Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
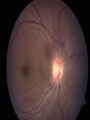
GRAND ROUNDS Denise A. John VEI 1/19/2007 Case HPI: 17 y/o ♀ s/p trauma OD ~ 2 wks earlier awoke in the AM with severe pain & vision OD. ROS: Headache & nausea x 2 days PMHX: Umbilical hernia Case POHX: Trauma OD Hyphema Commotio retinae Hemorrhagic choroidal detachment ø Surgery/lasers FHX: (-) SHX: ø Tobacco/ETOH Allergies: NKDA Meds: PF 1% qid OD; stopped atropine 1% a wk earlier Case 20/400 NI VAsc 20/30 Motility: Full OU 52 IOPA 16 Pupils: Moderately dilated & sluggish OD; ø RAPD Differential Diagnosis Hyphema Traumatic iritis Traumatic glaucoma Lens-induced Ghost cell Trabecular meshwork damage/Angle recession Steroid response Closed cyclodialysis cleft Case External exam: Unremarkable OU SLE: OD: 2+ conjunctival injection; corneal MCE; AC deep & formed with rare cell; multiple iris sphincter tears; lens clear & centered; trace pigmented vitreous cells OS: Unremarkable DFE Summary Recent history of blunt trauma OD with period of IOP with the development of a hemorrhagic choroidal detachment, optic disc edema, retinal venous engorgement & macular striae now with IOP. What is your diagnosis? What would you like to do next? Case Assessment: Spontaneous closure of a cyclodialysis cleft with IOP Plan: IOP to 32 (alphagan/cosopt/diamox) in clinic Sent home on glaucoma gtts/diamox/PF & atropine F/u 3 days Cyclodialysis: Pathophysiology Blunt trauma: Axial compression & rapid compensatory equatorial expansion Cyclodialysis: Pathophysiology Separation of the longitudinal ciliary muscle fibers from the scleral spur Uveal-scleral outflow Cyclodialysis Uncommon Etiology: Accidental Blunt ocular trauma Ocular surgeries involving manipulation of the iris tissue Intentional Glaucoma management Surgical Cyclodialysis Heine,1905: Alternative to filtering surgery, esp. in aphakic glaucoma Unpredictable results Complications: Hemorrhage, stripping of Descemet’s, corneal damage, tearing of the iris/ciliary body, lens injury & vitreous loss & phthisis Cyclodialysis: Complications Hypotony (IOP < 6) Internal filtration, aqueous production or both Often stabilizes in a few weeks Magnitude of hypotony ø proportional to size of cleft Variable VA Transudation of protein-rich fluid into the subretinal space in posterior pole Statistical association between IOP < 4 & VA < 20/200 Cyclodialysis: Complications Shallow AC Induced hyperopia Cataract Choroidal effusion Retinal & choroidal folds Engorgement & stasis of retinal veins CME Optic disc edema Diagnosis Clinical Gonioscopy Often small < 4 clock hrs White band (sclera) below the TM Ultrasound biomicroscopy (UBM) Resolution with higher frequencies at the expense of depth of penetration 50MHz transducer 50 μm resolution 5mm penetration Accurate assessment of location & size Cyclodialysis: Management Goal: Reverse hypotony Indications for treatment: Hypotonous maculopathy + disc edema Macular folds Choroidal detachment Corneal edema + worsening vision Cyclodialysis: Medical 1st line treatment Duration: 6 wks Topical long-acting cycloplegic 1% Atropine Corticosteroids ø indicated Cyclodialysis: Laser Argon laser photocoagulation (Joondeph,HC; 1980) 400-800mW 200μm spot size 0.1-0.2 sec Transscleral YAG laser cyclophotocoagulation (Brooks et al.; 1991) 6 J power 20 applications 2-3mm behind limbus Cyclodialysis: Surgical Techniques Ciliochoroidal diathermy Direct cyclopexy Indirect cyclopexy (McCannel retrievable suture) Iris-base inclusion cyclopexy Anterior scleral buckle Vitrectomy/cryotherapy/gas tamponade Cyclodialysis: Hypotony Management Aminlari et al , 2004, described the management of 7 pts with a cyclodialysis cleft Etiology of cyclodialysis cleft 1 eye: blunt trauma 5 eyes: s/p ECCE 1 eye: s/p trabeculotomy Duration of ocular hypotony (IOP range 0-6mmHg) 2 pts: 1-2 wks 3 pts: 3-5 mos 2 pts: > 1yr VA pretreatment: Range 20/50-20/100 Cyclodialysis: Hypotony Management Management 4/7 eyes: Medical tx (atropine 1% BID-TID) alone 2 eyes: 2 treatments of argon laser (1 wk apart) due to ø response atropine tid-qid Hypotony reversed in 4 days 1 eye: Surgical closure (direct cyclopexy) Hypotony reversed within 1 wk Pediatric pt unable to cooperate at slitlamp for laser Hypotony reversed POD#1 VA post-treatment: Range 20/20-20/60 Cyclodialysis: Management Algorithm 1. Medical tx 2. Laser 3. Repeat laser Ormerod et al, 1991 Small cleft (< 2 clock hrs) 1. Direct cyclopexy 2. Ciliochoroidal diathermy 3. Indirect cyclopexy Medium cleft (2-4 clock hrs) Large cleft (> 4 clock hrs) 1. Direct cyclopexy 2. Ciliochoroidal diathermy 1. Direct cyclopexy 2. Anterior scleral buckle Cyclodialysis: Management Cyclodialysis cleft may close spontaneously due to… Inflammatory response hyphema Cycloplegia May occur within first 6 wks More common in children Cyclodialysis: Management Following resolution, a self-limited ocular hypertension is common within the first 2 wks IOP rarely > 45mmHg Miotics are contraindicated Cyclodialysis: Prognosis Vision often improves after hypotony is corrected (IOP: 6-12mmHg) Best results with early correction Vision may improve rapidly or take months Delay of treatment > 8 wks the risk of losing 1-3 snellen lines of vision Back to our patient… VA 20/60; IOP nrl on f/u appt. Tapered pred forte; atropine continued; glaucoma gtts/diamox stopped ~ 2 wks after IOP normalized, recurrence of IOP (38); VA 20/50+2; glaucoma gtts resumed; PF/atropine stopped ~ 2 wk f/u IOP normalized; VA 20/25-2; glaucoma gtts continued Follow-up 3 mos Take home points… Cyclodialysis cleft should be considered with IOP in setting of blunt trauma. Closed cyclodialysis cleft should be considered with IOP and a history of blunt trauma (within 6 wks) and IOP with signs of hypotony maculopathy &/or choroidal detachment. Hypotony is the major complication & is responsible for vision loss. A hypotonous cyclodiaysis cleft without retinopathy does not require treatment. Goal of treatment is to reverse the hypotony Medical treatment is the primary form of management for the first 6 wks. References Ormerod et al. Management of a hypotonous cyclodialysis cleft. Ophth 1991; 98 (9): 1384-93 Tran et al. UBM in the diagnosis & management of cyclodialysis cleft. Asian J Ophth, Vol. 4 (3) 2002; 11-15 Hansen et al. Visualized cyclodialysis: an additional option in glaucoma surgery. Acta Ophth. 1986; 64: 142-45 Joondeph HC. Management of postoperative & post-traumatic cyclodialysis clefts with argon laser photocoagulation. Ophth Surg. 1980; 11: 186-88 Brooks et al. Noninvasive closure of a persistent cyclodialysis cleft. Ophth.1996; 103: 1943-45 Aminlari et al. Medical/surgical/laser management of cyclodialysis cleft. Arch Ophth. 2004; 122; 399-404 Alward. Color Atlas of Gonioscopy. AAO. 2001 BCSC. Glaucoma. AAO. 2004-5 Yanoff. Traumatic Glaucomas. 2nd Ed. 2004 Allingham et al. Shield’s testbook of glaucoma. Traumatic Glaucomas. 5th Ed. 2005