Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
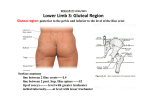
This is an enhanced PDF from The Journal of Bone and Joint Surgery The PDF of the article you requested follows this cover page. Structures at risk from medially placed acetabular screws EM Keating, MA Ritter and PM Faris J Bone Joint Surg Am. 1990;72:509-511. This information is current as of October 26, 2009 Reprints and Permissions Click here to order reprints or request permission to use material from this article, or locate the article citation on jbjs.org and click on the [Reprints and Permissions] link. Publisher Information The Journal of Bone and Joint Surgery 20 Pickering Street, Needham, MA 02492-3157 www.jbjs.org Copyright 1990 by The Journal of Bone Structures Medially BY E. MICHAEL at Placed KEATING, M.D.t, and Joint Risk From The ABSTRACT: fourteen acetabula the Department MERRILL the Centerfor of Orthopaedic anatomical were studied structures to identify Incorporated from Acetabular A. RITTER, MOORESVILLE, and Surgery, Hip adjacent to structures M.D.t, AND PHILIP M. FARIS, M.D.t, INDIANA and Surgery, Screws* Knee Surgery, Louisiana State screws; vascular Mooresville, University, Shreveport, many manufacturers complications that Louisiana now sell such components. have been reported usually The have that are at risk from acetabular screws. There were six embalmed acetabula, four acetabula from two fresh autopsy specimens, and four acetabula that were studied been related to intrapelvic extrusion of cement or to damage to the common iliac vein during reaming’3. Little attention during when two gynecological operations. Models screws can penetrated structed to show where these dially placed screws either were penetrate. or came conMedan- has been paid, however, to the risk to anatomical structures a drill-bit or screw penetrates the second cortex. Although orthopaedic surgeons are very familiar with the structures that are anterior, superior, and posterior to ACETABULAR COMPONENT IN RIGHT _/ ACETABULUM SYMPHYSIS 1 FIG. Fig. Fig. possible 1: Drawing 2: Drawing placement of the right pelvic of the right pelvic of the screws. brim. brim, FIG. 2 showing placement of the gerously close to the external iliac vein; the obturator artery, nerve, and vein; and tributaries of the internal iliac vein. To avoid injury to the medial vascular structures, screws should not be placed in the anterosuperior quadrant of the acetabulum. acetabular cup, interest has developed in the use of porouscomponents that are fixed with cancellous holes the acetabulum, that lie medial tation in 1986. drilled in the pelvis and pins used many are not as well acquainted to it. Our interest was piqued After a revision hip arthroplasty, penetration of a branch by selective prompted us to study acetabulum of an internal arteriography. the structures to determine iliac The the danger to demonstrate with those by a consulthis patient had a retroperitoneal hematoma, anuria, and infection about the implant; the patient eventually mined Substantial coated acetabular with a secondary died from artery, case as deter- of this patient that lie adjacent of penetration to the by a drill- bit or screw. * No benefits in any form have been received or will be received a commercial party related directly or indirectly to the subject No funds were received in support of this study. t Center for Hip and Knee Surgery, 1 199 Hadley Road, Indiana 46158. VOL. 72-A, NO. 4, APRIL 1990 ofthis from Materials article. Mooresville, Three embalmed types acetabula and of anatomical and four Methods subjects fresh autopsy were studied; specimens six were 509 510 E. M. KEATING, M. PJT. ILIAC EXT. ILIAC A. A. & V. V. RITTER, AND P. M. FARIS joined the external thus did not course iliac vein as it entered the pelvis and along the surface ofthe internal obturator muscle with the obturator nerve. The sciatic nerve, as it left the pelvis, lay directly against the osseous surface of the sciatic notch adjacent to the internal iliac vein. In the acetabula that were studied during the gynecological opera- OBTURATOR tions, surface the external iliac of the arcuate vein line, lay and directly thus it was on the osseous not protected by the iliopsoas and iliacus muscles as it appeared to be in the cadavera. The external iliac artery, however, coursed along the iliopsoas muscle and tendon and thus was relatively protected by the thickness of the muscle. In the models and the cadaver specimens, screws that were inserted into the anterior part of the rim and the depths of the acetabular cup either penetrated or came dangerously close to the external iliac vein; the obturator artery, nerve, FIG. 3 Drawing of the right pelvic brim, showing penetration of the external iliac vein, obturator vein, and tributaries of the internal iliac vein by holes drilled in the anterosuperior portion of the acetabulum. The arrows indicate the areas of penetration marked by fixation pins that were used to secure the acetabular component. dissected, of two and four additional hysterectomies. and porous-coated overly sional acetabula Six cadaver were as part studied acetabula were reamed, acetabular components were secured We constructed four long screws. models. then with AREA three-dimen- Results In our dissections, the internal obturator muscle was only two to four millimeters thick and provided minimum protection for the adjacent vascular structures. The obturator artery, vein, of the pelvis inferior to the obturator that included internal iliac and nerve on the the pudendal vein2 (Fig. coursed way medially to the foramen the arcus below superior and vein, and other branches tributaries of the internal 1). The tendineus was the rim foramen. was a large plexus inferior were found two to three millimeters wall of the pelvis, with no strong since just obturator vesicular of veins veins, (the arcus iliac vein medial barrier, tendineus is the lateral origin of the levator ani muscle, which forms the abdominal floor). The intra-abdominal tributaries of the internal iliac vein, especially the superior and inferior vesicular veins and the uterine plexus, were extremely variable; they really were a plexus of veins usually formed a and on the inferior obturator muscle. In two of the were replaced by rather than a single vein. These the obturator pubic vein 4 acetabulum. The shaded of intrapelvic structures area represents by a screw the danger or drill-bit. and vein; and tributaries of the internal iliac vein (Figs. 2 and 3). Any screws that were placed in the superior portion of the acetabulum and penetrated the medial wall were close to the external iliac vein and the internal iliac venous plexus. The bladder and rectum were relatively safe. Neither the screws that were placed vein and artery and artery that posterior tabulum nor those placed distal transverse acetabular ligament dangerous position (Fig. 4). to the midline of the ace- to the anterior border of the penetrated the pelvis in a Discussion vessels plexus that lay on the levator ani muscle portion ofthe exposed part of the internal specimens, an enlarged FIG. Drawing of the right zone for the penetration the of the internal from the osseous protecting fascial inferior Just The sciatic nerve lies against the posterior wall of the acetabulum as it leaves the pelvis at the greater sciatic notch. This nerve may be identified and protected by palpation of the posterior part of the wall of the acetabulum during drilling and the insertion of screws; thus, screws that are placed ThE JOURNAL OF BONE AND JOINT SURGERY STRUCTURES in the posterior inferior the portion anterior part of the wall of the acetabulum, attachment ment, is relatively longer artery, near the medial and vein are pelvis, by the The tributaries viously; of safe, the since iliopsoas and that posterior transverse iliacus artery it has safe. and to is no The femoral nerve, as they leave the is replaced inferior epigastric noted, replaced by an enlarged stated that the obturator by an enlarged small pubic in 30 per number anatomical that we have described cent from the population4. ofdissections variations are present branch of the in our study, other than in the area the ones medial to the acetabulum. Screws been reported preand venous system that 511 SCREWS artery In view ofthe it is possible tendons. as already ACETABULAR artery liga- cavity and PLACED The distal in the intra-abdominal vein has arterial were been MEDIALLY acetabular muscles In two of our dissections, the obturator vein and pubic vein and artery; FROM the abdominal we found of the internal iliac this is the most variable RISK are relatively wall of the pelvis. protected laterally, variability in the body4. AT that are inserted in the anterosuperior of the acetabulum, a pie-shaped arc drawn from the mid-portion quadrant area that is bounded of the superior dome anterior border of the transverse acetabular ligament, the most dangerous area because of the thinness acetabulum dially. and the intra-abdominal vascular by an to the are in of the structures me- References I . BERGQVIST, 163, 2. 3. 4. VOL. A. S.; and ERICSSON, B. F.: Vascular Complications after Total Hip Arthroplasty. Acta Edited by Roger Warwick and P. L. Williams. British ed. 35, pp. 668-708. Philadelphia, W. T. H. : Rupture of the Common Iliac Vein from Reaming the Acetabulum during Total Hip Replacement. , 54-A: 276-277, March 1972. R. T.: Essentials of Human Anatomy. Ed. 6, pp. 500-505, 511, 536. New York, Oxford University ANATOMY: MALLORY, Surg. WOODBURNE, 72-A, CARLSSON, Orthop. Scandinavica, 54: 157- J. Bone and 1983. GRAY’S Joint D.; NO. 4, APRIL 1990 B. Saunders, A Case Press, 1973. Report. 1978.