Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
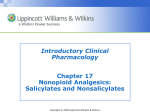
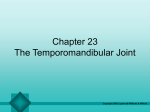
Chapter 19 The Pelvic Floor Copyright 2005 Lippincott Williams & Wilkins Anatomy and Kinesiology Skeletal Muscles Superficial 1. Anal sphincter – Provides fecal continence. 2. Superficial perineal muscles – Aid in sexual function. 3. Urogenital diaphram – Part of continence mechanism. Deep 4. Pelvic diaphragm – Coccygeus assists to stabilize sacrum, levator ani muscles support pelvic viscera. Copyright 2005 Lippincott Williams & Wilkins Pelvic Floor Muscles Copyright 2005 Lippincott Williams & Wilkins Related Musculature Copyright 2005 Lippincott Williams & Wilkins Pelvic Floor Function 1. Supportive – Supports pelvic organs. 2. Sphincteric function – Provides closure (via slow twitch fibers) of urethra, vagina, and rectum. 3. Sexual function – Pelvic Floor Muscles (PFMs) provide proprioceptive sensation. Copyright 2005 Lippincott Williams & Wilkins Physiology of Micturition Physiologic process of urination and involves complex set of somatic and autonomic reflexes. PFMs and detrusor muscle coordinate activity upon bladder filling. Urgency increases as bladder fills. PFMs relax and detrusor contracts, urine flows out, and PFMs then return to resting levels. Copyright 2005 Lippincott Williams & Wilkins Anatomic Impairments 1. Birth injury – Tear, overstretch, crushing of PFMs 2. Neurologic dysfunction – Disk herniation, spinal cord injury (SCI), diabetes, radical pelvic surgery, CNS disease Copyright 2005 Lippincott Williams & Wilkins Psychological Impairments Motivation – Perception of disability WRT incontinence varies across patients. Sexual abuse – Higher incidence of incontinence and pelvic pain. Knowledge of symptoms (low selfesteem, self-mutilation, etc.) is crucial! Copyright 2005 Lippincott Williams & Wilkins Examination/Evaluation Risk Factors – Screening Questionnaires Brief 1. 2. 3. Do you ever leak urine or feces? Do you ever wear a pad because of leaking urine? Do you have pain during intercourse? Affirmative responses to these questions directs practitioners to use a more detailed questionnaire. Copyright 2005 Lippincott Williams & Wilkins Screening Questionnaires – Detailed The more detailed questionnaire is administered to patients with pelvic, back, or hip pain who are recovering slower than expected. Affirmative answers to the detailed questionnaire can distinguish patients with: supportive dysfunction stress incontinence urge incontinence organ prolapse hypertonia, incoordination, obstruction, urinary retention Copyright 2005 Lippincott Williams & Wilkins Results of the Internal Exam Muscle performance (including power and endurance) Resting tone between contractions Coordination Trigger points, sensory impairment, scars, adhesions Internal exams are contraindicated in some cases (pregnancy, etc.) Copyright 2005 Lippincott Williams & Wilkins Therapeutic Exercise Interventions for Common Impairments Impaired Muscle Performance Pelvic floor muscles – Treatment is active Pelvic Floor Exercises (PFEs). Abdominal muscles – Patient is taught not to “bear down.” Focus on lumbopelvic core. Hip muscles – Piriformis, obturator internus, and hip adductors, often underlying hypertonus of PFMs. Copyright 2005 Lippincott Williams & Wilkins PFEs Dosage – Based on principles of overload and specificity Duration – Progress to 10-second contractions Rest – Work:rest, 2:1, graduate to 1:1 as quality and endurance improve Copyright 2005 Lippincott Williams & Wilkins PFEs Slow twitch muscle repetitions Individualize dosage. Starting 3 sec/5–10 reps. Fast twitch muscle repetitions Contractions are held less than 2 seconds. Sets Several times throughout the day. 30–80 contractions per day. Copyright 2005 Lippincott Williams & Wilkins Activity Posture – Graduate exercises from horizontal to standing and functional activity. Accessory muscle use – Eventually, patients should learn to contract PFMs without accessory muscles (abdominal muscles, adductors, etc.). Patient education – Location, function, and importance of PFMs should be explained. Copyright 2005 Lippincott Williams & Wilkins Patient Education Kegel Exercises: 1. Supportive – Hold pelvic organs in. 2. Sphincteric – Stop urine, feces, gas from escaping until reaching the toilet. 3. Sexual – Increase sexual feelings for women and men, assist men in maintaining erection. Copyright 2005 Lippincott Williams & Wilkins Sample Exercise Prescription Duration of ST contractions (5 sec) Rest between ST contractions (10 sec) Repetitions of ST contractions (5 times) Repetitions of FT contractions (10 times) Sets per day (4–6) Position (gravity eliminated) Accessory muscle use (not at this time) Copyright 2005 Lippincott Williams & Wilkins Pain PFMs – Treatment should focus on normalizing tone. – Manual soft tissue manipulation – Surface EMG feedback – Electrical stimulation, ultrasound, hot or cold on the perineum to treat spasm Copyright 2005 Lippincott Williams & Wilkins Role of Hip and Trunk Muscles in Pelvic Pain Trigger Points Adductors, PFMs, obterator internus, piriformis, iliopsoas, abdominal Soft tissue mobilization, modalities, therapeutic exercise for stretching, strengthening, and patient education regarding body mechanics and postures Copyright 2005 Lippincott Williams & Wilkins Joint Mobility and ROM Spasm of PFMs is often related to lumbopelvic mobility impairments. – SI, pubic symphysis hypo/hypermobility may cause secondary impairment of PFM hypertonus. – Unilateral PFM spasms may perpetuate pelvic joint mobility impairments. Copyright 2005 Lippincott Williams & Wilkins Adhesions, Scar, Connective Tissue Adhesions – May cause SI joint mobility impairments. Treatment – Specialized visceral mobilization. Scar – May cause adhesions, spasm, or pain-inhibited PFM weakness. Treatment – Soft tissue mobilization, friction massage, electrotherapy, hot, cold, PFEs, biofeedfack. Connective tissue – Muscle strain may result in irritation and shortening of fascia and tendons. Treatment – Soft tissue mobilization, therapeutic exercise, modalities (i.e., US, ES, HPs). Copyright 2005 Lippincott Williams & Wilkins Posture Impairment Copyright 2005 Lippincott Williams & Wilkins Coordination Impairment Related to inappropriate patterns of timing and recruitment of PFMs and abdominal muscles. Inability to contract and relax PFMs at appropriate times. Lack of coordination of PFMs during ADLs is observed with stress incontinence. Activation of TrA and LM occurs with PFMs – training this synergy can be useful to restore coordination to PFMs. Copyright 2005 Lippincott Williams & Wilkins Clinical Classification of PFM Dysfunction 1. 2. 3. 4. Supportive dysfunction Hypertonia dysfunction Incoordination dysfunction Visceral dysfunction Copyright 2005 Lippincott Williams & Wilkins Supportive Dysfunction Impaired performance of PFMs Treatment (TMT) – PFE with facilitation Incoordination of PFMs TMT – PFE with SEMG feedback during ADLs Pain in PFMs TMT – Origin of pain must be treated Joint mobility impairment of lumbopelvic joints TMT – Soft tissue/joint mobilization, muscle energy techniques, therapeutic exercise Copyright 2005 Lippincott Williams & Wilkins Hypertonia Dysfunction May result from many possible physiologic impairments such as pelvic joint dysfunctions, hip muscle imbalance, abdominopelvic adhesions and scars. Interventions vary widely and are based on underlying impairments. Copyright 2005 Lippincott Williams & Wilkins Incoordination Dysfunction Neurologic syndrome For example, detrusor sphincter dyssynergia results from neurologic lesion in the spinal cord between the brainstem and T10. Non-neurologic syndrome Characterized by absent or inappropriate patterns of timing and recruitment of PFMs. Often related to disuse and decreased awareness of PFMs and abdominal muscles. Functional limitation includes stress incontinence during coughing, sneezing, lifting. Copyright 2005 Lippincott Williams & Wilkins Visceral Dysfunction Disease or abnormality in mobility or motility of the abdominopelvic visceral tissues that leads to pain and musculoskeletal impairments. Urge incontinence is the most widely seen visceral dysfunction directly related to the PFMs. Visceral mobilization techniques are used to restore normal mobility to organs. Combine with postural training, comprehensive therapeutic exercises involving PFMs, abdominal and hip musculature. Copyright 2005 Lippincott Williams & Wilkins Therapeutic Exercise Interventions for Common Impairments Incontinence Stress incontinence Urge incontinence Mixed incontinence Overflow incontinence Functional incontinence Copyright 2005 Lippincott Williams & Wilkins Stress Incontinence Involuntary leaking of urine on effort or Exertion, such as coughing, laughing, sneezing, and lifting. PFEs SEMG/pressure feedback Vaginal cones NMES Copyright 2005 Lippincott Williams & Wilkins Urge Incontinence Urge incontinence is defined as leaking urine associated with a strong urge to urinate. Bladder training Avoid bladder irritants PFEs SEMG/pressure feedback Low-frequency NMES Medications Copyright 2005 Lippincott Williams & Wilkins Mixed Incontinence Mixed incontinence is a combination of stress and urge incontinence symptoms. PFEs Bladder training Avoid bladder irritants SEMG/pressure feedback Vaginal cones NMES Medications Copyright 2005 Lippincott Williams & Wilkins Overflow Incontinence Overflow incontinence results from a failure to empty the bladder fully. Medical evaluation may be needed Advanced PFM rehab with SEMG/pressure feedback NMES MFR PFEs Bladder training Copyright 2005 Lippincott Williams & Wilkins Functional Incontinence Functional incontinence is defined as the loss of urine because of gait and locomotion impairment (inability to get to toilet quickly). Gait training Transfer training Strengthening exercises for lower & upper extremities Environmental modifications (velcro-open pants, skirts/dresses, absorbent garments) Copyright 2005 Lippincott Williams & Wilkins Additional Diagnoses 1. 2. 3. 4. 5. 6. 7. 8. Organ prolapse Chronic pelvic pain Levator ani syndrome Coccygodynia Vulvodynia Vaginismus Nonrelaxing puborectalis syndrome Dyspareunia Copyright 2005 Lippincott Williams & Wilkins Adjunctive Interventions Many other interventions are used in conjunction with exercise for the treatment of pelvic floor dysfunction. Biofeedback Basic bladder training Scar mobilization Copyright 2005 Lippincott Williams & Wilkins Biofeedback It is necessary to provide all patients with some form of biofeedback whether it is a finger in the vagina, a mirror, or surface EMG. Surface EMG and pressure biofeedback are two methods of machine biofeedback. SEMG – Provides precise information regarding quality of contraction(s), recruitment patterns, and resting/baseline tone. Copyright 2005 Lippincott Williams & Wilkins Surface Electromyography (SEMG) Copyright 2005 Lippincott Williams & Wilkins Basic Bladder Training Scheduled voiding to regain normal voiding patterns. Used in cases of urgency, frequency, urge incontinence, or mixed incontinence. Patient keeps a record of time of day he or she urinates in the toilet, time of incontinence, and cause of incontinence. Average voiding interval is determined. Voiding interval is adjusted based on improvements in continence. Copyright 2005 Lippincott Williams & Wilkins Scar Mobilization Copyright 2005 Lippincott Williams & Wilkins Summary Pelvic floor tissues include four skeletal muscle layers. Pelvic diaphragm is the largest group of PFMs and is 70% ST, 30% FT. Three functions of pelvic floor are supportive, sphincteric, sexual. All patients should be screened for PFM dysfunction using brief questionnaire. Copyright 2005 Lippincott Williams & Wilkins Summary (cont.) Patients can be given self-assessment tests and selfawareness exercises. Impairments that affect PFMs include impairment in muscle performance of PFMs, abdominal muscles, hip muscles, trunk muscles; pain; joint mobility, etc. PFMs have four clinical classifications. Incontinence types include: stress, urge, mixed, overflow, and functional. Teaching PFMs involves thorough patient education. Copyright 2005 Lippincott Williams & Wilkins