Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
CLIN. CHEM. 24/10, 1744-1750(1978)
Determination of a Trivariate Reference Region for Free Thyroxine
Index, Free TriiodothyronineIndex, and Thyrotropinfrom Results
Obtained in a Health Survey of Middle-aged Women
BertH K#{226}gedal,
Arne Sandstrbm, and Gunnar Tibbling
We measured free thyroxine index, free triiodothyronine
index, and thyrotropin in serum in a community survey of
This was performed in connection with a gynecological health
survey carried out ina community of southern Sweden. Highly
the female population 39-60
abnormal results (outliers) were statistically eliminated and
the remaining values were used for calculation of reference
intervals for free thyroxine index, free triiodothyronine
index,
and thyrotropin.
Furthermore
a trivariate reference region
was developed to increase the diagnostic sensitivity of the
methods as discussed by Grams et al. (12) and Winkel et al.
(13).
method using Mahalanobis’
years old. A statistical
distance
was applied to the
data, to identify and eliminate highly abnormal values,
“outliers.” There was a small but statistically significant
increase in each of the three hormones with age. After
correction for age dependency,significant but rather small
correlationswere found between the hormones. The
material was used to calculate univariate reference intervals and a trivariate 0.95-tolerance region.
Materials and Methods
Population
reference values
thyroid disease
#{149}
sex- and age-related effects
statistics of “normality”
thyroid hormones
thyroid function . problem of outliers
AddItIonal
Keyphrases:
‘
The true incidence of thyroid disorders is difficult to establish. Most incidence figures given in the literature are obtained from diagnosis registers and may therefore underestimate the true value. From these studies, however, one may
conclude that the incidence of hyperthyroidism
is high in
middle and old age (1), and that there is a large preponderance
of females for both Graves’ disease (2-4) and toxic nodular
goiter(5, 6). Women are also affected more frequently with
spontaneous
hypothyroidism
than men, the prevalence in
women varying from 0.2 to 1.0% (1, 7, 8). Therefore, careful
studies on thyroid function of middle-aged women should be
of special interest.
For evaluation of the thyroid function, concentrations
of
thyroxine, triiodothyronine,
and thyrotropin in serum must
be determined. During recent years the variationof thyroid
hormone
concentrations
in serum in elderly people has been
but there are few reports on the corresponding
changes in middle age (40-60 years), although the incidence
of thyroid function disorders is high in this age category.
Menopause poses special problems in the interpretation
of
results because changes in ovarian function may affect the
concentrations
of proteins that bind thyroid hormones
studied
(9-11),
participate
in a gynecologic
health-screening
program.
Specimens of venous blood were drawn from the attending
4087 women, with the subjects seated, and the specimens were
sent to the laboratory. Serum was separated and stored at -20
#{176}C
until analyzed. In 202 individuals the venous puncture
failed or the volume of serum was insufficient for the analyses.
Complete data were obtained for 3885 of the women.
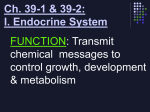
The age-distribution
of these women was very similar to
that for all the 5494 women living in the community (Figure
1)-i.e.,the attendance rate was similar in allage groups
studied.
Analytical
The aim of the present
variation
function
study was to evaluate the physio-
of some biochemical
variables
reflecting
in a population
of women 39 to 60 years old.
Departments ofClinical
Chemistryand ofMathematics,University
ofLinkoping,S-58185 Linkoping, Sweden.
Received May 17, 1978; accepted July 5, 1978.
1744 CLINICALCHEMISTRY,Vol. 24, No.10, 1978
Methods
The thyroxine concentration in serum was determined by
a competitive protein-binding
technique (14) with use of a
purifiedthyroxine-binding globulin fraction(15) as binder
insteadofthe serum from pregnant women used inthe original
method. The triiodothyronineconcentration in serum was
measured by radioimmunoassay
with a double-antibody
technique, with thimerosal
to displace triiodothyronmne from
thyroid hormone binding proteins (16). To separate the free
and bound fractions we used a swine antibody (Dacopatt8 A/S,
Denmark)
(11).
logical
thyroid
The women, all 39 to 60 years old except some who had been
examined by cytologicalsmear during the lastyear,livingin
the Motala township, County Ostergotland,
were invited to
directed
two methods
obtained
against
rabbit
IgG. As standards
in these
and L-triiodothyronine
Co., St. Louis, Mo. 63178.
uptake
test was performed
we used L-thyroxine
from Sigma
Chemical
The serum triiodothyronine
according to Nosslin (17). Pooled human serum from 100 male
blood donors was used as a reference standard and the results
for women were multiplied by the factor 1.05, to correct for
the sex-related difference in results.
Table 1. Reference Intervals for Free Thyroxine Index, Free Triiodothyronine index, and Thyrotropin
A.8
B.
a
Variable
No.
Mean
Free thyroxine index, nmol/l
Free triiodothyronine index, nmol/l
3885
3885
94.5
1.74
25.3
Thyrotropin, milli-int. units/tb
Free thyroxine index, nmol/l
Free triiodothyronine index, nmol/l
Thyrotropin, milli-int. units/I b
3885
3816
3840
3844
1.76
92.8
1.72
1.72
19.6
0.33
(A) Women 39-60 years old: (B) after univariate elimination of extreme values.
The thyroxine
concentration
in serum was adjusted
for the
influence
of variations
in thyroxine
binding globulin by calculating the free thyroxine index according to Clark and Horn
(18): (thyroxine
X triiodothyronine
uptake)/100.
Similarly,the freetriiodothyronineindex was calculated
as (triiodothyronine
X triiodothyronine
uptake)/100.
Thyrotropin
in serum was determined
by a double antibody
radioimmunoassay
(19). Antithyrotropin
(Calbiochem,
San
Diego, Calif. 92112) was used as the first antibody and a swine
antibody
to rabbit IgG (Dacopatts
A/S, Denmark)
as the
second.
As standard
obtained
detection
we used the human pituitary thyrotropin
68/38
from the Medical Research
Council, London. The
limit for the method
Lower values
merical value
Statistical
was 0.5 milli-int.
were for calculation
purposes
of 0.4 milli-int.
units/liter.
units/liter.
given
the nu-
Analyses
Women with abnormal thyroid function would give extreme
hormone values and should not be considered as belonging to
the healthy population. Moreover, extreme values could arise
from measurement
errors. For identification
of such outliers
(20) we used the principles described by Afifi and Azen (21).
They used the Mahalanobis’
(22) sample distance
for this
purpose. These calculations and the calculations of multiNariate reference regions (12, 13, 23) were performed with a
Univac 1108 computer and are described more in detail in the
Appendix. Calculations
of means, variances, standard deviations, and covariances as well as linear regression analysis
were performed according to standard methods
(24). The
theoretical
gaussian
distribution
curves
were calculated
from
12
10
B
E
=
4-
C
4-
2
39
41
43
45
47
49
51
40 42
44
46 48
50
52
53 55 57 59
54 56
58 60
Age, years
Fig. 1. Age distribution of the 3885 women studied (white bars)
comparedwith the 5494 women of the same age living In Motala
township (stippled bars)
The number of subjects In the subgroups of two years are given as percent of
total
b
SD
Reference Interval
43.9-145.1
0.40
0.94-2.54
0.40-7.74
53.6-132.4
-
1.06-2.38
0.44-6.74
-
After antlogarithmic transformation.
the obtained means, standard deviations, and number of
subjects, with the area under the gaussian curves set equal to
the area under the histogram.
The univariate
tervals were calculated
as the mean ±2 SD.
reference
in-
Results
Univariate Reference Intervals
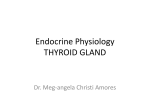
Figure
2 shows the distributions
roxine index, free triiodothyronine
all subjects studied.
free triiodothyronine
The results
of results
for the free thy-
index, and thyrotropin
for free thyroxine
index
for
and
index approximated
a gaussian distribution, although a few individual results deviated markedly
from the main group. On the other hand, the distribution
for
thyrotropin
was positively skewed but became more symmetrically
bell-shaped
after logarithmic
transformation.
Also
in thiscase a small number of outlying results were observed
(Figure 2d).
Reference
intervals
for the three hormones
were first calculated as mean ±2 SD from all results (Table 1). As already
mentioned, the material included a number of outliers, which
must be expected to influence the reference intervals. These
outliers were then identified as described in the Appendix.
There were few outliers, and they were evenly distributed
among the three hormone variables and amounted to 69(1.8%)
in case of the free thyroxine index, 45 (1.2%) in case of free
triiodothyronine
index,
and 41 (1.1%) for thyrotropin.
How-
ever, one woman had outlying results for all the three hormones, 20 women had outlying values for two hormones, and
112 women for one hormone,
giving a total of 133 women
(3.4%) with one or more values as outliers.
After the outlier values were eliminated, we recalculated
the reference intervals. As shown in Table 1, the widths of the
reference intervals were now markedly smaller and the distribution was more nearly gaussian (Figure 2). Besides the
women with outlying values there were additionally
520
women (13.9% of the remaining 3752 subjects) with one or
more values beyond the reference intervals. The number of
results outside the reference intervals for each hormone
variable was 172 (4.6%) in the case of the free thyronine index,
165 (4.4%) in the case of the free triiodothyronine
index, and
243 (6.5%) for thyrotropin.
Of the subjects there were seven
women for whom all three hormone values were beyond the
reference intervals, 46 women with two values beyond, and
467 women with one value beyond. Thus the total number of
hormone values outside each of the reference intervals was
close to the expected 5% and the total number of women with
one or more values outside the reference intervals (13.9%) was
close to the figure of (1 - 0,95) X 100 = 14.3%, the expected
proportion
for combinations
of three uncorrelated
variables.
Trivariate
Reference
Region
In clinical chemistry, reference intervals (normal values)
are often defined as an estimated 0.95-tolerance
interval obtained from results from healthy individuals (25). Analogous
to the univariate 0.95 interval, we want to calculate a trivariate
CLINICALCHEMISTRY,Vol. 24, No.
10, 1978
1745
a
800
C
800-
‘1
600
400
E
Z
‘
200
-
400
200
0
0-
0
50
100
150
Free thyroxine
200
index,
-,
0
250
2
4
6
10
12
14
16
18
20
Thyrotropin, mU/l
nmol/l
1200
b
800
8
-
d
1000
800
600
600
400
j
I
200
400
200
0
0
1.0
2.o
Free triiodothyronine
3.o
I
4.o
-1.6
0
-0.8
index. nmol/ I
0.a
1.6
elog
Fig. 2. Distribution ofresults
for(a)freethyroxine Index, (I)) free triiodothyronlne index,
the 3885 women
(C)
I
2.4
3.2
4.o
4.8
tltyrotropin
thyrotropin, and (d) log thyrotropin for
The theoretical gaussian cirves calculated from the total ntmiber of subjects and the mean and standard deviation before (dotted line) and after (solid line) elimination
of outliers are compared with the histograms for free thyroxine index, free triiodothyronine index, and log. thyrotropin from the sample population
reference region also containing 95% of the material. Outliers
were now identified trivariately
by simultaneously
taking free
thyroxine index, free triiodothyronine
index, and loge thyrotropin into account as described in the Appendix. This procedure identified the set of values from 108 women (2.8%) as
outliers. After elimination of these values, the outlier-free
material was used to calculate a trivariate reference region.
For calculation of multivariate
reference regions the covariances between the variables are used in addition to the
means and variances. Before the correlations
between the
hormones were studied, we had to look for any significant
intercorrelations
of the hormones with age, and, in fact, found
such correlations. Simple regression analysis of the hormone
variables on age was therefore performed using the outlier-free
3777 women. The resulting linear equations and correlation
r, were as follows:
coefficients,
Free thyroxine
index
=
66.7 + 0.52
X age (r
Free triiodothyronine
Loge thyrotropin
=
index
=
0.165, P <0.001)
1.33 + 0.0078
X age (r = 0.147, P <0.001)
0.112 + 0.0091
X
The results
=
were then
age (r
=
0.081, P <0.001)
normalized
to the age of 50 years by
lines (see Appendix).
The co-
application of the regression
variances between the hormones were then calculated and in
each case there was a small but statistically significant correlation (Table 2). As expected, a positive correlation was
obtained between free thyroxine index and free triiodothy-
Table 2. VarIances and Covariances for the Variables Shown, After Trivariate Elimination of Outliers
and Transformation of Data to Correspond to the Age of 50 Years
Mean
Variable
Free thyroxine Index
Free trliodothyronine Index
Loge thyrotropin
Variables
Free thyroxine
92.8
1.72
0.569
Covarlance
Index, free
trllodothyronine Index
Free thyroxineIndex, loge thyrotropin
Free triiodothyronlne index, Ioo, thyrotropin
1740 CLINICALCHEMISTRY,Vol. 24, No. 10, 1978
1.481
-2.551
-0.021
Variance
363
0.102
0.474
r
0.244
-0.194
-0.094
SD
19.1
0.32
0.69
P
<0.001
<0.001
<0.001
0
2
4
6
8
10
12
14
16
02
Fig. 3. Cumulative distribution of D2
From the 95th percentIle a 02-vaiue of 8.49 was obtained. For comparison, the
theoretical cumulative x2-dlstributlon with three degrees of freedom is shown
(smooth curve)
ronine index, and negative correlations between thyrotopin
and each of the thyroid hormones. The means and variances
for each of the normalized hormone variables were very similar
to the values obtained after univariate elimination of outliers.
A trivariate
reference
region can now be described
by the
squared Mahalanobis’
distance, D2. It may be noted here that
D represents
the three-dimensional
distance between a point
defined by a set of hormone values and the point described by
the mean values (Table 2) for the three hormones. D2-values
were now calculated from the hormone results for all the
subjects and were arranged as a cumulative
distribution
(Figure 3). From this distribution
a D2-value corresponding
to the 0.95 tolerance
interval was determined
and obtained
as 8.49. The reference interval for D2 was thus 0-8.49. The
trivariate
reference
region is represented
by an ellipsoid
(Figure 4) where each point on its surface has D2 = 8.49. Points
giving D2-values of less than 8.49 are located within the elip-
soid and the corresponding
hormone results are considered
normal. On the other hand, points with D2-values exceeding
8.49 are located outside the reference ellipsoid. This was found
in 188 subjects
from the outlier-free
material.
Discussion
When reference values are calculated from results obtained
in a health-screening
program, the problem of outliers arises.
The sample population
should consist mostly of healthy
subjects, but the risk that it also includes diseased subjects
must
not be neglected.
Furthermore,
improper
sample
col-
lection and analytical errors may result in experimentally
determined values that are not representative
for the population studied.
All such aberrant
values may be called “outliers.” Obviously, they must be eliminated from the population
sample before reference
intervals
are calculated.
An outlier may be identified from the fact that it lies well
outside the boundaries of the main sample population.
If this
population
is normally
distributed
and univariate,
its
boundaries
can with a certain
statistical
significance
be de-
scribed by its mean and standard deviation. Outliers may then
be defined as values that differ from the mean with a value
larger than a certain multiple of the standard
deviation.
The numerical value that should be given to the multiplier
is a matter of dispute. In connection with quality-control
programs applied to clinical laboratory results, the values 2
or 3.5 are used (26,27). In other quality-control
programs the
calculations are made with a value of 3 (28, 29), and even a
value of 10 has been suggested (29). Burnctt (30), on the other
hand, claimed that the multiplier should increase with the
number
of observations
in the sample.
Besides
the confusion
Fig. 4. ComparIson between the triple univarlate reference region, the rectangular box with univariate Intervals, and the tnvariate reference region
The ellipsoid has the equation D2 = 0.00302 (x1 - 92.8)2 + 10.5 (x2 - 1.72)2
+ 2.20 (x3 - 0.569)2 - 0.0822 (x1 - 92.8) (x2 - 1.72).+ 0.0289 (x1 - 92.8)
(x3 - 0.569) + 0.465 (x2 - 1.72) (x3 - 0.569), where 02 = 8.49
which exists concerning the numerical value of the multiplier
there is another drawback with this technique. It cannot be
applied multivariately, and another statistical approach must
then be used. For this purpose we used the Mahalanobis’
distance (22), which is a statistical concept describing the
distance between two populations
(31). It has not been used
in clinical
chemistry forthe purpose of outlier identification,
although its application
to the establishment
of reference
regions (12, 13) and in connection with discriminant
analysis
(32) has been described.
When outliers were identified by a triple univariate evaluation of the data, 133 women with outlying results were found.
This isa higher number than the corresponding value of 108
obtained
by trivariate
evaluation
of the data. This difference
may partly be attributed to the fact that the risk factor chosen
for misclassification
of an inlier as an outlier is used three
times in the univariate evaluation and the total risk is therefore higher than if the univariate evaluations were performed
simultaneously for the three variables as in the trivariate case,
and partly it may be due to the fact that in the trivariate case
attention is also paid to the correlation between the variables.
Outliers have been further studied with the aid of cluster
analysis and have been allocated to different disease states.
These results will be reported in a forthcoming paper.
It is of interest to compare our results with those recently
reported
from a health survey in Great Britain (8,33). In this
study a largerrange for age was used and the study included
both men and women, but the number of cases in each age
group was smaller. The results of the thyroid hormones were
not adjusted for variations in thyroid-hormone
binding proteins, but subjects on drugs that were known to affect the
thyroid function tests and those who were pregnant or had any
marker of thyroid disease were excluded. In spite of the differences in the way their study and ours were done, the results
were quite similar, both with respect to concentration
levels
and the distributions
of hormone values. We calculated the
free thyroxine
index and free triiodothyronine
index as
products of the respective thyroid hormone concentrations
and the serum triiodothyronine
uptake test. Since the latter
has a normal mean value of 100% (male blood donors) the
numerical value of the free thyroxine index and the free tniodothyronine
index will give mean results close to the determined values of thyroxine and triiodothyronine.
The reference intervals for serum thyroid hormones vary in the litCLINICAL
CHEMISTRY. Vol. 24, No. 10, 1978
1747
erature.
The values we obtained
are neither extremely
low or
high and are similar to the values given by Evered et al. (33).
Also, a similar increase of the hormones
with increasing
age
was observed
for the women of comparable
ages as in their
study. As can be seen from Figure 2 there was a tendency
to
leptokurtic distribution of log thyrotropin.
However, from a
practical point of view we accepted gaussian statistics
for
calculation of the univariate reference intervals. The results
agree well with recently published reference values (33, 34).
After adjusting the hormone data for age variations, we
found positive correlations between free thyroxine index and
free triiodothyronine
index and negative correlations between
the serum concentrations
of thyrotropin
and the respective
thyroid hormone concentrations.
The correlation coefficients
were low but statistically significant. Perhaps many results
are needed to establish significant correlations, and this may
explain why others found no correlations
in healthy controls
(10, 35).
If the hormone variables were gaussian distributed,
the
univariate reference interval, calculated as the mean ±2 SD,
should include 95% of a healthy population (25). Such results
were obtained in the present investigation.
The univariate
combination of three variables, each with 0.95 reference intervals will, however, include only #{216}#{149}953
X 100 = 85.7% of the
healthy population
if the hormones are uncorrelated.
Correlations between the variables would increase this figure, but
the correlations we found were small and consequently
our
observed value 86.1% was close to the theoretical 85.7%.
No trivariate reference region for thyroid hormones and
thyrotropin
has been published earlier. A geometric interpretation of the reference region described by triple univariate
reference intervals is shown in Figure 4. It is represented
by
a box in which the values for 86.1% of all normal individuals
will be located; 13.9% will be outside the box. The same figure
also shows a three-dimensional
representation of the trivariate
reference region, which is an ellipsoid containing (by definition) 95% of the healthy individuals. It may be noted here that
of the total material (including outliers) there were 653 individuals with values outside the triple univariate reference
region and there were 296 individuals
with values outside the
trivariate
reference region (ellipsoid). Of the individuals
outside the box there were 360 individuals inside the ellipsoid
and of the individuals outside the ellipsoid there were three
women with values inside the box. Although the trivariate
reference region (ellipsoid) thus classified considerably fewer
subjects as abnormal, a small number of subjects were on the
other hand classified as abnormal by trivariate evaluation but
as normal by triple univariate evaluation.
From the foregoing discussion it is evident that tnivariate
evaluation of the hormone results offers considerable
advantages in comparison with the triple univariate evaluation,
mostly because the number of normals misclassified as abnormals will be decreased. Although the calculations of D2 (see
legend to Figure 4) necessary for a trivariate evaluation of
patient data may appear too cumbersome for use in clinical
routine, they are in fact easily performed with a programmable
desk-top calculator.
This study was supported by a grant from the Swedish Board for
Technical Development,
project number 77-4380, II. Excellent
technical assistance was given by Miss Anita Pettersson.
Appendix
I. Age-corrected Variables
Notations:
x 1’
=
=
1748
free thyroxine index
age-corrected free thyroxine
CLINICAL CHEMISTRY,
index
Vol. 24, No. 10, 1978
free triiodothyronine
index
age-corrected free tniiodothyronine
= loge thyrotropin
x3 = age-corrected
loge thyrotropin
b = subject’s age in years
X‘
=
index
=
The hormone values were transformed
regression
according to the linear
line to the age of 50 years by using the equations
x1’ + 0.522 (50-b)
=
X2 =
x2’ + 0.00775
(50-b)
=
x3’ + 0.00914
(50-b)
II.Segregation of Outliers
Notations:
n
=
p
=
the number of observation vectors
the vector dimension (number of variables)
= the ith p-dimensional
observation vector; x
., x,,3.
i = 1, 2,
n.
= the p-dimensional
mean vector; X,t =
i,..
When , is calculated, x is excluded.
= the transponate
of x
...,
S1
=
the p’p-dimensional,
[
tnix.
positive
Q2
ii
=
definite
-
C
=
(x1,, x2,
covaniance
., 1,,,).
ma-
C
J12
S11
Si
Si1
S,
-
x is excluded in the calculation
of the variances
and covariances.
D2 = the sample Mahalanobis distance between x and i;
D
n-k-i
T
k
j
F
(x1
-
S’ (x1 -
.)t
.
D follows Hotelling
=
n-k
the number
=
=
of outliers that are segregated
step in the iterative
segregation
1, 2,
iterative
m
(m
...,m, where
=
procedure
=
procedure.
the total number
n).
(n-k-1-p)(n-k-i)
=
(n
and (n
-
Segregation
,
k -2)
- k -
s T2-distnibution
p (n
1 -
-
k)
.
up to the jth
of steps in the
D is F-distributed
with p
p) degrees of freedom.
procedure:
The n observation vectors are arranged in a random ordered
list. For the first vector, the sample Mahalanobis
distance D
is calculated.
If the above
F
(n_l-p)(n-l)D2
1
(n-2)pn
1
is greater than the tabulated
F with p and (n - 1- p) degrees
of freedom and a pre-assigned risk level a, the observation
vector is segregated from the set of vectors, and it is classified
as an “inlier.” The risk level a, of misclassification
an inlier
as an outlier was set to 0.001 as a reasonably low risk level.
The sample Mahalanobis
distance is then computed
for the
next vector. An F-test is made and the result gives outlier or
inlier classification of the second vector. The procedure will
continue in m steps (m n). After m steps all nonsegregated
vectors have been tested once without any vector being segregated.
Because
of probability
difficulties
when first
choosing a simultaneous risk level a8, and from that computing
simple conditional risk levels, a3, j = 1,.
m, we make the
..,
approximation
that all the a3’s are equal
to 0.001.
In the univariate
case, the test statistic
n-k
which follows Student’s
to a, which
was set
is
s
t -distribution
with n
-
-2 degrees
k
of freedom.
x1,
-
______
.
-
(xj-xj)2,IJ.
n-k-i
n-k-2
Ill.Reference
Regions
In the single-variate case, the reference
containing95% of the sample population,
region is an interval
here calculated
as
± 2 SD. The bivariate
reference
region is an area also containing 95% of the sample population
and is calculated
from
the joint density function from the two variables.
If the variables are jointly normal distributed
the area will be described
by an ellipse. In the same manner the three-dimensional
reference region will be described
by the ellipsoid equation,
D2
(x1
=
-
S’ (x4 -
)t
where the mean vector and the covariance
matrix are calcu-
lated from the outlier-free
observation
vectors. The reference
volume was defined to contain 95% of the outlier-free
observations.
The values for D2 were therefore
arranged
in increasing order, and the 95 percentile
was defined (D95). All
vectors with D2 < D95 will then be located inside the ellipsoid.
The algebraic expression for the ellipsoid is calculated by
using
x1
the following
notations:
is the age-corrected
free thyroxine
x2 is the age-corrected
x3 is the age-corrected
=
index
free triiodothyronine
loge thyrotropin
index
X2, X3)
(ii,
r2
I S1
S12
Sj3
S3
S
S12
I
Ls13
is the sample variance, i
s is the sample covariance,i,
s
1, 2, 3.
= 1, 2, 3; i #
=
j
j
abc
S’
The elements
b d
cef
of the inverted
e
18. Clark, F., and Horn, D. B., Assessment of thyroid function by the
combined use of serum protein-bound
iodine and resin uptake of
‘311-triiodothyronine.
J. Clin. Endocri not. 25, 39 (1965).
19. Odell, W. D., Wilber, J. F., and Paul, W. E., Radioimmunoassay
of thyrotropin in human serum. J. Clin. Endocri not. Metab. 25,1179
matrix are:
2
=
23
5j3 -
S3 S12
(1965).
u
d=51S3
U
2 2
s13
2
12
f._5152
u
c=
12 23
e
12
=
S 513
533 - S 23
U
where
u
s s s + 2s12
=
The ellipsoid
D2
=
a(x1
-
-
5j3 23
in then calculated
)2
+ d(x2
+ f(x3
+ 2c(x1
-
-
-
s? 23
11)(x3
-
S
513
-
S
512
as
2)2
x3)2 + 2b(xj
-
7)
+
1. BUrgi, H., and Labhart, A., VI. The thyroid gland. In Clinical
Endocrinology,
Theory and Practice, A. Labhart, Ed., SpringerVerlag, New York, Heidelberg, Berlin, 1974, pp 135-283.
2. Furszyfer, J., Kurland, L. T., McConahey, W. M., and Elveback,
L. R., Graves’ disease in Ohnsted County, Minnesota, 1935 through
1967. Mayo Clin. Proc. 45,636 (1970).
3. Furszyfer, J., Kurland, L. T., McConahey, W. M., et al., Epidemiologic aspects of Hashimoto’s thyroiditis and Graves’ disease in
Rochester, Minnesota (1935-1967), with special reference to temporal
trends. Metabolism 21, 197 (1972).
4. R#{216}nnov-Jessen,V., and Kirkegaard,
C., Hyperthyroidism-a
disease of old age? Br. Med. J. 1,41 (1973).
5. Horst, W., ROsIer, H., Schneider, C., and Labhart, A., 306 cases of
toxic adenoma: Clinical aspects, findings in radiochromatography
and
histology, radioiodine diagno8tics, results of I13i and surgical therapy.
J. NucI. Med. 8, 515 (1967).
6. PohI, G., Galvan, G., Steiner, H., and Salis-Samaden,
R., Das autonome Adenom der Schilddr0se un Struma.Endemie-Gebiet. Dtsch.
Med. Wochenschr. 98, 189 (1973).
7. Gordin, A., Heinonen, 0. P., Saarinen, P., and Lamberg, B.-A.,
Serum thyrotropin in symptomless autoimmune thyroiditis. Lancet
i, 551 (1972).
8. Tunbridge, W. M. G., Evered, D. C., Hall, R., eta!., The spectrum
of thyroid disease in a community: The Wickham survey. Clin. Endocrinol. 7, 481 (1977).
9. Herrmann, J., Rusche, H. J., Kroll, H. J., et al., Free triiodothyronine (T3)-and
thyroxine (T4) serum levels in old age. Horm.
Metab. Res. 6, 239 (1974).
10. Bermudez, F., Surks, M. I., and Oppenheimer, J. H., High incidence of decreased serum triiodothyronine
concentration in patients
with nonthyroidal
disease. J. Clin. Endocrinol.
Metab. 41, 27
(1975).
11. Hesch, R.-D., Gatz, J., Pape, J., eta)., Total and free triiodothyronine and thyroid-binding
globulin concentration in elderly human
persons. Eur. J. Clin. Invest. 6, 139 (1976).
12. Grams, R. R., Johnson, E. A., and Benson, E. S., Laboratory data
analysis system: Section IlI-Multivariate
normality. Am. J. Clin.
Pat hot. 58, 188 (1972).
13. Winkel, P., Lyngbye, J., and Jorgensen, K., The normal region-a
multivariate problem. Scand. J. Clin. Lab. Invest. 30, 339 (1972).
14. Seligson, H., and Seligson, D., Measurement
of thyroxine by
competitive protein binding. Clin. Chim. Acta 38, 199 (1972).
15. Penky, J., and Marshall, J. S., Studies on thyroxine-binding
globulin (TBG) II. Separation from human serum by affinity chromatography. Arch. Biochem. Biophys. 135, 304 (1969).
16. Gharib, H., Ryan, R. J., Mayberry, W. E., and Hockert, T., Radioimmunoassay
for triiodothyronine
(T3): I. Affinity and specificity
of the antibody for T3. J. Clin. Endocrinol.
33,509 (1971).
17. Nosslin, B., A simplified technique
for the triiodothyronine
test
(T3 test) with Sephadex. Scand. J. Clin. Lab. Invest. 17, Suppl. 86,
177 (1965).
covariance
b
References
11)(x2
2e(x
-
-
x2)
2)(x3
-
x3)
20. Anscombe, F. J., Rejection of outliers. Technometrics
2, 123
(1960).
21. Afifi, A. A., and Azen, S. P., Statistical Analysis. A Computer
Oriented Approach, Academic Press, New York, 1972.
22. Mahalanobis, P.C., (hi the generalized distance in statistics. Proc.
Nati. Inst. Sci. India 2 (1), 49 (1936).
23. Harris, E. K., Effects of intra-and inter-individual
variation on
the appropriate use of normal ranges. Clin. Chem. 20, 1535 (1974).
24. Snedecor, G. W., and Cochran, W. G., Statistical Methods. Iowa
State University Press, Ames, Iowa, 1973.
25. Alstrom, T., GrSsbeck, R., Hjelm, M., and Skandsen, S., Recommendation concerning the collection of reference values in clinical
chemistry and activity report. Scand. J. Clin. Lab. Invest. 35,SuppL
144, 1 (1975).
26. Stromme, J. H., and Eldjarn, L., Surveys of the routine work of
CLINICAL CHEMISTRY,
Vol. 24, No. 10, 1978
1749
clinical chemical laboratories in 116 Scandinavian hospitals. Scand.
J. Clin. Lab. Invest. 25, 213 (1970).
27. Bowers, G. N., Burnett, R. W., and McComb, R. B., Preparation
and use of human serum control materials for monitoring
precision
in clinical chemistry. Clin. Chem. 21, 1830 (1975).
28. Whitehead, T. P., Browning, D. M., and Gregory, A., A comparative survey of the results of analyses of blood serum in clinical
chemistry laboratory in the United Kingdom. J. Clin. Pat hot. 26,435
(1973).
29. Schork, M. A., Greenhouse, J. B., and Williams, G. W., Normality
and other statistical considerations
as they relate to selected quantitative
measures
in the CAP survey. Am. J. Clin. Pathol. 68, 112
(1977).
30. Burnett, R. W., Accurate estimation of standard deviationsfor
quantitative methods used in clinical chemistry. Clin. Chem. 21,1935
(1975).
1750
CUNICAL
CHEMISTRY,Vol.24.No. 10. 1978
31. Rao, C. R., The use and interpretation
of principal component
analysis in applied research. Sankhya, Ser. A 26,329(1964).
32. Solberg, H. E., Skrede, S., and Blomhoff, J. P., Diagnosis of liver
diseases by laboratory results and discrinunant analysla Identification
of best combinations of laboratory tests. Scand. J. Clin. Lab. Invest.
35, 713 (1975).
33. Evered, D. C., Tunbridge, W. M. G., Hall, R., et al., Thyroid
hormone concentrations in a large scale community survey. Effect of
age, sex, illness and medication. Clin. Chirn. Acta 83,223 (1978).
34. Gordin, A., and Saarinen,
dioimmunoassay
of human
P., Methodological study of the rathyrotropin.
Acta Endocrinol.
71, 24
(1972).
35. Transbol, I., Christiansen,
C., and Baastrup, P. C., Endocrine
effects of lithium. I. Hypothyroidism,
its prevalence in long-term
treated patients. Acta Endocri not. 87, 759 (1978).