Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
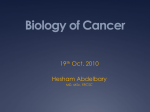
RESPONSE TO LENVATINIB IN PROGRESSIVE METASTATIC PARAGANGLIOMA Sina Jasim,M.D.1, Chintakuntlawar, Ashish,M.D.PhD 2, Keith Bible, M.D.PhD 2 1Division of Endocrinology, 2Division of Medical Oncology Mayo Clinic, Rochester, MN BACKGROUND: • Paragangliomas are rare, sometimes malignant, vascular endocrine tumors that highly express vascular endothelium growth factor (VEGF). • Anti-angiogenic agents may thus play a role in the treatment of these tumors. • We report a dramatic clinical response to the oral VEGFR 1-3 and multi-kinase inhibitor lenvatinib. CASE DESCRIPTION • A 49-year-old female with longstanding metastatic pelvic PGL with SDHB (p.V140F--c.418G>T) mutation. • Multiple surgical resections, chemotherapeutic regimens (etoposide, cisplatin; cyclophosphamide, doxorubicin, cisplatin; cyclophosphamide, vincristine, dacarbazine) as well as with local therapies at metastatic sites (radiation, cryoablation). • She benefited from pazopanib (VEGFR and multi-kinase inhibitor) for ~2 years, attaining a partial response, but ultimately progressed with the development of hypertension. • CT scans of chest, abdomen and pelvis showed progression of hilar, pelvic and peritoneal metastatic lymphadenopathy. • Laboratory values: Metanephrine level < 0.20 nmol/L (<0.50 nmol/L),nor-metanephrines 5.7 nmol/L (<0.90 nmol/L), Chromogranin A 1018 ng/mL (< 93 ng/mL) • Radiotherapy to the right hilar lymphadenopathy (4000 cGy, 10 fractions; irradiated disease progress despite radiotherapy) • Alpha and beta blockade (phenoxybenzamine and atenolol) as well as calcium channel blockers started to maintain controlled blood pressure while initiating lenvatinib (24 mg daily). RESULTS • Within 48 hours of lenvatinib initiation, she had dramatic nodal clinical tumor regression associated with fever. Work up revealed no infectious source for fever. • Laboratory evaluation were consistent with mild tumor lysis syndrome. • Biochemical response (Figure 1) • Follow up imaging showed interval decreases in hilar and retroperitoneal adenopathy and a confirmed RECIST response (Figure 2) • Side effects prominently included fatigue. RESULTS Figure 1A: Chromogranin A level Figure 1B: Normetanephrine level Chromogranin A (ng/mL) 1200 Normetanephrine (nmol/L) 1018 6 1000 5.7 5 800 4 600 400 200 3 3 306 93 93 280 2 93 1 1.7 0.9 0.9 0.9 1.1 Jul-15 Aug-15 Sep-15 Oct-15 0 0 Jul-15 Aug-15 Patient Sep-15 Reference Oct-15 Patient Reference FIGURE 2: CT CHEST BEFORE AND ON THERAPY DISCUSSION/CONCLUSION • Like other VEGFR-targeted kinase inhibitors, lenvatinib may represent a promising drug for further development in treating refractory metastatic paraganglionoma. • Systemic therapies, like multi-kinase inhibitors , can induce hypertensive episodes, which require close monitoring, as well as have potential to induce tumor lysis-like phenomena. • Special care must be taken to respond emergently to minimize patient risks in the event of rapid tumor regression.