Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
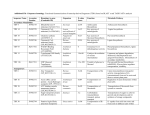
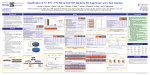
Precision of Transdermal Fentanyl Prescribing at UMHS Kate Veltman Advised by Dr. John Clark September 6, 2013 IRB HUM00062367 Objectives • Explore the unique PK/PD profile of transdermal fentanyl (TDF), the differences between oral opioids and transdermal fentanyl, and how these differences affect usage • Review the FDA black box warning, dosing chart, and absolute contraindications and determine if these are supported by outside literature • Look at the results of a retrospective study examining transdermal fentanyl prescribing at UMHS and discuss the implications for patient care What is TDF? • Long-acting transdermal opioid designed to be used for chronic pain control • Only CII opioid currently on the market in transdermal form • Other transdermal pain medications available: • Buprenorphine (Schedule III) • Lidocaine (legend, non-controlled) http://medlibrary.org/lib/images-rx/fentanyl-transdermal-system-1/a7c456e6-403b-4aae-a57660b106bf66a7-01.jpg TDF versus Oxycontin® TDF ER Oxycodone Dosing schedule Every 72 hours Every 12 hours Tmax 20 to 72 hours 2.1 to 3.2 hours Half-life 20 to 27 hours 4.5 to 8 hours 6 L/kg 2.6 L/kg Hepatic impairment AUC ↑ 120% AUC ↑ 95% Renal impairment AUC ↑ 100% AUC ↑ 60% Volume of distribution Micromedex. Accessed July 24 2013. Dosing Current Analgesic Daily Dosage (mg/day) 25 mcg/hr 50 mcg/hr 75 mcg/hr 100 mcg/hr Oral Morphine 60-134 135-224 225-314 315-404 IV/IM Morphine 10-22 23-37 38-52 53-67 Oral Oxycodone 30-67 67.5-112 112.5-157 157.5-202 Oral Hydromorphone 8-17 17.1-28 28.1-39 39.1-51 150-447 448-747 748-1047 1048-1347 20-44 45-74 75-104 105-134 Oral Codeine Oral Methadone Duragesic full prescribing information. Revised 7/2012. Titration and tapering • Titration • May increase dose no more than every 3 days • Increase based on amount of breakthrough meds needed on days 2 and 3 • 45 mg morphine = 12.5 mcg/hr increase • Dose interval may be changed to every 48 hours if wearing off occurs, but dose increase should be considered first • Taper • Decrease by no more than half the current dose no more frequently than every 6 days • Withdrawal symptoms may occur Unique PK profile: Pros and Cons BENEFITS • Long-term, constant pain relief • Compliance • No swallowing DANGERS • Overdose potential • Mcg/hr strength • Patient understanding • Requires careful disposal • Heat sensitive Duragesic® and the FDA • FDA mandated specific dosing guidelines and contraindications designed to prevent fatal respiratory depression • • • • • • Patients who are not opioid tolerant Acute pain or intermittent pain Post-operative pain (in- or out-patient) Mild pain Respiratory compromise Severe or acute bronchial asthma • REMS program participant Duragesic full prescribing information. Revised 7/2012. Chronic Pain Management • WHO guidelines: opioids are mainstay of therapy • Oral drugs preferred • Morphine: “gold standard” drug http://idsportsmed.com/patient_education/45/eeb17d844459b3adc6ce05a5f1559f42 Ripamonti et al. Support Care Cancer. 2006;14:400-407. Efficacy in pain management • Equally effective in RCTs comparing to morphine for both chronic non-cancer and cancer pain1,2 • Surgical pain: higher doses decrease PCA use compared to placebo3 • Satisfaction, pain control: varies by study3,4 • Shows some benefit over ER morphine in regards to pain during movement at 24 hours post-op, but not at 12 or 36 hours4 • Open-label crossover: fentanyl had higher satisfaction and better pain control5 1. Allan et al. SPINE. 2005;30(22):2484-2490. 2. Ahmedzai & Brooks. J Pain Symptom Management. 1997;13(5):254-261. 3. Caplan et al. JAMA. 1989;261(7):1036-1039. 4. Sevarino et al. Anesthesiology. 1992;77:463-466. 5. Allan et al. BMJ. 2001;322:1-7. Convenience factors • Dosed every 72 hours (or every 48 hours) • Easier administration and compliance > 90%1 • No swallowing required • Nursing studies show increased nurse satisfaction when using fentanyl as opposed to morphine PCA for post-surgical patients2 1. Chiou et al. AJH. 2010;27:31. 2. Lindley et al. JAN. 2009;65:1370. Safety of TDF • Serious adverse effects of all strong opioids: • Constipation • Nausea/vomiting • Somnolence • Respiratory depression and death 1. Allan et al. BMJ. 2001;322:1-7. 2. Weschules et al. PainMed. 2006;7:320-329. 3. Allan et al. SPINE. 2005;30:2484-2490. Adverse Effects • Compared to oral morphine, studies generally show fentanyl is associated with: • Increased nausea1 • Decreased constipation1,3 • Decreased sleep amount2 • Decreased ability to communicate2 • Increased risk of respiratory depression or death4 • Participant withdrawal rates tend to be similar in both groups in studies2,3 1. Allan et al. BMJ. 2001;322:1-7. 2. Weschules et al. PainMed. 2006;7:320-329. 3. Allan et al. SPINE. 2005;30:2484-2490. 4. Sevarino et al. Anesthesiology. 1992;77:463-466. Safety of TDF: Respiratory Depression • Serious, potentially fatal adverse event • Bradypnoea: less than 10 breaths per minute1 • High risk in opioid naïve patients • Can still occur in opioid tolerant patients • Mechanism:2 • Opioid sensitive chemoreceptors responsible for breathing rhythm decrease tonic input, causing decreased breathing rate • Decreases in tidal volume are observed • This is partly compensated for by increased PaCO2 1. Bulow et al. Acta Anaesthesiol Scand. 1995;39:835-839. 2. Pattinson. Br J Anaesth. 2008;100(6):747-758. Safety of TDF: Respiratory Depression • Many studies on use in contraindicated populations focus on pain score and common adverse effects; do not monitor respiratory rate • Japanese study: initiation of TDF in doses above the recommended minimum (25 mcg/hr) showed significant respiratory effects1 • This was true whether prescribed by general physicians or palliative care specialists1 1. Hashizume et al. Kagaku Ryoho. 2007;34:897-902. Safety of TDF: Respiratory Depression • Denmark study: Small RCT evaluating TDF vs morphine PCA after major upper abdominal surgery • TDF was applied 1 hour before surgery began and was left in place for 72 hours • 3 of 10 patients randomized to 100 mcg/hr TDF experienced bradypnoea • One required naloxone due to significantly decreased PaO2 • All started between 11 and 12 hours after last intraoperative fentanyl dose Bulow et al. Acta Anaesthesiol Scand. 1995:39;835-839. Safety of TDF: Respiratory Depression • USA: RCT of 42 patients undergoing major shoulder surgery, receiving either 75 mcg/hr patch immediately prior to surgery or morphine PCA post surgery • Significant decrease in respiratory rate with TDF between hours 13 and 24 post-op (p = 0.002) • Placebo: 16 ± 2 breaths per minute • TDF: 14 ± 3 breaths per minute • 3 patients experienced transient bradypnoea of 5 to 7 breaths per minute while sleeping; patients were awoken and breathing rate increased Caplan et al. JAMA. 1989;261:1036-1039. What’s the actual risk? • IMSN study of 3291 voluntarily reported incorrectly prescribed TDF prescriptions in Canada, USA, UK and Ireland found: • 32.8% were wrong dose, strength, or quantity of patches • 30.5% were dose omission or underdosing • The major themes of these Rxs were: • Overdosing, or administered too soon • Underdosing, or administered too late • Patient did not need/should not have received medication • Other • There were significant risks to these patients • 8% resulted in harm but not death • 0.3% resulted in death ISMP. 2009. Medication incidents related to the use of fentanyl transdermal systems: An international aggregate analysis. Study Rationale • Current prescriptions written at UMHS are not evaluated by a pharmacist for appropriate use before dispensing • Unique pharmacokinetic factors of transdermal fentanyl make incorrect dosing potentially dangerous to the patient • It is currently unknown whether patients at UMHS are receiving prescriptions written in accordance with FDAlisted guidelines and contraindications • Objective: to determine whether prescribers at UMHS are appropriately using TDF, and if not, what deviations from are most common Methods • Retrospective descriptive chart review • 200 patients reviewed, 106 qualified • Inclusion criteria • 18 or older • First TDF prescription written at UMHS • Filled at least one TDF Rx at UMHS in 2010 or 2011 • Exclusion criteria • First Rx written by outside hospital or physician • Lack of proper documentation to determine previous analgesia Methods • Data collected: • General patient information, including age and BMI • Previous analgesia (drug and dosing) • Length of time on previous analgesia • Prescriber service • Presence of contraindications • Surgical pain • Non-surgical acute pain • Intermittent pain or PRN dosing • Accurate dosing was determined as maximum daily dose ± 25% Methods • Statistical analysis • Descriptive statistics calculated using SPSS • Categorical data: chi squared analysis • Discrete data: regression analysis • Data was considered significant if p < 0.05 • Analysis included: • Actual dose as a function of age or BMI • Accurate dosing as related to various demographic characteristics Results Characteristic Quantity (n = 106) Percentage Female 50 47% Age* 55 ± 12 years N/A Overweight 50/91 56% Caucasian 89 83% Started inpatient 20 19% * p = 0.022; R = -0.222 Results Prescriber Service Prescriber Type 3% 2% 3% 10% Hem/Onc Gen Med NP, 41% MD, 42% Surgery 82% SympAll Other PAC, 17% Results Analgesia Prior to TDF 35% 30% 32% 27% 25% 20% 15% 10% 10% 12% 12% 5% 0% 2% 4% Results Incidences of Prescribing Discrepancies 60% 54% 50% 40% 39% 30% 20% 10% 16% 0% No breakthrough med Incorrect dose Contraindicated Incidence of Dosing Discrepancies 35% 30% 29% 25% 25% 20% 15% 18% 10% 5% 0% Not appropriate Overdose Underdose Use In Contraindicated Populations 25% 20% 21% 15% 10% 5% 8% 8% 3% 0% PRN usage Acute pain Surgical pain < 1 week on opioids Results • 19 patients did not qualify for any strength of TDF based on previous opioid usage and were evaluated based on: • Swallowing ability • Prescribing of breakthrough pain medications • Initial dosage Ability to Swallow Considerable difficulty swallowing, 3 Difficulty swallowing, 3 Able to swallow, 13 Breakthrough Medication Prescribing No breakthrough meds, 7 Breakthrough meds, 12 Starting Dose 50 mcg/hr, 2 25 mcg/hr, 2 12 mcg/hr, 15 Conclusions • The majority of patients (54%) are receiving an incorrect dose of TDF upon initiation of therapy • Prescribers are using TDF as a first-line therapy, both for initial pain control and for long-acting opioids • Patients not opioid tolerant at any level are receiving TDF relatively frequently (18% of patients) and do not have clearly indicated prescriber rationale • Most patients are being treated for conditions that typically require long-acting pain medication, with a predominance (82%) in hematology/oncology • All types of prescribers are prescribing similarly, and there are no significant trends suggesting consistent prescribing Future Direction • Determine barriers to correct prescribing • Develop a strategic medication safety plan to improve patient safety by facilitating proper prescribing • Discourage improper prescribing via prescriber education and other available tools such as CPOE prompts Discussion Questions • Are there any contraindications that appear to be either unclear or unreasonable? • Which errors seen at UMHS seem most likely to cause patient harm? • What challenges could prescribers be facing that prevent them from proper prescribing? • What role can pharmacists play in prevention of patient harm with use of TDF?