Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
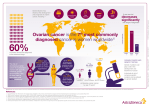
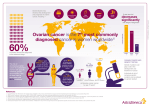
Running head: IMPLICATIONS OF GENETIC TESTING Implications of Genetic Testing Kaeleigh A. Molloy University of New Hampshire 1 IMPLICATIONS OF GENETIC TESTING 2 To gain a better understanding of the ethical, legal, and social implications of genetic testing, one should examine a real-life scenario. With that being said, in this paper one of Mariann Harding, Julie Snyder, and Barbara Preusser’s (2016) cases, which reads as follows, will be investigated: R.M. is a 58-year-old woman with stage III ovarian carcinoma. Her initial treatment is an exploratory laparotomy with a total abdominal hysterectomy, an ileocecal resection and anastomosis, omentectomy, and peritoneal biopsies. The postoperative CA-125 level is 69 units/mL. Family history analysis reveals a strong positive occurrence of breast and ovarian cancer in R.M.’s family. Her mother died of breast cancer at the age of 56, and a maternal aunt died of ovarian cancer at the age of 59. The oncologist suggests testing for the presence of the BRCA1 and BRCA2 genes and, if the results are positive, testing of R.M.’s two daughters and son. (p. 447). Then, using supporting evidence, effective solutions will be proposed. Before delving into said implications, however, it is important to take a deeper look into the testing itself, which revolves around mutations in the BReast CAncer (BRCA) 1 and 2 genes (National Cancer Institute, 2015). Normally, BRCA1 and BRCA2 function as tumor-suppressing genes, producing proteins that regulate cell growth and repair damaged deoxyribonucleic acid (DNA) (Greenberg, 2006, p. 1103). When mutations in these breast cancer-linked genes occur, though, their protein products do not function correctly. As a result, cells are likely to divide and grow in an uncontrolled way. Hence, persons with these mutations are at an increased risk of developing breast cancer. Additionally, depending on their sex, they are at a higher-than-average risk of developing either ovarian or prostate cancer (Susan G. Komen, 2016). It is important to note, however, that testing positive for the presence of BRCA1 and BRCA2 mutations does not IMPLICATIONS OF GENETIC TESTING 3 guarantee a diagnosis of cancer. Instead, it gives at-risk individuals an opportunity to better manage their health, which some would say is a benefit of genetic testing (“Seeking Your Genetic Information: Pros and Cons,” 2014). For instance, in their research article, Heidi Nelson, Miranda Pappas, Bernadette Zakher, Jennifer Priest Mitchell, Leila Okinaka-Hu, and Rongwei Fu (2013) argue that those who test positive can lower their risk of breast and/or other cancers by undergoing prophylactic surgery, taking risk-lowering drugs, and/or having more frequent exams. For example, women with BRCA1 and BRCA2 mutations may choose to have mastectomies and/or oophorectomies. That is, to prevent their risk of developing breast and/or ovarian cancer, they may choose to have their breasts, ovaries, or both surgically removed. Or they may choose to take a less drastic measure. They may, for example, begin taking a hormonal therapy medicine, such as tamoxifen, raloxifene, or exemestane, as these drugs have been found to reduce the risk of developing breast cancer. Or, to reduce their risk of developing ovarian cancer, they may choose to take oral contraceptives. Or they may choose to take the least drastic measure of all, which would be to take advantage of more frequent pelvic exams and breast screenings. Rather than once a year, they may choose to visit their gynecologist and primary care physician every six months. Similarly, male carriers may choose to have annual digital rectal examinations and, if they are between the ages of 40 and 50, prostate-specific antigen (PSA) blood tests. But, despite all of these things, some people may choose not to be tested, for they fear that a positive test result would trigger anxiety, depression, or anger. Also, parents who pass these mutations onto their children may feel guilty or worried, even though a positive test result does not necessarily mean their children will develop cancer (“Seeking Your Genetic Information: Pros and Cons,” 2014). Say, for example, that after finding out their mother tested positive for a BRCA2 mutation, IMPLICATIONS OF GENETIC TESTING 4 R.M.’s two daughters and son choose to be tested. Though their mother has a mutation in her BRCA2 gene, R.M.’s two daughters and son might not have the same, for they have a 50/50 chance of inheriting either their mother’s faulty gene or their father’s working copy (Royal Marsden NHS Foundation Trust, 2013). If they were to inherit their mother’s BRCA2 mutation, however, R.M.’s two daughters and son could choose to take any of the above-mentioned precautions. If he is between the ages of 40 and 50, for example, R.M’s son could choose to have an annual digital rectal exam. Having gained knowledge on his inherited BRCA2 mutation, he could take action to reduce his risk of getting breast and/or prostate cancer. Nevertheless, genetic testing for breast cancer susceptibility may not be for everyone. In fact, Susan G. Komen (2015) recommends that only those who had breast cancer at an early age, whose family member had breast cancer at an early age or ovarian cancer at any age, or who are of Ashkenazi Jewish descent be tested, for their chance of having a BRCA1 or BRCA2 gene mutation is greater. That being said, R.M. chose to be tested because her aunt died from ovarian cancer at age 59, and her mother died from breast cancer at age 56 (Harding, Snyder, & Preusser, p. 447). Similarly, R.M.’s children may choose to be tested, for they have a positive maternal history of both breast and ovarian cancer, and their mother, who is a first-degree relative of theirs, has stage III ovarian carcinoma. And, according to Memorial Sloan Kettering Cancer Center (2016), it would be wise of them to do so. For if they were to test positive and have regular screenings, they may be able to prevent cancer or find it at an early stage. This is especially important for R.M.’s daughters, who, after testing positive for the presence of a BRCA2 mutation, would be aware of their increased risk for ovarian cancer. Ovarian cancer, which is referred to as the “silent killer,” and occurs when cells in the ovaries begin to grow out of control, is hard to detect, for its symptoms are often attributed to far IMPLICATIONS OF GENETIC TESTING 5 less serious conditions (Knox, 2007). For example, the most common symptoms, which include bloating, pelvic or abdominal pain, trouble eating or feeling full quickly, and urinary urgency or frequency, are often linked to menopause, aging, dietary indiscretions, stress, depression, and/or functional bowel problems (Ovations for the Cure of Ovarian Cancer, 2016). In their research article, John Schorge, Christopher McCann, and Marcela Del Carmen (2010) suggest that, as a result of this, “substantial delays prior to diagnosis are very common” (p. 111). Perhaps, that is why R.M.’s cancer went undiagnosed for such a long time. For it is feasible, at least according to Pietrangelo’s research (2014), that both R.M. and her doctor attributed her vague and nonspecific symptoms to her growing older. In spite of this and as mentioned above, it would be beneficial for her two daughters to be genetically tested, for if they tested positive and chose to have more frequent screenings ovarian cancer, if developed, could be detected early and treated more effectively (Royal Marsden NHS Foundation Trust, 2013). And perhaps, if R.M.’s daughters were more attune to these digestive disruptions and urinary problems, they could prevent a progression of the disease similar to that of their mother’s, which reads as follows: R.M. begins a chemotherapy regimen of paclitaxel (Taxol) and cisplatin (Platinol). After receiving the fourth course, she presents with shortness of breath, complaints of nausea, and early satiety with a recent weight loss of 10 pounds. Her abdomen is distended, and her SpO2 is 86% on room air. Her current CA-125 level is 328 units/mL. You are admitting her directly from the oncologist’s office to the medical floor. (Harding, Snyder, & Preusser, p. 448). While nausea, weight loss, and feeling full are known side effects of ovarian cancer and its treatments, shortness of breath and decreased oxygen saturations are not (American Society of IMPLICATIONS OF GENETIC TESTING 6 Clinical Oncology, 2015a). Instead, they are indicative of a worsening disease state, as is R.M.’s CA-125 level. According to the Foundation for Women’s Cancer’s (2011) clinical guideline, CA-125 is “a substance found in the blood called a glycoprotein (a sugar associated protein)” (p. 1). It provides information about the state of ovarian cancer and is obtained by taking a blood sample. It is most commonly used throughout the course of chemotherapy to measure treatment effectiveness (p. 3). However, it can also be used to screen for ovarian cancer in high-risk women, and recurrent cancer in women who have been previously diagnosed. And while it can and does fluctuate, normal levels usually fall between 0 and 35 units/mL (King, 2015). An elevated level, says Melissa Conrad Stöppler (2016), signifies tumor recurrence. Conversely, a decreased level indicates that therapy has been effective. And so, in R.M.’s case, the CA-125 level is viewed negatively, for it suggests that her cancer is intensifying. Having gone from a level of 69 units/mL to one of 328 units/mL, she may have a tumor. And her other symptomology, such as her shortness of breath and SpO2 of 86%, imply that it may be metastasizing. For though they could be signs of an allergic reaction, they could also signify an advanced malignancy. And her chest x-ray film, which revealed bilateral pleural effusions, confirms this, for pleural effusions are a common complication of advanced malignancy (Musani & Langmack, 2016). “This buildup of fluid between the layers of tissue that line [her] lungs and chest cavity,” and her associated dyspnea, cough, and chest pain indicate a poor prognosis (Hadjiliadis, 2014). In fact, it may signify that she is entering into the final stage of her illness. Knowing that her disease is progressing, and that, as a result, she has a reduced number of blood cells in circulation, R.M. should be carefully monitoring her health. She should be developing an increased awareness of the symptoms of low blood counts, for the IMPLICATIONS OF GENETIC TESTING 7 chemotherapeutic agents she is receiving, such as paclitaxel (Taxol) and cisplatin (Platinol), not only destroy rapidly dividing cells (cancerous cells), but also affect her normal cells, such as her red blood cells, white blood cells, and platelets. That being said, she should be on the look out for signs that her blood cell counts are low. If she is feeling fatigued, dizzy, or lightheaded, she should take note. Additionally, if she has dark, amber-colored urine, bleeding gums and mouth ulcerations, or numbness in her lower legs bilaterally, she should recognize that these are symptoms of the chemotherapeutic agents. If, however, she develops an increased temperature, such as one of 101.8 ° F (38.8° C), she or the person caring for her should contact her oncologist immediately (UNM Cancer Center, 2016). Likewise, according to Julia Warr, Amanda Hird, Carlo DeAngelis, Angie Giotis, and Yoo-Joung Ko’s (2013) research article, R.M.’s oncologist should order a Complete Blood Count (CBC) to determine whether additional treatments, such as blood transfusions, are necessary before the initiation of therapy. Also, to treat the abovementioned pleural effusions, R.M.’s provider should consider performing a thoracentesis, in which the fluid would be removed from the pleural cavity with a needle. Or he could insert a chest tube to drain the fluid from the pleural space, or administer a diuretic, which would increase the excretion of water from the body (Musani & Langmack, 2016). Additionally, if an underlying infection is present, he could prescribe an antibiotic. Regardless, R.M.’s provider should plan to address these effusions, so as to rid or lessen her discomfort. And according to Mariann Harding, Julie Snyder, and Barbara Preusser (2016) her oncologist does just that, for the case study progresses as follows: After performing a thoracentesis, the oncologist orders a magnetic resonance imaging (MRI) scan of the chest, abdomen, and pelvis, which reveals a mass in the left lower quadrant and a malignant bowel obstruction. He immediately schedules R.M. for a tumor IMPLICATIONS OF GENETIC TESTING 8 debulking and possible placement of an ostomy. (p. 449). As talked about, R.M has an advanced disease and her prognosis is poor. And so, prior to performing said palliative surgical interventions, R.M.’s oncologist would consult with her and her family about the likely outcomes, explaining to them that the reason for his debulking the tumor and placing an ostomy is to relieve R.M. of the complications of her cancer, such as ulcerations, obstructions, hemorrhages, and pain, not to cure it. He or another member of the staff may mention to R.M., for example, that because her cancer has extended beyond her pelvis into her abdominal organs and, worse yet, into her lungs, the focus of her care has shifted (American Society of Clinical Oncology, 2015b). Using honest and informative communication, he would make clear to her that the goal, then, would be to provide her with emotional support and physical comfort. Additionally, having an ostomy placed on top of having had her ovaries, cecum, distal portion of her small bowel, and omentum removed recently, may negatively impact R.M.’s body image. And so, as Janice Hinkle and Kerry Cheever (2014) mention, he or the nurse may want to “exhibit interest, concern, and willingness to listen to [her] fears,” so as to help her progress through this difficult experience (p. 1446). Debulking, in and of itself, is considered a palliative surgical intervention, for it does not rid individuals entirely of their tumors. Instead, as much of their tumors as possible are removed, so as to treat their symptoms of advanced cancer, including pain and disability. And in this process, other parts of their diaphragm, and segments of their bowel, spleen, and liver may be removed (Marshfield Clinic, 2016). It makes sense then that R.M. may need to have an ostomy placed, for if a segment of her bowel were to be removed she would need a way for her stool to exit her body (Vasilev, 2014). Again, it is imperative that either the oncologist or nurse mention this in R.M.’s preoperative teaching. Additionally, it would be in R.M.’s best interest if along IMPLICATIONS OF GENETIC TESTING 9 with telling her about these surgeries and their accompanying risks, such as pain, infection, loss of organ function, and bleeding, they discuss with her what postoperative life might be like. They may choose, for example, to begin teaching on ostomy care, so as to help her and her family better assimilate to postoperative life. As Zimnicki (2015) mentions in her research article, “Preoperative Teaching and Stoma Marking in an Inpatient Population,” they may choose to educate R.M. and her family on the techniques used for cleansing stoma sites, or the signs and symptoms of complications, such as changes in bowel habits or bulging around the stoma, before surgery. Nonetheless, the four main points they should include in their teaching should be: the type of surgery, the aim of the surgery, what can be expected, and how the surgery is going to impact her life from here on out. And, say, they were to find R.M’s daughter crying quietly, telling them that she thought her mother was going to fight this, and that it is really hitting her that her mother is dying, their best response would be “let’s talk about what is going on with your mother’s illness,” as it would give her an opportunity to open up (Harding, Snyder, & Preusser, p. 449). To support her and her mother, the staff could ask them open-ended questions, which would encourage them to share their feelings and questions. It is important that they help them find ways to talk about their feelings, and so they may also recommend that they meet with a counselor to help them deal with this stressful situation. It may be beneficial, for example, for R.M.’s two daughters and son to seek counseling, so as to figure out how best they can adjust to losing their mother, and how their family roles may change. Overall, and regardless of whether they meet with a physician, nurse, or counselor, R.M. and her family should be made to feel comfortable and like they can openly talk about the situation at hand (American Cancer Society, 2014). And, perhaps, they should be IMPLICATIONS OF GENETIC TESTING 10 afforded the opportunity to meet with a hospice or palliative care team, so as to ensure that R.M. will be surrounded by love and comfort when she dies. The takeaway, however, would be to prevent this from happening to R.M.’s children. And so, to prevent R.M.’s two daughters and son from dying a death similar to that of their mother’s, which reads as follows, the medical staff should encourage them to be genetically tested, and if they receive a positive result, to be screened more frequently: R.M. undergoes the debulking procedure. Because of the presence of multiple small tumors that were not detected on preoperative scanning, the oncologist elects not to place an ostomy. R.M. never fully recovers from surgery and does not resume chemotherapy. She experiences recurrent bowel obstructions and passes away in hospice care 7 weeks later. (Harding, Snyder, & Preusser, 2016, p. 450). As mentioned in Lobb, Butow, Meiser, Tucker, and Barratt’s (2001) research article, they should be genetically counseled, and, if desired and necessary, able to take a hormonal therapy medicine or oral contraceptive, take advantage of more frequent clinical exams, and/or have prophylactic surgery. In summary, and as an implication of their mother’s having tested positive for a BRCA2 mutation and died of ovarian cancer at the age of 58, R.M.’s two daughters and son may want to be genetically tested. And it is the ethical and legal obligation of their care providers to recommend that they are, for they are at an increased risk of developing a similar mutation. Consequently, if they were to also test positive, they would be at a higher-than-normal risk of developing breast and/or other cancers. And so, as an anticipatory action, R.M.’s children should receive genetic counseling, so as to be made aware of how their genetics and mother’s death IMPLICATIONS OF GENETIC TESTING 11 affect them. They should be given a choice as to whether or not they would like to be tested. And if they are tested, and know their results, they should be supported in how they wish to proceed. IMPLICATIONS OF GENETIC TESTING 12 References American Cancer Society. (2014). Coping with advanced cancer. Retrieved from http://www.cancer.org/treatment/understandingyourdiagnosis/advancedcancer/advancedcancer-coping. American Society of Clinical Oncology. (2015a). Side effects of chemotherapy. Retrieved from http://www.cancer.net/navigating-cancer-care/how-cancer-treated/chemotherapy/sideeffects-chemotherapy. American Society of Clinical Oncology. (2015b). Ovarian cancer: Stages and grades. Retrieved from http://www.cancer.net/cancer-types/ovarian-cancer/stages-and-grades. Foundation for Women’s Cancer. (2011). Understanding CA 125 levels: A guide for ovarian cancer patients. Chicago, Illinois: Foundation for Women’s Cancer. Retrieved from http://www.foundationforwomenscancer.org/wp-content/uploads/CA125levels.pdf Greenberg, R. (2006). BRCA mutations and childhood cancer. Cancer Biology & Therapy, 5(9), 1103-1004. Hadjiliadis, D. (2014). Pleural effusion. National Institute of Health. Retrieved from https://www.nlm.nih.gov/medlineplus/ency/article/000086.htm. Harding, M., Snyder, J. & Preusser, B. (2016). Winningham’s Critical Thinking Cases in Nursing. (6th Ed.) St. Louis: Elsevier. Hinkle, J.L., & Cheever, K.H. (2014). Brunner & Suddarth’s Textbook of Medical-Surgical Nursing (13th ed.). Philadelphia: Lippincott Williams & Wilkins. King, G. (2015). CA 125. Retrieved from http://emedicine.medscape.com/article/2087557overview. IMPLICATIONS OF GENETIC TESTING 13 Knox, R. (2007). Ovarian cancer: Early diagnosis poses challenges. Retrieved from http://www.npr.org/templates/story/story.php?storyId=14721359. Lobb, E., Butow, P., Meiser, B., Tucker, K., & Barratt, A. (2001). How do geneticists and genetic counselors counsel women from high-risk breast cancer families? Journal of Genetic Counseling, 10(2), 185-199. Marshfield Clinic. (2016). Understand cancer surgery. Retrieved from https://www.marshfieldclinic.org/specialties/cancer-care/cancer-surgery. Memorial Sloan Kettering Cancer Center. (2016). Inherited risk for breast & ovarian cancers. Retrieved from https://www.mskcc.org/cancer-care/risk-assessment-screening/hereditarygenetics/genetic-counseling/inherited-risk-breast-ovarian. Musani, A., & Langmack, E. (2016). Management options for malignant pleural effusions. National Jewish Health. Retrieved from https://www.nationaljewish.org/about/mediacenter/newsletters/lungcancerfrontiers/article s/malignant-pleural-effusions/. National Cancer Institute. (2015). BRCA1 and BRCA2: Cancer risk and genetic testing. Retrieved from http://www.cancer.gov/about-cancer/causes-prevention/genetics/brcafact-sheet. Nelson, H., Pappas, M., Zakher, B., Priest Mitchell, J., Okinaka-Hu, L., & Fu, R. (2013). Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer in women: A systematic review to update the U.S. preventive services task force recommendation. Annals of Internal Medicine, 160(4), 255-266. Ovations for the Cure of Ovarian Cancer. (2016). Ovarian cancer—what you need to know. Retrieved from https://www.ovationsforthecure.org/aware/aware_facts.php. IMPLICATIONS OF GENETIC TESTING 14 Pietrangelo, A. (2014). Ovarian cancer: Early signs & symptoms. Healthline. Retrieved from http://www.healthline.com/health/cancer/ovarian-cancer-early-signs#Treatment6 Schorge, J. McCann, C., & Del Carmen, M. (2010). Surgical debluking of ovarian cancer: What difference does it make? Reviews in Obstetrics and Gynecology, 3(3), 111-117. Seeking your genetic information: Pros and cons. (2014). Retrieved from http://www.breastcancer.org/symptoms/testing/genetic/pros_cons. Stöppler, M. (2016). CA 125. Retrieved from http://www.medicinenet.com/ca_125/page2.htm. Royal Marsden NHS Foundation Trust. (2015). A beginner’s guide to BRCA1 and BRCA2. London: The Royal Marsden NHS Foundation Trust. Retrieved from https://www.royalmarsden.nhs.uk/sites/default/files/files_trust/brca_0.pdf. Susan G. Komen. (2015). Genetics and breast cancer. Retrieved from http://ww5.komen.org/uploadedFiles/_Komen/Content/About_Breast_Cancer/Tools_and _Resources/Fact_Sheets_and_Breast_Self_Awareness_Cards/Genetics%20and%20Breast %20Cancer.pdf. Susan G. Komen. (2016). BRCA1 and BRCA2. Retrieved from http://ww5.komen.org/BreastCancer/BRCA1andBRCA2.html#riskloweringoptions. UNM Comprehensive Cancer Center. (2016). Low blood counts. Retrieved from http://cancer.unm.edu/cancer/cancer-info/cancer-treatment/side-effects-of-cancertreatment/common-side-effects/low-blood-counts/. Vasilev, S. (2014). Colostomy and ileostomy in ovarian cancer: What are stomas? Retrieved from http://ovariancancer.about.com/od/surgery/a/stomacare.htm. IMPLICATIONS OF GENETIC TESTING 15 Warr, J., Hird, A., DeAngelis, C., Giotis, A., & Ko, Y. (2013). Baseline blood work before initiation of chemotherapy: What is safe in the real world? Journal of Oncology Practice, 9, 182-185. Zimnicki, K. (2015). Preoperative teaching and stoma marking in an inpatient population. Journal of Wound, Ostomy & Continence Nursing, 42(2), 165-169.