Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Department of OUTCOMES RESEARCH
Clinical Research Design
Systematic Reviews
and
Meta-analysis
Daniel I. Sessler, M.D.
Michael Cudahy Professor and Chair
Department of OUTCOMES RESEARCH
The Cleveland Clinic
Literature Reviews
Reviews are important
• Often too much primary literature
• Clinicians cannot critically review all literature
Classical reviews
• Informed synthesis by authors
– Most helpful when authors are experts and active investigators
• Excellent perspective
– Integrates historical development with future directions
• Typically restricted to best relevant articles
• Most suitable for reviewing an entire field
• Subject to author(s) bias
Systematic Reviews
Useful for specific interventions & outcomes
• Specific, important, and sensible question essential
• Equally effective for complications and therapeutic outcomes
Standardized search of all relevant work
• Documented and reproducible selection process
• Tabular presentation, often stratified by
– Research approach
– Study quality
– Population
– Outcome
Synthesis can be
• Qualitative, based on authors’ expertise (and bias)
• Quantitative: meta-analysis
Meta-analysis
Statistical summary of systematic review
• Effect size and significance
• Patient level (patient pooling) or study level (aggregate stats)
– Individual patient data preferable, but rarely available
Usually used for randomized trials
• Can be used for observational studies— with great caution
Studies must evaluate similar treatment & outcomes
Suitable for various types of data
• Dichotomous, continuous, risk difference, relative risk, etc.
Generalizability good; internal validity variable
Data-acquisition
Individual studies are unit of analysis
• Summary statistics are the data elements
Consider studies to be like patients in a trial
• Rigorous a priori inclusion and exclusion criteria
Specify search strategies and sources of studies
• Which databases? Search terms?
• Language restrictions?
• Randomized trials only?
• Primary outcomes only?
• Published versus unpublished?
Specify adjudication methods
Sample Data-extraction Form
Population
Comparison
• Treatment
• Active vs. placebo
Outcome(s)
Measures of quality
Surprisingly difficult
• Adjudication critical
Evaluating Study Quality
No good way
• Many design errors non-obvious or subtle
Various scoring systems used; points for
• Legitimate randomization
• Concealed allocation
• Blinded outcome evaluation
• Drop-outs and reasons described
Standard-of-care: report quality of included studies
Reporting Search Results
Major Sources of Error
Garbage in, garbage out
• Meta-analysis never better than underlying studies
• Cannot correct for methodologic errors or bias
Reporting bias
• Changed or omitted primary outcomes
• Significant findings 2.2-4.7 X more likely to be complete (Dwan 2008)
Subtle (or not) treatment & measurement differences
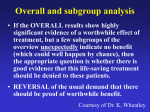
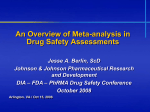
Publication bias
• Large trials are almost always published
• Positive studies usually published even if under-powered
• Small negative studies less likely than others to be published
– Censoring by authors or corporate sponsors
– Appropriate editorial decision, but unpublished studies disappear
– Meta-analysis depends on knowing about all relevant results
Funnel Plots
SE of
Log(OR)
Log(OR)
Heterogeneity
Data: variation in study results exceeding chance
Biology: true differences related to methodology
• Differences in populations: age, gender, ethnicity, etc.
• Differences in drug dose (or drug within a class)
• Unappreciated patient factors
Tests: chi square, etc.
Analysis strategies
• Minor heterogeneity
– Report amount
– Combined analysis may be sensible
• Treat serious heterogeneity as an interaction
– Stratify analysis as for other effect modifiers
Analysis Strategies
Fixed-effects model
• Assumes all trials share same underlying treatment effect
– Treats each trial as random samples from one large trial
– Differences in results due to chance alone
• Similar to Mantel-Haenszel
• Often over-estimates significance
Random-effects model
• Assumes each study estimates a unique treatment effect
– That is, may truly differ from other included studies
– Allows heterogeneity, and is required for heterogeneous data
• Weights smaller studies more heavily
• Generally provides similar effect estimate with lower precision
– More conservative; probably should always be used
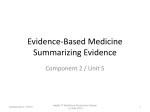
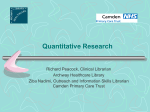
Forest Plots
Log weighted mean
effect ≈ sum of {log
(effect)/variance)}
for individual
studies, divided by
sum of 1/variance
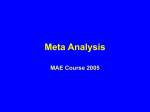
How Good are Meta-analyses?
“Large” defined by n≥1,000 “Large” defined by power
Generally, pretty good. But not perfect.
Cappelleri, JAMA 1996
Meta-analyses Increasingly Common
Most published as part of systematic reviews
Increasingly included in trial reports
• Objective comparison of current to previous results
Grant applications
• Summarize knowledge
• Support equipoise
• Need for proposed trial
• Complications unlikely
Blood loss with lowdose perioperative
aspirin
Cochrane Collaboration
International non-profit, 1993
Repository for meta-analyses
Standardized reporting
• QUORUM (1999)
• PRISMA (2009)
Provides free software
Evidence-based med movement
• David Sackett
• Gordon Guyatt
• Tom Chalmers
Archie Cochrane
Summary
Systematic reviews
• More objective than “expert” reviews
• May lack expert perspective and subtlety
• Meta-analysis is quantification of systemic review
Subject to major errors
• Any problems with underlying studies remain
• Publication and reporting bias can be substantial
• Heterogeneity can complicate analysis
Conduct and report per guidelines
Useful summary of available literature
• Especially when many similar studies are available
Department of OUTCOMES RESEARCH