Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
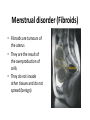
Higher level- Menstrual Cycle Hormonal control in the menstrual cycle • Four hormones involved: – FSH (Follicle Stimulating Hormone) – Oestrogen – LH (Luteinising Hormone) – Progesterone • Each hormone causes the production of the hormone following it and inhibits the hormone preceding it FSH – Follicle Stimulating Hormone • Produced by pituitary gland • Produced early in the cycle (days 1-5) • Stimulates a few potential eggs to develop, surrounded by graafian follicles • Only one usually survives • Sometimes used in fertility treatments to stimulate ovaries to produce eggs – often lots of eggs develop. This explains some multiple births • Each graafian folllicle then produces oestrogen Oestrogen • • • • Produced by the graafian follicle in the ovary Produced from days 5 -14 Causes the endometrium to develop Inhibits FSH ensuring no further eggs develop (useful in contraceptive pill) • High levels of oestrogen just before day 14 stimulate release of LH LH - Luteinising Hormone • • • • Produced by the pituitary gland Produced on day 14 Causes ovulation Causes the remains of graafian follicle to develop into corpus luteum • Corpus luteum makes final hormone in the cycle progesterone (along with small amounts of oestrogen) Progesterone • Produced by the Corpus Luteum in the ovary • Produced from days 14-28 • Maintains structure of endometrium • Inhibits FSH to stop further eggs developing • Inhibits LH to stop further ovulation and pregnancies • Prevents contractions of the uterus Insemination • Insemination is the release of sperm into the female • Contractions of uterus and fallopian tubes move the sperm to the fallopian tubes within 5 minutes • If an egg is present it releases chemicals to attract the sperm this is called chemotaxis Fertilisation Fertilisation is the fusion of the egg and sperm nuclei to form a diploid zygote. This usually occurs in the fallopian tube. Fertilisation The acrosome releases enzymes to digest the egg membrane A number of sperm may reach the egg at the same time. The sperm loses its tail and the head enters the egg. The sperm and egg nuclei fuse to form a zygote A chemical reaction at the membrane prevents other sperm cells entering. Implantation Implantation is the embedding of the fertilised egg into the lining of the uterus •This occurs 6 - 9 days after fertilisation. •By this time the zygote has grown into an embryo. •During implantation a membrane called the amnion develops around the embryo. This secretes amniotic fluid which will surround the developing embryo and act as a shock absorber. •After implantation the placenta forms. Sequence of development from fertilised egg Early stages Sequence of development from fertilised egg • The zygote contains 46 chromosomes, twenty three from the egg and 23 from the sperm It divides rapidly by mitosis to produce 2 cells, then 4, then 8, 16 etc. and continues to divide • At this point the developing individual is referred to as the morula • Around 5 days after fertilisation the morula forms a hollow ball of cells called the blastocyst • The outer layer of the blastocyst forms the trophoblast. This will later develop into the layer of membranes that surround the embryo (placenta and amnion) Trophoblast • The inner cells (called the inner cell mass) of the blastocyst will eventually form the embryo. These cells are not yet specialised. They have a phenomenal ability to differentiate – divide to give rise to many different types of tissue Inner cell mass The morula/blastocyst is pushed along the fallopian tube until it enters the uterus • Here it will implant into the uterus wall. The endometrium now provides nourishment for the developing blastocyst • Connections with the mother will begin to form (placenta and umbilical cord) This point marks the beginning of pregnancy Sequence of development from fertilised egg Development of the embryo • About 10 days after fertilisation the inner cell mass forms the embryonic disc • This usually consists of three layers called germ layers – Ectoderm (outside) – Mesoderm (middle) – Endoderm (inside) • Each of these layers gives rise to specific structures in the developing embryo • In humans the mesoderm is split by a layer called the Coelom • This allows space for more complex organs such as heart, lungs and kidneys to develop Ectoderm – skin, nervous system Coelom – heart, lungs Mesoderm – muscles, skeleton Endoderm – inner lining of digestive system The Amnion • When first formed the amnion is in contact with the embryo, but at about the fourth or fifth week fluid begins to accumulate within it (amniotic fluid) • The primary function of the amnion and amniotic fluid is the protection of the embryo for its future development Four to five weeks after fertilisation • The heart forms and starts to beat • The brain also develops • The limbs have started to form By the 6th week • Eyes are visible • The mouth, nose and ears are forming • The skeleton is at the early stages of development By the 8th week • the major body organs are formed • Sex glands have developed into testes or ovaries • Bone is beginning to replace cartilage By the 8th week • At this stage the embryo has taken on a recognisably human from. • From this point it is referred to as a foetus • The foetus continues to grow. No new organs are formed from this point By the 12th week (3 months) • The nerves and muscle become co-ordinated allowing the arms and legs to move • The foetus sucks its thumb, urinates and even releases faeces into the amniotic fluid By the 12th week (3 months) • The gender of the foetus can be seen in scans • The time from fertilisation to birth (the gestation period) lasts about 38 weeks (9 months) Placenta formation Placenta formation Placenta formation • The placenta forms from a combination of the tissues of the uterus and the embryo • Soon after implantation a membrane called the chorion completely surrounds the amnion and embryo • The chorionic villi emerge from the chorion and invade the endometrium allowing the transfer of nutrients from maternal blood to fetal blood • This combination of the chorionic villi and the endometrium will eventually form the placenta which becomes fully operational about three months into the pregnancy The Placenta Placenta Chorion Embryo Mother’s blood Wastes, Carbon Dioxide, Water Nutrients, Oxygen, antibodies Mother Embryo Amnion Amniotic fluid Umbilical cord Embryo’s blood • Placenta allows gases, nutrients, waste, antibodies, some drugs, hormones and microorganisms to be exchanged between mother and baby • Placenta also produces hormones • Blood supplies of mother and embryo do not mix – Blood types may not be compatible – Mother’s blood pressure might damage embryo • Umbilical cord connects the embryo with the placenta • it takes blood from the embryo to the placenta and back again • It must be cut at birth to separate mother and baby Birth 1 The hormones oestrogen and progesterone are produced throughout pregnancy firstly by the corpus luteum (3 months) and then by the placenta. The placenta acts as an endocrine gland. 2 Immediately before birth the placenta stops making progesterone. The walls of the uterus begin to contract as a result. 3 The pituitary gland releases the hormone called oxytocin. This causes further contractions of the uterus Labour has now begun Breastfeeding Lactation • The secretion of milk from the mammary glands • The first days after birth colostrum produced • Milk production triggered by release of prolactin by pituitary Breastfeeding Breastfeeding is better than bottle feeding because: • Colostrum and breastmilk provides the baby with essential antibodies protecting it against infection • Ideal balance of nutrients for baby • Has little fat making it is easier to digest than milk Birth control • Birth control refers to the methods employed to limit the number of children that are born • Removing the possibility of conception is called contraception. • This is achieved by preventing the egg and sperm from meeting • There are a number of methods: Mechanical contraception -male • The use of condoms • Surgical contraception – Sperm ducts are cut and tied Mechanical contraception - female • The use of diaphragms Chemical contraception • Use of ‘the pill’. The pill contains oestrogen and progesterone which prevents ovulation and hence conception. • Use of spermicide Surgical contraception • The fallopian tubes and sperm ducts can be cut and tied Natural contraception - Not having sexual intercourse during the fertile period of the menstrual cycle - Natural methods of contraception try to identify the time of ovulation based on: • monitoring the body temperature. This rises slightly after ovulation • - mucous secreted in the cervix (which changes its texture after ovulation) Infertility Infertility is the inability of a couple to achieve conception. Male infertility disorders • Low sperm count – Refers to a low number of sperm per ml of seminal fluid. • Low sperm mobility - If movement of the sperm is slow, not in a straight line or both, the sperm may have difficulty passing through the cervical mucous or penetrating the shell of the egg. • Endocrine gland failure – A failure of the testes to produce sperm Low sperm count Causes: • The persistent use of drugs such as alcohol, cigarettes and anabolic steroids. • Abnormalities in sperm production or obstruction of the tubes through which sperm travels. • Stress Treatment • A change in diet. • A change in lifestyle e.g. stopping alcohol consumption, smoking. • A reduction in stress levels. Female infertility disorders • Blockage of the Fallopian Tube – Scarring of the fallopian tube can block the passage of the egg to the uterus • Endocrine gland failure – A failure of the ovaries to produce an egg Blockage of the fallopian tubes Causes: • Fragments of the uterus lining may spread to the fallopian tube • Inflammation as a result of infection Treatment • In-vitro fertilisation (I.V.F.) In-vitro fertilisation (IVF) is a method of treating infertility It involves removing eggs from an ovary and fertilising them outside the body During IVF fertility drugs are given to the female to stimulate the ovaries to produce more than one egg During the natural menstrual cycle an egg is produced by the ovary every month These eggs are then taken from the females body and into the laboratory In the meantime a sperm sample is taken from the male The eggs and sperm are mixed together in the hope that fertilisation will occur The sample is placed in the most ideal conditions for fertilisation to occur The main aim of the procedure is to obtain a zygote. If successful the zygotes development will be monitored closely If successful the zygote develops into a morula, blastocyst and eventually becomes an embryo The developing embryo can now be placed back into the females body for implantation to take place • Babies born as a result of IVF are often incorrectly called ‘test tube’ babies. • While fertilisation takes place in the laboratory (‘in vitro’ – in glass) the fertilised egg is re-inserted into the mother’s body and develops naturally in the uterus Events when pregnancy does not occur Menstrual disorder (Fibroids) • Fibroids are tumours of the uterus • They are the result of the overproduction of cells • They do not invade other tissues and do not spread (benign) Menstrual disorder (Fibroids) • Slow growing and range from the size of a pea to the size of a melon • Common between ages of 35 and 45 • Small fibroids often produce no symptoms • As they enlarge they produce heavy and prolonged menstrual bleeding (this can lead to anaemia, pain, miscarriage or infertility) Cause • Cause is uncertain • May be an abnormal response to oestrogen • Can occur in women taking the contraceptive pill Prevention and treatment • Small fibroids require no treatment just monitoring to check their growth • Large fibroids can be removed by surgery • If many large fibroids are present a Hysterectomy may be necessary. This is where the uterus is removed Menstrual disorder (Endometriosis) • Growth of endometrial cells outside the uterus (often in fallopian tube) • Normally endometrium is shed each month in the menstrual cycle. In endometriosis misplaced endometrium is unable to exit the body • Results in internal bleeding, inflammation of surrounding area and pain • Formation of scar tissue may result • If in the fallopian tube this can interfere with the passage of eggs to the uterus (infertility) Cause • Exact cause remains unknown • Several theories (response to excess oestrogen creation) Prevention and treatment • No known cure • Hysterectomy (removal of uterus) - no guarantee that symptoms will disappear • Medication can be taken to interfere with hormones resulting in a reduction or elimination of menstrual flow