Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
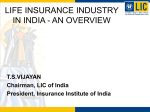
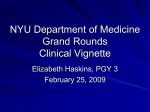
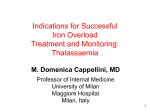
Noncompliance with Iron Chelation Therapy in an Adolescent with Thalassaemia Major Adlette C. Inati, MD Head, Division of Pediatric Hematology-Oncology Medical Director Children's Center for Cancer and Blood Diseases Rafik Hariri University Hospital Beirut, Lebanon Background Information • In thalassaemia major,chelation therapy is recommended in patients1 – With serum ferritin >1000 ng/mL, or – Who have received >10–20 blood transfusions, or – Who have an elevated liver iron concentration (level D) • Compliance with chelation therapy and adequate dose titration are crucial factors in achieving prolonged patient survival1 • The probability of survival to at least 25 years of age in poorly chelated patients was just one third that of well chelated patients2 1. Thalassaemia International Federation. Guidelines for the clinical management of thalassaemia. 2nd ed. Nicosia, Cyprus; 2008. 2. Brittenham GM, et al. N Engl J Med. 1994;331:567-573. Compliance and Survival • Survival in thalassaemia is directly related to compliance with iron chelation therapy1 • Projected survival is markedly improved with 100% compliance2 100 Survival (%) 90 Infusionsa/year 300–365 225–300 150–225 75–150 0–75 80 70 60 50 40 N = 257 30 Compliance, rather than LIC or serum ferritin, predicted survival 20 10 0 0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 aDesferrioxamine. Time (years) Abbreviation: LIC, liver iron concentration. 1. Gabutti V, et al. Acta Haematol. 1996;95:26-36. 2. Delea TE, et al. Pharmacoeconomics. 2007;25:329-342. Graphic with permission from Gabutti V, et al. Acta Haematol. 1996;95:26-36. Impact of Compliance, Ferritin and LIC on Long-Term Trends in Myocardial T2* with Deferasirox • 33 transfusion-dependent patients with thalassaemia or rare anaemias, age range 7–51 years • mT2* and T2* liver iron concentration (LIC) assessments repeated with a median interval of 14 months (3.6 occasions per patient) while receiving deferasirox • Factors associated with trends in mT2* = compliance, LIC, and ferritin • Compliance <90% (more than 3 daily doses missed per month) was associated with decrease in mT2* – Whereas compliance ≥90% was associated with an increase in mT2* (P = .0001). Garbowski M, et al. Blood. 2008;11:116. Patient Presentation • Patient is now a 16-year-old boy with thalassaemia major diagnosed at age 6 months • Treated with packed red blood cell transfusion every 3–4 weeks since diagnosis • At age 3 years, his laboratory values were as follows – LIC 12 mg Fe/g dry weight – Serum ferritin 3000 ng/mL – T2* 40 ms Decision Point 1 For the Patient at Age 3 Years, What Was the Best Next Step? a. Start patient on desferrioxamine b. Start patient on deferasirox c. Start patient on deferiprone d. Continue with transfusions but wait to start iron chelation therapy Decision Point 1 For the Patient at Age 3 Years, What Was the Best Next Step? a. Start patient on desferrioxamine CORRECT: Until recently, desferrioxamine has been the gold standard and the only approved chelator for thalassaemia. b. Start patient on deferasirox INCORRECT: 13 years ago, when this patient needed chelation, deferasirox was not available. If he were treated now, deferasirox would also be a correct choice. c. Start patient on deferiprone INCORRECT: Deferiprone is not approved for the initial treatment of iron overload in patients with thalassaemia major, but for cases when desferrioxamine therapy is inadequate or contraindicated. d. Continue with transfusions but wait to start iron chelation therapy INCORRECT: As indicated by the very high serum ferritin level and LIC, the patient has significant iron overload, which necessitates immediate chelation. Case Continues • Patient started on desferrioxamine at age 3 years • In recent years, patient was often noncompliant with desferrioxamine therapy • He complained of local pain at site of injection and was concerned about carrying a pump and not being accepted by peers • All attempts by parents and thalassaemia team to convince him to be compliant were unsuccessful • He decided to stop desferrioxamine altogether What Patients Dislike Most Patient Surveys in the United Kingdom and Cyprus 60 Cyprus (N = 119) UK (N = 129) Patients (%) 50 40 30 20 10 0 Pump Transfusions Visiting Investigations hospital With permission from Telfer P, et al. Ann N Y Acad Sci. 2005;1054:273-282. Other Impact of Infusion Iron Chelation Therapy on Patients with Iron Overload Results from Patients and Clinician Interviews Work: • Work-related travel • Ability to work late Evening social life: • Limits going out at night and doing "normal" things • Interrupts activities due to preparing Self-esteem: • Due to unsightly bumps/bruises • Due to inability to do “normal” things Impact of ICT on patients with iron overload Pain at needle site Impact on parent (thalassaemia/ SCD): • Guilt • Stress/worry • May impact relationship with child Sex life: • Pump inhibits sexual activity • May inhibit development of intimate relationships Sleep disturbance: • Specific to those with oldstyle pump: noise keeps them awake • Have to sleep on opposite side, which may interrupt sleep • Pain may also disrupt sleep Abbreviation: ICT, iron chelation therapy; SCD, sickle cell disease. With permission from Abetz L, et al. Health Qual Life Outcomes. 2006;4:73. Emotional well-being: • Depression • Anger • Frustration • Sadness Decision Point 2 What Is the Best Next Step? a. Let patient have a drug holiday, then restart desferrioxamine b. Start patient on deferiprone c. Start patient on deferasirox d. Let patient have a transfusion and drug holiday Decision Point 2 What Is the Best Next Step? a. Let patient have a drug holiday, then restart desferrioxamine INCORRECT: Patient will continue to accumulate iron, which will be toxic to his organs, from ongoing transfusions. b. Start patient on deferiprone INCORRECT: Deferiprone is indicated when desferrioxamine therapy is inadequate or contraindicated. c. Start patient on deferasirox CORRECT: Patient’s compliance is expected to increase with a once-daily oral drug, and the efficacy and safety of deferasirox in thalassaemia has been well documented. d. Let patient have a transfusion and drug holiday INCORRECT: This would deprive the patient of recommended medical treatment and increase disease complications. Case Continues • Patient was started on deferasirox 30 mg/kg/day with good tolerance • Serum ferritin levels and LIC decreased over the next 12 months on deferasirox • After 12 months, serum ferritin level started to increase • No changes in other clinical parameters, such as markers of inflammation or infection or in patient’s transfusion requirement, were observed Patient Trends in Serum Ferritin, LIC, and T2* Deferasirox 30 mg/kg/day Start of Noncompliance 3500 50 3000 Ferritin ng/mL 2500 2000 30 1500 20 1000 10 500 0 0 0 3 6 9 12 15 Months 18 21 24 T2* ms; LIC Fe g/dw 40 Ferritin ng/mL LIC Fe g/dw T2* ms Decision Point 3 What Is the Best Next Step? a. Increase dose of deferasirox b. Question the patient about compliance c. Switch to deferiprone d. Add deferiprone to the treatment regimen Decision Point 3 What Is the Best Next Step? a. Increase dose of deferasirox INCORRECT: This patient is receiving recommended dose of deferasirox and there is no indication to increase the dose. b. Question the patient about compliance CORRECT: Even with oral drugs, patients may be noncompliant. c. Switch to deferiprone INCORRECT: Deferiprone is used in cases when desferrioxamine therapy is inadequate or contraindicated. d. Add deferiprone to the treatment regimen INCORRECT: To date, there are no data on combining any other chelator with deferasirox Reasons for Noncompliance Associated with Deferasirox • • • • Forgetting to take the drug Undesirable drug-related side effects Cost of drug Ignorance among parents/patients about morbidity and mortality associated with untreated iron overload Case Continues • The patient was asked about his compliance • He admitted to forgetting to take some pills and, on occasion, had also not taken the prescribed deferasirox dose due to high drug cost and concern about possible side effects – Lack of compliance with deferasirox treatment may explain the increase in serum ferritin levels after month 12 • Counseling on the importance of compliance and taking the medication as directed was provided Outcomes • Patient continued on deferasirox 30 mg/kg/day and was fully compliant with the regimen – Serum ferritin levels and LIC steadily decreased – T2* continued normal at normal level • At month 24, serum ferritin levels had decreased to 1300 ng/mL and LIC was 3.5 mg Fe/g dw • No further adverse events or abnormal laboratory values were observed Patient Trends in Serum Ferritin, LIC, and T2* Deferasirox 30 mg/kg/day Counseling Intervention Start of Noncompliance 3500 50 3000 Ferritin ng/mL 2500 2000 30 1500 20 1000 10 500 0 0 0 3 6 9 12 15 Months 18 21 24 T2* ms; LIC Fe g/dw 40 Ferritin ng/mL LIC Fe g/dw T2* ms Conclusions • Iron chelation therapy is a safe and effective way to manage iron overload in patients with thalassaemia • Survival in thalassaemia is directly related to compliance with iron chelation therapy • Physicians need to stress to their patients the importance of full compliance with therapy if iron burden is to be reduced • Patients must take their assigned dose on a daily basis as directed and dose should be reviewed regularly at 3- to 6-month intervals – Dose adjusted according to trends in serum ferritin levels • Compliance remains a challenge for all forms of medical therapy, including oral therapies • The first thing to suspect if drug does not seem to be working is that the patient is not taking it! Thank you for participating in this webcast Please remember to take the posttest QuickTime™ and a decompressor are needed to see this picture.