Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
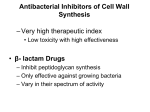
Treatment of Infections 1. Outline the defence mechanisms in the lung which are impaired by CF As CF is a deficit of the epithelial chloride channels due to abnormal functioning of the cystic fibrosis transmembrane conductance regulator (CFTR), the epithelial cells of the lungs will be affected. The defence mechanisms in the lung which are impaired are: Innate Defences o Surface barrier Mucous membrane impaired due to mutation of CFTR gene Cl⁻ secretion into the lumen Epithelial sodium channel (ENaC) action is also ↑ ↑ Na⁺ into cell ↑water into the cell Mucous membrane is dehydrated Less effective barrier Less effective barrier means o Defective mucociliary clearance o Accumulation of hyperconcentrated viscid secretions leading to obstruction and an inability to clear bacteria (especially pseudomonas aeruginosa species) o Static mucous creates hypoxic microenvironment which favours alginate production that allows bacteria to form a protective biofilm that protects them, allowing them to evade host defences. This leads to chronic lung disease and pulmonary destruction o Bronchioles distended with mucous which leads to hyperplasia (increase in number of cells) and hypertrophy (increase in size of cells) of mucous secreting cells. o Prone to bronchitis and bronchiestasis (irreversible dilatation and destruction of the bronchial walls, often as a result of infection or obstruction). o Lung abscesses can occur 2. List the major groups of antibiotics a nd outline their mechanisms of action Antibiotics can be classified according to Chemical structure Spectrum of activity Mechanism of action Bacteriocidal effect – kills all bacteria Bacteriostatic effect – stops growth (bacteria survive but don’t multiply) Narrow spectrum – affects some bacteria only Broad spectrum – affects numerous types of bacteria Group Inhibitors of cell wall Protein synthesis inhibitors Action Bacteriocidal Inhibits cell wall production that protects bacteria Inhibits production of murein (peptidoglycan) lattice of cell wall Can be bacteriocidal or bacteriostatic Selectively inhibits bacterial protein Class β-lactam Chloramphernical (broad spectrum, bacteriostatic, inhibits enzyme that links AA together, side effect is aplastic anaemia 1:50 Examples Penicillin (βlactamase resistant – methicillin, broad spectrum – ampicillin and amoxicillin, extended spectrum – antipseudomonal. These are more expensive) Cephalosporin (structurally similar to pencillin) synthesis 000, not to be given to babies because they cannot metabolise the drug) Tetracyclines (broad spectrum, bacteriostatic, bulky structure of drug blocks aminoacyltRNA binding therefore peptide bond synthesis is inhibited) Aminoglycosides (bacteriocidal, but not absorbed orally, has a narrow therapeutic window and requires monitoring. Penetration through the cell wall and requires oxygen dependent active transport, used for serious gram –ve infections) Folate synthesis inhibitors Microorganisms synthesise folate from paminobenzoic acid (PABA) so these antibiotics interfere with this synthesis process Macrolides (bacteriostatic or – cidal, wide spectrum, gram +ve, suppresses ribosome advancement, widely used as alternative to penicillin allergic patients) Trimethoprim (bacteriostatic, resembles folic acid, selective inhibitor of dihydrofolate reductase) Tetracycline, doxycycline Gentamicin, streptomycin, amikacin Erythromycin, clarithromycin, roxirithromycin Sulphonamides Sulfamethoxazole (bacteriostatic, wide range of gram +ve and –ve) Usually Nucleic acid synthesis inhibitors Narrow spectrum sulfamethoxazole used in combination with trimethoprim (co-trimoxazole) for complicated infections Quinolones (gram – ve, urinary and GIT infections only) Antimycobacterial agents (bacteriostatic, used for leprosy and TB, resistance developed rapidly) Nalidixic acid, norfloxacin Rifampicin 3. Describe the common mechanisms of resistance to antibiotics 1. Metabolic characteristics that confer a natural insensitivity to the drug on a particular strain of the bacteria (natural resistance) Lullman et al (2005) http://www.thieme.com.ipacez.nd.edu.au/SID2483990066258/ebooklibrary/flexibook/pubi d1005568195/show_pdf.html?/pdf/pubid1005568195_1000.pdf 2. Acquired resistance – random genetic mutation gives rise to resistance (susceptible bacteria die off, the resistant ones free to multiply) 3. Non susceptible DNA (resistant plasmid) is passed on from one resistant bacteria to another via conjugation (temporary fusion so genetic material can be transferred) or transduction (DNA transferred from one cell to another via a viral vector - bacteriophages – virus that causes lysis of host bacteria). This is also acquired resistance. E.g. some bacteria produce β-lactamase which breaks down the bonds in β-lactam (present in βlactam antibiotics). Therefore this renders the antibiotic ineffective against the bacteria which are resistant to it. The more frequently a drug is given the more probable resistance will develop.