Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
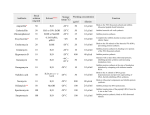
Drug Main action Side effects Notes Neuromuscular blocker: -Curare -D-Tubocurarine (the reactive gradient of Curare) Block cholinergic transmission (Ach). So they’re used in: Surgeries, Intubation, ECT, ICU and orthopedic procedures. -Histamine release - Bronchoconstriction and ↑ Mucus secretion. - ↑HR. -Hypotension. - Ganglion blockade. - Non-depolarizing blockers. - Competitive (antagonists). - To reverse their action we ↑ Ach by giving AchE inhibitor. - Given IV. - Doesn’t penetrate membranes or BBB. - Excreted unchanged. - Calcium channel blockers and aminoglycosides enhance their action. - Depolarizing blocker. - Agonist that leads to desensitization of the receptor. - Doesn’t respond to AchE. -Short onset of action. - Given IV. - Doesn’t penetrate membranes or BBB. - Excreted unchanged. - Given orally except Dantroline is given IV in the urgent situations. Neuromuscular blocker: - Succinylcholine “suxamethonium” Block cholinergic transmission (Ach). So they’re used in: Surgeries, Intubation, ECT, ICU and orthopedic procedures. - Hyperkalemia. - Malignant Hyperthermia (we use IV dantroline to reverse this). - Post-operative pain. Spasmolytic drugs: On CNS: Diazepam (facilitate GABA) Baclofen (GABA agonist) Tizanidine (Reinforce) On skeletal muscle: Dantroline (Ca+2 blocker) DMARD aka SAARD: Methotrexate Cerebral palsy. Multiple sclerosis. Stroke with spasms. - GI effects. - Sedation. - RA and Psoriatic arthritis - Antineoplastic - Immunosuppression -GI effects -Mouth ulcers, Stomatitis -Leucopenia -Hepatotoxicity -Teratogenic - Low doses, once weekly. - Cotrimoxazole has synergistic effect with it -NSAID increase its elimination -4-6 weeks for its effect Chloroquine and Hydrochloroquine - Antimalarial - Slow the progression of RA -GI effects -Blurring vision -Urticaria -Hemolysis -Given in combination with NSAID or Methotrexate Sulfasalazine - RA - Ulcerative colitis -Hemolytic anemia -Infertility - 2-3 months for its effect - More toxic than Methotrexate - Used in refractory cases TNF inhibitors: Entanercept Infliximab - Moderate to severe RA - Immunosuppression so the body is prone to infections - Combined with methotrexate - Antibiotic and vaccinations are given with it Acetaminophen (paracetamol) - Early RA to decrease pain “analgesic and antipyretic” - Poison Ivy - Toxic in high doses. - N-acetylcysteine is the antidote NSAIDs Ex: aspirin - RA “analgesic, antipyretic and anti-inflammatory” - LT (Zafrilukast) inhibitor are given with it in asthmatic patients (any allergy, ex: Urticaria). - Celecoxib are used instead of NSAID in patients with peptic ulcer Bacitracin - staph aureus infections - +ve bacteria -GI effects -Peptic ulcers - no ptt aggregation - PDA closure - Asthmatic patients worsening - Reye’s syndrome “only with aspirin” - When it’s used systemically it has side effects - rarely cause hypersensitivity Polymyxin B - -ve bacteria - side effects “systemically use” - Inhibits membrane synthesis Neomycin and Gentamycin - gram negative aerobes and some anaerobes *was not mentioned* - ototoxicity and nephron toxicity “systemically use” - May cause hypersensitivity - Topical - Oral in GI infections - Inhibits proteins synthesis Neosporin = Bacitracin + polymyxin B + Neomycin - wide spectrum: gram positive, negative and anaerobes Benzoyl Peroxide - First line in mild cases of Acne Salicylic acid - First line in mild cases of Acne - Chemical burns - Metabolite of aspirin - MOA: 1- decrease inflammation 2- Keratolytic Retenoids Topical: Tezarotene and adapalene Systemic: Isotretinoin - First line nowadays in Acne - Also used in Psoriasis Topical: teratogenic “not a concern” Systemic: Teratogenic and cause chelitis - Vit.A analogue - Control epithelial cells growth - Ointment/ Topical - inhibits cell wall synthesis - No resistant against it - Used in combination with antibiotics Tetracycline: Minocycline and Doxycycline Clindamycin - Acne - Discoloration of teeth and bone - Don’t give it to children - Given orally -Acne - Anaerobic bacteria - pseudomembranous colitis - Topical Erythromycin -Acne Azoles: Imidazoles *bad drugs* ex: Ketoconazole Triazoles *most common* ex: fluconazole+ itracon- - Against fungal infections Allylamines: naftifine terbinafine. - Onychomycosis - MOA: inhibits ergosterol synthesis Nystatin - Against fungal infections - Attacks ergosterol directly Griseofulvin - Against fungal infections - Inhibits mitosis Acyclovir Penciclovir - Against viral infections. - Inhibits viral replication. - Has low bioavailability so it’s found as creams - Can be given orally Premethrin - DOC in parasitic infections “first line” - Apply before going to bed for about 14 hours. Lindane - Second line in parasitic infections Rifampicin - Leprosy treatment - Once a month Dapsone - Leprosy treatment - Once daily Clofazimine - Severe cases of leprosy Topical Corticosteroids: Hydrocortisone -Psoriasis -Eczema -Poison Ivy *in severe cases we use systemic* -Bites - Burning sensation - Adrenal gland suppression - Atrophy of the dermis and epidermis - Hypopigmentation - Steroid acne - Anti-inflammatory - Anti-proliferation - immunosuppression Vit.D analogues: Calcipotriene, calcitriol - Psoriasis - Hypercalcemia - Inhibits epidermal proliferations - Stimulates differentiation - Given with benzoyl peroxide - Staphcoccus is resistant to it - Imidazoles disrupts steroids synthesis - Neurotoxic - Can be given orally - MOA: inhibits ergosterol synthesis - Found in shampoos and lotions PUVA - Psoriasis Immuno-modulator: Tacrolimus - Eczema Antihistamine first generation: Diphenhydramine Chlorpheniramine (Allerfin) Hydroxyzine Promethazine Antihistamine second generation: Loratadine Cetirizine - Relax eczema patients -Skin cancer - Effusions - Sedation *it’s a SE but it’s why I use it in eczema* - Urticaria - Peptic ulcer - Bites ,مجد بن الهيثم .النادي الطبي