Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
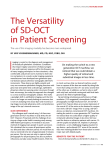
■ B R I E F Spectral Domain Optical Coherence Tomography Imaging of Retinal Diseases in Singapore Mandeep Singh, MRCSEd Caroline K. L. Chee, FRCSEd ABSTRACT In this retrospective case series, the authors reviewed cases of patients with macular disorders whose eyes had been imaged using spectral domain optical coherence tomography (SD-OCT) (Cirrus HD-OCT; Carl Zeiss Meditec, Inc., Dublin, CA). SD-OCT images were obtained from patients with a variety of ocular conditions attending a tertiary retinal clinic in Singapore from August 2007 to December 2007, according to standardized protocols. Images of 428 eyes from 301 patients were reviewed. Ocular diagnoses included diabetic macular edema, exudative age-related macular degeneration, central serous chorioretinopathy, cystoid macular edema, retinal vein and artery occlusions, infective chorioretinitis, and others. The authors present four cases of particular interest to illustrate how SD-OCT was useful in complementing the clinician’s assessment of macular disease. [Ophthalmic Surg Lasers Imaging 2008;39:S120-S125.] INTRODUCTION Optical coherence tomography (OCT) is a noninvasive imaging modality that provides high-resolution, cross-sectional images of the retina. Its principles have been described elsewhere.1,2 It enables clinicians to diagnose and monitor a number of retinal diseases.2-6 From the Department of Ophthalmology National University Hospital, Singapore (MS, CKLC), and the Department of Ophthalmology, Yong Loo Lin School of Medicine, National University of Singapore (CKLC). Accepted for publication March 14, 2008. The authors have no grant support to acknowledge or financial interest to disclose. Address correspondence to Caroline K. L. Chee, FRCSEd, Department of Ophthalmology, National University Hospital, 5 Lower Kent Ridge Road, Singapore 119074. S120 R E P O R T ■ Conventional time domain OCT (TD-OCT) is limited by suboptimal image resolution, slow data acquisition, and poor image registration. The recent introduction of spectral domain OCT (SD-OCT) has enabled imaging with greater resolution, higher scan speed, wider sampling area, and improved image registration.7,8 Here, we reviewed cases of patients with retinal disease whose eyes had been imaged using SD-OCT (Cirrus HD-OCT; Carl Zeiss Meditec, Inc., Dublin, CA) to determine the clinical utility of this imaging device in the assessment of patients with retinal disorders. DESIGN AND METHODS In this retrospective case series, we reviewed the records of all patients who had undergone SD-OCT imaging of the retina from August 2007 to December 2007 at a tertiary retinal clinic in Singapore. Most eyes were also concurrently imaged using TD-OCT (Stratus OCT; Carl Zeiss Meditec, Inc.); in these cases, we compared the quality and clinical utility of data obtained using each method. In all cases, imaging was performed using standardized protocols: the Fast Macular Thickness Map protocol was used for Stratus OCT (scan length, 6.0 mm; axial resolution, 10 µm) and the 512 × 128 Macular Cube protocol for Cirrus HD-OCT (scan area, 6.0 × 6.0 mm2; axial resolution, 5 µm). Fundal fluorescein angiography (FA) and indocyanine green angiography (ICGA) were performed at the clinician’s discretion. To facilitate image review, SD-OCT images were color-, brightness-, and contrast-adjusted until optimal clarity of detail was obtained. TD-OCT and SD-OCT images were reviewed and correlated with data from clinical examination and investigations. Here, we discuss four cases of particular interest to illustrate how SD-OCT imaging contributed significantly to the clinician’s understanding of the disease. Institutional review board approval was not obtained because this study was retrospective, involved the use of devices (Cirrus HD-OCT and Stratus OCT) that were in routine clinical use, and did not involve randomization of patients. FINDINGS SD-OCT images of 428 eyes from 301 patients with various ocular conditions were reviewed. Diagnoses OPHTHALMIC SURGERY, LASERS & IMAGING · JULY/AUGUST 2008 · VOL 39, NO 4 (SUPPLEMENT) A B C D E F G Figure 1. A, Submacular hemorrhage, OD, in a 68-year-old woman with VA CF at 1 m, OD. The white line denotes the location of TD-OCT and SD-OCT images shown in C, D, F, and G. B, ICGA showed polypoidal choroidal vasculopathy, OD. The white line denotes the location of the SD-OCT image shown in E. C, TD-OCT showing macular RPE and retinal detachment with intraretinal edema 3 days after intravitreal injection of perfluoropropane (C3F8) gas and tissue plasminogen activator. D, SD-OCT showed the location and extent of the RPE detachment in greater detail. Subfoveal fluid is also better seen with SD-OCT. E, The polyps were not visualized on SD-OCT images at the location suggested by ICGA (white arrow). Only irregularity and thickening of the outer retinal hyperreflective layers corresponding to RPE were seen at this site. F, One month after direct argon laser photocoagulation of polyps, TD-OCT showed widening of the hyperreflective layers in the outer retina, RPE detachment, and mild retinal thickening. G, SD-OCT of the same eye in Fig. 2A clearly showing RPE detachment and a hyperreflective subfoveal area above the RPE (white arrow) not visualized on TD-OCT. included diabetic macular edema, exudative age-related macular degeneration, central serous chorioretinopathy, cystoid macular edema, retinal vein and artery occlusions, infective chorioretinitis, and others. SD-OCT images had greater resolution than TD-OCT and imaged a greater area of retina in each scan. Topographic retinal thickness and retinal pigment epithelial (RPE) maps in the SD-OCT yielded more information than similar depictions on TD-OCT. The localization capability of the crosshairs of SD-OCT was useful in locating lesions across an area of imaged retina and could be used in conjunction with angiographic findings. There was improved patient cooperation with SD-OCT owing to BRIEF REPORT fast data acquisition. Optimal resolution of outer retinal layers was found when SD-OCT images were modulated to a grayscale output and contrast and brightness were adjusted for each image. In this manner, the layers of the retina, especially the outer retinal hyperreflective layers near the RPE and photoreceptor inner segment/ outer segment junctions, appeared maximally distinct and separate. We discuss four interesting cases in detail below to illustrate these differences. Polypoidal Choroidal Vasculopathy A 68-year-old, nonsmoking woman presented with poor vision in the left eye for 10 days. Visual acu- S121 C A B Figure 2. A, A 16-year-old Indonesian boy with Toxoplasma chorioretinitis had a pale retinal lesion OD at the fovea and overlying vitritis with a “headlight-in-the-fog” appearance and a chorioretinal scar on the inferior macula. The white line denotes the location of scans shown in C–E. The black line denotes the location of the scan shown in F. B, FA showed ring-shaped foveal leakage and staining corresponding to the inferior macular scar. C, TD-OCT showed retinal thickening, loss of normal foveal contour, and shadowing of the subfoveal RPE layer. Central macular thickness (CMT) was 400 µm. D, Two months after beginning oral anti-Toxoplasma therapy, TD-OCT showed reduced retinal thickening with a CMT of 276 µm. E, SD-OCT showed features not seen on TD-OCT such as intraretinal cysts, loss of normal intraretinal striations in the fovea, thickened posterior hyaloid with foveal vitreomacular traction, epiretinal membrane, and attenuation of the hyperreflective layer corresponding to subfoveal RPE. F, In the same macular cube SD-OCT image, thinning of the retina, loss of the hyperreflective layers of the outer retina, and increased light transmission to the choroid through this atrophic area were seen. D E F ity (VA) was counting fingers (CF) 1 m in the left eye due to a large submacular hemorrhage (Fig. 1A) attributable to polypoidal choroidal vasculopathy (Fig. 1B). She received an intravitreal injection of perfluoropropane (C3F8) gas and tissue plasminogen activator. Three days later, the hemorrhage had displaced, and VA was 20/30 in the left eye. TD-OCT showed macular RPE detachment, subretinal fluid, and retinal thickening (Fig. 1C). SD-OCT showed more precisely the extent of RPE detachment underlying the foveal detachment (Fig. 1D). The cross-hairs of the SD-OCT scan output were placed over the polyps as guided by ICGA. The polyps were not visualized on SD-OCT images; irregularity and thickening of outer retinal hyperreflective layers were seen at this site (Fig. 1E). Direct argon laser photocoagulation of the polyps was performed. At 1 month, VA was 20/50 in the left eye. S122 TD-OCT showed widening of the hyperreflective layers in the outer retina, RPE detachment, and mild retinal thickening (Fig. 1F). SD-OCT provided more detailed information, showing RPE detachment and a hyperreflective subfoveal layer above the RPE (Fig. 1G) possibly representing altered subretinal blood or scar that was not visualized on TD-OCT. Toxoplasma Chorioretinitis A 16-year-old boy from East Java, Indonesia, presented with 8 days of visual loss in the right eye. VA was CF 0.5 m in the right eye. There was a pale retinal lesion at the fovea and overlying vitritis with a “headlight-in-the-fog” appearance, and a chorioretinal scar on the inferior macula (Fig. 2A). FA is shown in Fig. 2B. TD-OCT showed retinal thickening, loss of normal foveal contour, and shadowing of OPHTHALMIC SURGERY, LASERS & IMAGING · JULY/AUGUST 2008 · VOL 39, NO 4 (SUPPLEMENT) B A C D E Figure 3. A, FA in a 70-year-old man with VA 20/40, OD, showed a vascularized RPE detachment. The black line denotes location of scans shown in B–D. B, TD-OCT showed a large RPE detachment and minimal retinal thickening. C, SD-OCT showed RPE irregularity and thickening in the region of the choroidal neovascularization. D, After 2 months with no treatment, SD-OCT showed collapse of the RPE detachment, corrugation of RPE and retina, and intraretinal edema. E, The topographic RPE map of the SD-OCT at 2 months showed this morphologic change clearly. the subfoveal RPE layer (Fig. 2C). Central macular thickness (CMT) was 400 µm. Serology supported the diagnosis of Toxoplasma chorioretinitis. The patient received oral clindamycin with a tapering regimen of prednisolone over 3 months. At 2 months, there was a central foveal scar; VA was unchanged despite complete resolution of retinitis and vitritis. TD-OCT showed reduced retinal thickening with a CMT of 276 µm (Fig. 2D). SD-OCT showed in greater detail a number of features not seen on TDOCT, such as intraretinal cysts, loss of normal intraretinal striations in the fovea, thickened posterior hyaloid with foveal vitreomacular traction, epiretinal membrane, and attenuation of the hyperreflective layer corresponding to subfoveal RPE (Fig. 2E). The same 6 × 6-mm2 cube of the SD-OCT scan of the foveal lesion also captured the second lesion in BRIEF REPORT the inferior macula, showing thinning of the retina, loss of hyperreflective layers of the outer retina, and increased light transmission to the choroid through this atrophic area (Fig. 2F). Spontaneous Collapse of RPE Detachment A 70-year-old, nonsmoking man presented with poor vision in the right eye of uncertain duration. VA was 20/40 in the right eye with a large RPE detachment centered on the fovea. FA diagnosis was that of vascularized RPE detachment (Fig. 3A). TD-OCT showed a large RPE detachment and minimal retinal thickening (Fig. 3B). Guided by the FA, we located the choroidal neovascularization on SD-OCT where we found thickening and irregularity of the outer retina near the RPE (Fig. 3C). VA remained stable over 2 months with no treatment. SD-OCT at 2 months showed collapse of S123 ing showed thickening and increased reflectivity of the inner retina in the infarcted area. The inner retinal layers were not seen distinctly, and demarcation between normal and infarcted inner retina was unclear (Fig. 4A). Along the superior edge of the area of retinal infarction, SD-OCT showed areas of disruption of only inner retinal architecture demarcated from areas of normal inner retina (Fig. 4B). SD-OCT images also showed increased separation between inner retinal layers that were identified distinctly. Outer retinal morphology was relatively normal. At the completely infarcted inferior macula, outer retinal layers retained a normal appearance on SD-OCT despite complete inner retinal disorganization with increased reflectivity of inner retina, loss of inner retinal striations, and inner retinal thickening (Fig. 4C). The patient was treated conservatively and vascular risk factors controlled. A B DISCUSSION C Figure 4. A, In a 70-year-old man with inferior branch retinal artery occlusion OD, TD-OCT image across the fovea showed increased thickness and reflectivity of inner retina. The retinal layers in the outer and inner retina were not clearly seen. B, SD-OCT showed areas of disruption of inner retinal architecture (white arrows) interspersed with areas of normal inner retina along the superior edge of the area of inferior retinal infarction. C, In the completely infracted inferior macula, outer retinal layers retained a normal appearance despite complete inner retinal disorganization with increased reflectivity of inner retina, loss of inner retinal striations, and inner retinal thickening. the RPE detachment, full-thickness folds of RPE and retina, and intraretinal edema (Fig. 3D). The topographic RPE map of SD-OCT demonstrated this morphologic change clearly (Fig. 3E); there was no such output capability in TD-OCT. The patient was managed conservatively and maintained stable vision. Branch Retinal Artery Occlusion A 70-year-old man with hypertension presented with visual loss in the right eye for 3 days. VA was 20/200 in the right eye due to inferior branch retinal artery occlusion involving the fovea. TD-OCT imag- S124 As found by other investigators, TD-OCT and SD-OCT provided images of macular anatomy that added data to clinical assessment.9-11 SD-OCT images were of greater axial resolution than TD-OCT. This enabled detection of smaller lesions and improved resolution of larger lesions, compared with TD-OCT. Each SD-OCT macular cube scan is able to cover a greater area than TD-OCT line scans, enabling visualization of multiple lesions with a single scan. Patient cooperation is improved in the faster SD-OCT scans. The current practice of having to read SD-OCT output from the monitor attached to the device posed a minor inconvenience to clinicians, who had to walk to the machine to review results. We also found the lack of normative data in the SD-OCT unit at our center to be a disadvantage in that affected eyes could only be qualitatively compared with healthy eyes. This may be overcome in the future with the addition of normal retinal thickness values obtained in our population. SD-OCT is a useful tool in macular evaluation and provides more detailed anatomic information to the clinician than TD-OCT. The utility of SD-OCT imaging in clinical management of patients with retinal diseases needs to be further assessed. REFERENCES 1. Huang D, Swanson EA, Lin CP, et al. Optical coherence tomography. Science. 1991;254:1178-1181. OPHTHALMIC SURGERY, LASERS & IMAGING · JULY/AUGUST 2008 · VOL 39, NO 4 (SUPPLEMENT) 2. Puliafito CA, Hee MR, Lin CP, et al. Imaging of macular diseases with optical coherence tomography. Ophthalmology. 1995;102:217-229. 3. Hee MR, Baumal CR, Puliafito CA, et al. Optical coherence tomography of age-related macular degeneration and choroidal neovascularization. Ophthalmology. 1996;103:1260-1270. 4. Hee MR, Puliafito CA, Wong C, et al. Quantitative assessment of macular edema with optical coherence tomography. Arch Ophthalmol. 1995;113:1019-1029. 5. Hee MR, Puliafito CA, Wong C, et al. Optical coherence tomography of macular holes. Ophthalmology. 1995;102:748-756. 6. Hee MR, Puliafito CA, Wong C, et al. Optical coherence tomography of central serous chorioretinopathy. Am J Ophthalmol. 1995;120:65-74. 7. Drexler W, Morgner U, Kartner FX, et al. In vivo BRIEF REPORT 8. 9. 10. 11. ultrahigh resolution optical coherence tomography. Opt Lett. 1999;24:1221-1223. Drexler W, Morgner U, Ghanta RK, et al. Ultrahighresolution ophthalmic optical coherence tomography. Nat Med. 2001;7:502-507. Ko TH, Fujimoto JG, Duker JS, et al. Comparison of ultrahigh- and standard-resolution optical coherence tomography for imaging macular hole pathology and repair. Ophthalmology. 2004;111:2033- 2043. Swanson EA, Izatt JA, Hee MR, et al. In-vivo retinal imaging by optical coherence tomography. Opt Lett. 1993;18:1864-1866. Ko TH, Fujimoto JG, Schuman JS, et al. Comparison of ultrahigh and standard resolution optical coherence tomography for imaging of macular pathology. Ophthalmology. 2005;112:1922-1922. S125