown SS. Temporal changes in the concentration
of serum constituents in healthy men. Distributions
of withinperson variances and their relevance to the interpretation of
differences between successive measurements. Ann Cliii Biochem
1979;16:169-76.
6. Harris EK. Distinguishing physiologic variation from analytic
variation. J Chron Dis 1970;23:469-80.
7. Harris EK, Yasaka T. On the calculation of a “reference
change” for comparing two consecutive measurements. Clin Chem
1983;29:25-30.
& Harris EK. Referencevalues for change: an addendum [Letter].
Clin Chem 1983;29:997.
9. Costongs GMPJ, Janson PCW, Has BM, Hermans J, Brombacher PJ, von Wersch JW, et al. Short-termand long-term
intra-individual variations and critical differences of clinical
chemical laboratory parameters. J Clin Chem Cliii Biochem1985;
23:7-16.
10. Godsiand IF. Intra-individual variation: significant changes in
parameters of lipid and carbohydrate metabolism in the individual
and intra-undividual variation in different test populations. Ann
Cliii Biochem 1985;22:618-24.
11. Browning
MCK, Ford RP, Callaghan SJ, Fraser CG. Intraand interindividual
biological variation of five analytes used in
assessing thyroid function: implications for necessary standards of
performance and the interpretation of results. Cliii Chem 1986;32:
962-6.
12. Harding PJ, Fraser CG. Biological variation of blood acid-
base status: consequences for analytical goal-setting and interpretation of results. Cliii Chem 1987;33:1416-8.
13. HSlzel WGE. Intra-individual variation of some analytes in
serum of patients with chronic renal failure. Clin Chem 1987;33:
670-3.
14. Holzel WGE. Intra-individual
variation of some analytes in
serum of patients with insulin-dependent diabetes meilitus. Cliii
Chem 1987;33:57-61.
15. Ford RP. Essential data derived from biologicalvariation for
establishment and use of lipid analyses. Ann Clin Biochem 1989;
26:281-S.
16. Fraser CG, Cummings ST, Wilkinson SP, Neville RG, Knox
JDE, Ho 0, MacWalter RS. Biological variability
of 26 clinical
chemistryanalytesin elderly people. Clin Chem 1989;35:783-6.
17. Juan-Pereira L, Fuentes-Arderiu
X. Intra-individual
variation of the electrophoretic serum protein fractions [Tech Brief].
Clin Chem 1989;35:1544.
18. Morris HA, Wishart JM, HorowitzM, Schou M. The reproducibility of bone-related biochemical variables in post-menopausal
women. Ann Cliii Biochem 1990;27:562-8.
19. BoydJC,HarrisEK Utility of reference change values for the
monitoring of inpatientlaboratorydata In: Zinder 0, ed. Optimal
useof the clinicallaboratory.Basel: Karger, 1986:111-22.
20. Cort#{233}s
M, Queralto JM, Castfflo MT. Study of analytical
interferences of lithium. Quim Cliii 1986;5:218.
21. Healy M,JR. Outliers in clinical chemistry quality control
schemes. Cliii Chem 1979;25:675-7.
22. Fraser CG, Harris EK Generation and application of data on
biological variation in clinical chemistry [Review]. Crit Rev Cliii
Lab Sci 1989;27:409-37.
23. Fraser CG, Wilkinson SP, Neville RG, Knox JD, King JF,
MacWalterES. Biologicvariation of common hematologic
laboratory quantities in the elderly. Am J Clin Pathol 1989;92:465-470.
24. Salata R, Klein I. Effects of lithium on the endocrinesystem:
a review. J Lab Clin Med 1987;110:130-6.
25. Vestergaard P, Amdisen A, Hansen HE, Need AG, Nordin BE.
Lithium treatment and kidney function, a survey of 237 patients
in long-term treatment. Acta Psychiatr Scand 1979;60:504-20.
26. Maletzky B, Blachly PH. The use of lithium in psychiatry
[Review]. Crit Rev Cliii Lab Sci 1971;2:279-345.
27. Anumonye A, Reading 11W, Knight F, Ashcroft GW. Uric acid
metabolism in manic-depressive illness and during lithium therapy. Lancet 1968i:1290-1.
CUNICALCHEMISTRY,Vol.39, No. 7,
1993
1403