Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
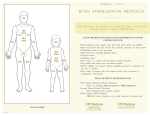
Region 5- Recommended Treatment Protocol for Burn Patients (From initial burn to 72°/transfer to Burn Care Center) 1. Primary Survey a. Airway Maintenance and consider cervical spine protection b. Breathing and ventilation (100% O2 via NRM, intubate PRN) c. Circulation and hemorrhage control d. Disability (assess neurological deficit, AVPU) e. Exposure (remove any sources of heat and remove any clothing that may be burned, covered with chemicals or are constricting) f. Secondary Survey to include Scene Hx, Physical exam, SAMPLE, etc 2. Initiate Fluid Resuscitation Estimate the burn size based on the Rule of Nines or based on patient’s palmer surface hand size (1% TBSA) to calculate the resuscitation fluid volume. Lactated Ringers solution at 3ml/kg/%TBSA burn = ml’s in first 24 hours; with ½ of this total given in the first 8 hours post injury and the remaining ½ given in the next 16 hours. Titrate to maintain urinary output as well. In children <30kg also administer D5 ½ LR solution @ maintenance rate of: For the first 1 to 10 kg - 100ml/kg/24 hours = 4ml/kg/hour For the second 11 to 20 kg - 50ml/kg/24hours = 2ml/kg/hour For any weight 21 to 30 kg - 20ml/kg/24hours = 1ml/kg/hour Example for a 12 kg child: 100 ml/kg for first 10 kg 10 kg x 100 ml = 1000ml 50 ml/kg for each kg between 11 and 20kg 2 kg x 20 ml/kg for each kg between 21 and 30 kg 50 ml = 100ml --- none needed ---=1100ml/24hours Do not give dextrose solutions (except for maintenance fluids in children) - they may cause an osmotic diuresis and confuse adequacy of resuscitation assessment. 3. Pain Management and other medications After fluid resuscitation has been initiated, pain management must be considered. Titrate doses of analgesia and sedation based on patient’s hemodynamic stability and pain control. Adjust as necessary. A tetanus immunization should be given. Antibiotics are not indicated but can be considered PRN. 4. Insert Nasogastric Tube for every intubated or unresponsive patient Give an IV Proton blocker if the patient will not be transported within 12 hours. 5. Assess Urine Output Insert Foley catheter in patients with burns >15 percent TBSA. Adequate urine output is 30 mL/hr in adults and 1 mL/kg/hr in a child less than 30 kg. Observe urine for burgundy color (seen with massive injuries or electrical burns).There is a high incidence of renal failure associated with these injuries, therefore prompt and aggressive intervention is required. Fluid bolus until output levels achieved or urine color changes to a straw color. 6. Escharotomies If transfer will be completed within 12 hours, escharotomies are rarely needed. Elevate burned extremities and assess distal pulses hourly. Assess for circumferential full thickness burns of extremities or trunk. Perform escharotomy as needed for decreased or absent pulses or respiratory compromise. 7. Wound Care Cover patient with a dry sterile sheet and tuck in to prevent hypothermia. Apply a thin layer of Silver Sulfadiazine to open burns if transport delayed by more than 12 hours. Consider debridement and application of topical antimicrobials if transfer to Burn Center is delayed beyond 24 hours. 8. Special Considerations for Chemical Burns Remove ALL clothing. Be careful to protect yourself. Brush powered chemicals off wound: then flush burns for a minimum of 30 minutes with running water. Irrigate burned eyes with a gentle stream of saline. Follow with an ophthalmology consult if transport is not imminent. 9. Special Considerations for Electrical Injuries Monitor distal pulses. Elevate burned extremities slightly. Cardiac monitor. Watch for burgundy colored urine. 10. Initial Laboratory tests (if available) Baseline studies: hematocrit, electrolytes, blood urea nitrogen, urinalysis, chest x-ray. Special studies as needed: arterial blood gas, carboxyhemoglobin, ECG, glucose.