Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
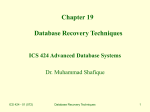
ADRENAL SUPPRESSION IN PEDIATRIC ASTHMA ADRENAL SUPPRESSION (AS) SYMPTOMS: ADRENAL SUPPRESSION (Patient may be asymptomatic) • Sustained deficiency of HPA axis following exposure to exogenous glucocorticoids can last from days to a year Glucocorticoid Deficiency • Malaise • Nausea • Headache • Poor growth • Consider after 2 or more weeks of glucocorticoid therapy (depends on the type, schedule of glucocorticoid administration and individual factors) • Poor weight gain • Hypoglycemia* • Hypotension* *Symptoms of adrenal crisis Mineralocorticoid deficiency (causing hypovolemia, hyponatremia and hyperkalemia) is NOT seen with AS (may be seen with other forms of primary adrenal insuffiency) COMPARISON OF THE VARIOUS ICS MEDICATIONS FATE OF INHALED STEROIDS P0TENTIAL SYSTEMIC SIDE EFFECTS • Adrenal suppression • Growth suppression • Cushingoïd features • Bone effects PK/PD CHARACTERISTICS OF ICS MEDICATIONS Particle size (µm) Fluticasone Budesonide Beclomethasone HFA Ciclesonide Lung deposition % Oral bioavailability % Protein binding % Clearance rates (Lh-1) 20 15-30 50-60 52 ≤1 11 20/40a ≤ 1/≤ 1a 90 88 87 99/99a 66 84 150/120a 152/228a 2.8 > 2.5 < 2.0 < 2.0 a = Active Metabolite SCREENING AND DIAGNOSIS OF AS WHEN TO SCREEN DIAGNOSIS BEST TEST • Symptoms (refer to table above) • Patients receiving high dose ICS (e.g. ≥ 500 mcg fluticasone ≥ 800-1200 mcg beclomethasone/budesonide) • Cortisol value < lab norm may indicate AS Consider endocrine consult • A normal non-stimulated cortisol does NOT rule out AS Note: Urinary cortisol is NOT a specific marker of AS • ACTH stimulation test >500 nmol/L normal in adults, >300 nmol/L normal in infants HOW TO SCREEN • Complete 8 am cortisol test • < lab normal – consider endocrine consult • within lab normal range – repeat every 6 months RULES FOR 8 AM TEST: • Must be done at 8 am or earlier • No oral steroids 48-72 hours before • No inhaled steroids the night before • Fasting not required PREVENTION AND RECOGNITION OF AS All PATIENTS ON ICS • Use lowest possible dose of ICS (regular re-evaluation) • Consider ICS with minimal systemic effects • Educate at risk patients and family on potential systemic side effects of ICS In children on high doses of ICS (e.g. ≥ 500 mcg fluticasone) screen & monitor for adrenal suppression every 6 months. Consider referral to endocrinologist IF abnormal screening test/growth. 1. Kelly HW. Comparison of inhaled corticosteroids: an update. Ann Pharmacother. 2009 Mar;43(3):519-27. 2. Gulliver T, Eid N. Effects of glucocorticoids on the hypothalamic-pituitary-adrenal axis in children and adults. Immunol Allergy Clin North Am. 2005;25(3):541-555, vii. 3. Derendorf H. Pharmacokinetic and pharmacodynamic properties of inhaled ciclesonide. J Clin Pharmacol. 2007;47(6):782-789.V Unrestricted Educational Grant provided by Nycomed Canada