Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
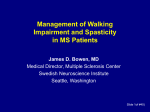
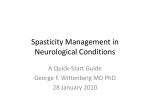
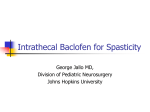
Spasticity After Stroke Heather Walker, M.D. Assistant Professor Department of Physical Medicine & Rehabilitation UNC-Chapel Hill What is a physiatrist??? NOT a physical therapist NOT a psychiatrist Education: Four years medical school Four years residency +/- Fellowship Training Take care of patients with disabilities Stroke, traumatic brain injury, spinal cord injury, amputations, burns, pediatrics, etc. Goal is to improve function and quality of life Physiatrists and Stroke Medical management during acute inpatient rehabilitation and as an outpatient Blood pressure Bowel and bladder dysfunction Skin Language impairments Cognitive and attentional impairments SPASTICITY What is spasticity?? “a motor disorder characterized by a velocity-dependent increase in tonic stretch reflexes (muscle tone) with exaggerated tendon jerks, resulting from hyperexcitability of the stretch reflex…” ???????????????????????? Spasticity can be defined as increased tightness in affected muscles What is spasticity?? Increased tightness in muscles Chest wall Difficulty raising arm to the side, putting on clothing Elbow flexors Difficulty straightening arm to reach for items or dressing Wrist flexors Finger flexors Difficulty opening hand voluntarily or passively (releasing items, hand hygiene) What is spasticity?? Increased tightness in muscles Hamstrings Difficulty straightening leg Quadriceps Stiff-knee gait Calf muscles Difficulty clearing toes when walking (tripping), foot turns in when walking Inner thighs Legs cross over each other when walking, difficulty pulling legs apart for hygiene Upper Extremity Spasticity Lower Extremity Spasticity Spasticity Complications Positioning Hygiene ADLs Sitting or Standing Balance Contractures Treatment Goals Improvements in position Mobility Pain Contracture prevention Ease of care are possible Spasticity Management Steps Therapeutic modalities Oral Medications Nerve blocks & Chemical neurolysis (Botox injections) Orthopedic procedures Intrathecal Medications Prior to Intervention Assess baseline status Determine specific goals Patient and family education PT and OT role after intervention Therapeutic Exercise Stretching and range of motion Myofascial and joint mobilization Active assistive, active and resistive exercise Endurance training Oral Medications Zanaflex Baclofen Adverse effects: drowsiness, dizziness, dry mouth, orthostatic hypotension Adverse effects: weakness, sedation, hypotonia, ataxia, confusion, fatigue, nausea, dizziness, lower seizure threshold Sudden withdrawal may cause seizures, hallucinations, rebound spasticity Dantrium Adverse effects: weakness (including ventilatory muscles), drowsiness, lethargy, nausea, diarrhea, Liver toxicity Botulinum Toxin Type A (BOTOX®): History of Development FDA approval of BOTOX® Dr. Schantz begins investigation C. botulinum identified 1989 1978 1944 1920s 1895 Botulinum toxin type A first isolated Dr. Scott initiates first therapeutic testing in humans BOTOX® (Botulinum Toxin Type A): A Focal Therapeutic • • • − Injected directly into overactive muscles Reduces contractions, relaxes muscles Advantages of local injection − Targeted to specific muscles that are causing the symptoms − When used at recommended doses, avoids systemic, overt distant clinical effects NOT FDA APPROVED FOR SPASTICITY Muscle identification Three main methods Exam and anatomic atlas EMG assistance and guidance Electronic stimulation Side Effects Localized Hematoma and bruising are seen regardless of the site injected Local weakness, created by diffusion of Botox and is site specific Death??? Intrathecal Baclofen Small doses of baclofen delivered directly to the spinal canal Fewer side effects, better relief of spasticity Usually more effective for spasticity in the lower extremities Requires committed patient and family, pump must be refilled every 3 months. Intrathecal Baclofen Surgical Procedures Tendon lengthening Neurosurgical procedures Last resort! Take Home Points…. Spasticity is common after stroke, and is manifested as muscle tightness in the affected arm and/or leg. Several different treatment options are available, including therapies, oral medications and injections. If you suffer from spasticity you should be seen by a physiatrist who specializes in spasticity management.