Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Where does the money come from
in Radiology?
An Application of Relative Value Units (RVUs)
A Special Thank You to:
Dr. David M. Yousem, M.D., M.B.A. Professor, Department of
Radiology Vice Chairman of Program Development Director of
Neuroradiology Johns Hopkins Hospital
for allowing the use of his material/content in this presentation
Dr. Yousem’s online lecture series can be viewed at:
http://webcast.jhu.edu/mediasite/Catalog/pages/catalog.aspx?catalogId
=7e18b7d5-9c63-487e-aaf1-77a86f83b011
Dr. Yousem’s project was funded through an RSNA Educational Grant
Relative Value Units and the RBRVS – A Brief Review
• RVUs are assigned to specific CPT codes
• The total radiology bill has two components
– Technical Fee
• Paid to the facility (owner/operator of the equipment)
– Professional Fee
• Physician Work, Practice Expense, and Malpractice Expense
• RVUs do not translate directly into money
– Modified by geographic and budgetary multipliers
– Money Paid = (RVU x GPCI) x Conversion Factor
Medicare – There are (usually) two bills for every study
•
•
•
•
Medicare Part A
– Submitted by the “facility” performing the study
– Technical component
Medicare Part B
– Submitted by the interpreting physician
– Professional component
Patient pays 20% of both bills, Medicare covers 80% of both
– The patient may have supplemental insurance to cover their 20%
Global Reimbursement
– For the freestanding entity that may bill for both the technical and
professional components of the CMS Physician Fee Schedule under
Medicare Part B
Follow the Money
• Over the next few slides we will create a simplified example of
the reimbursement process
• Certain assumptions will be made to facilitate understanding the
numbers on a fundamental level
• As always, reality is much more complicated
• To start, we will try to answer the following question:
– How many studies do I have to read each day to make
$300,000 in a year?
Follow the Money – Assumptions
• Net payment per RVU of $30
– This allows for incomplete collections in a mixed payer population
– Calculated across all departments within a practice
• Goal personal income of $300,000
– Benefits amount to 25% of salary
– Malpractice costs are $25,000 (high end of the scale)
– Cash allowance of $10,000 (meetings and travel)
– Practice Expenses of 35%
• Based on survey data from the ACR and median reported
expenses per FTE radiologist
Follow the Money – Assumptions continued
• Work Days
– 250 workable weekdays a year
– 50 days for vacation and/or meetings
– 5 weekends of coverage
– Total of 220 work days
• CMS Physician Fee Schedule RVU files for 2010
• Geographic Practice Cost Index (2010)
– GPCI (physician work) in North Carolina is 1.0
• Conversion Factor (2010)
– $36.0846
Follow the Money – The Challenge
• Our hypothetical radiologist must produce $515,000 in a year
– This covers his salary, group benefits, and expenses
– Stated another way
• $2,341 a day
Follow the Money – The Details
•
Using the CMS formula for reimbursement
$ = RVUprofessional x GPCI x CF
•
We break it down into parts
– In our case, the payment per RVU reflects the GPCI and CF modifiers
$510,000 = Payment per RVU x RVUtotal
RVUtotal = Sum of {RVUstudy x Number of each type of study}
•
To break it down further into the workload required in a single day
$510,000 / 220 days = $2,341/day
Number of studies = $2,341 / (RVUstudy x Payment per RVU)
Follow the Money – The Details
• The previously described equations are calculated to show how
many of one specific study (e.g. Chest Radiographs) must be
read in a single day to meet the goal income
• Calculating a mix of studies is simple, but less illustrative
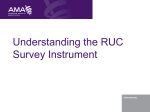
Follow the Money – The Work
•
•
Using only the professional
component of reimbursement,
these are the numbers of each
type of study you would have to
read in a single day to produce
$2,341 of income for your
practice
Specifically, if you are a
neuroradiologist, and only read
noncontrast Head CTs, you
would have to interpret, and be
reimbursed, for 68 exams to
meet your goal
Exam
RVU
(prof)
Number /
Day
CXR (2 view)
0.3
260
CT Head wo
1.14
68
CT A w/wo
1.89
41
MR Head w/wo
3.18
25
MR Knee wo
1.86
42
Xray Hand
0.24
325
US Abd Complete
1.09
72
NM HIDA
1.11
70
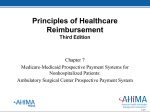
Follow the Money – Own the Equipment
•
•
•
The aforementioned examples
are for reimbursements with only
the professional component
The technical component of
reimbursement reflects 85% of
the global bill compared to the
professional component’s 15%
Here are the numbers again
when receiving the global
reimbursement (e.g. if all
imaging was performed at your
outpatient imaging center)
Exam
RVU (prof)
# / Day
RVU (global)
# / Day
CXR (2 view)
260
103
CT Head wo
68
22
CT A w/wo
41
10
MR Head w/wo
25
6
MR Knee wo
42
9
Xray Hand
325
96
US Abd Complete
72
22
NM HIDA
70
10
Conclusions
• Study volume is important to produce revenue
• So are your payer mix and contracts
– Medicare vs. Medicaid vs. Private Insurance
• Efficiency in Billing and Collections is essential to actually receiving
the revenue you have “earned”
– Accounts Receivable is an critical asset (see Accounting)
• Owning the equipment is crucial
– This is the basis of turf wars between radiology and some other
clinical subspecialties
– ACR has ongoing legislative efforts at closing Stark law
loopholes
The Big Picture
•
•
Managing a practice with multiple radiologists exponentially increases
the complexity of generating and measuring income
– Referral Base influences the RVU calculations and billing
• Inpatient vs. Outpatient and Medicare vs. Private Insurance
• Hospital vs. Imaging center vs. Physician Office
– Productivity Measurement and other Metrics
As well, there are many facets to both Accounting and Expenses
• Capital Purchases
• Marketing
• Technology
• Medicolegal and Legislative Issues