Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
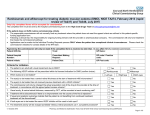
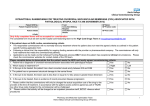
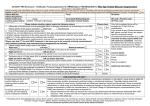
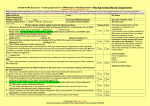
Notification for INTRAVITREAL ANTI-VEGFs for the treatment of WET MACULAR DEGENERATION AFLIBERCEPT (Eylea®) or RANIBIZUMAB (Lucentis®), NICE TAs 155 (updated June 2012) & 294 (Jul 2013) Patient NHS No. Patient Hospital Number: Patient initials Trust: Consultant Making Request: Consultant Contact Details: GP Name: GP Practice code: GP Post code: & DoB: Only fully completed forms will be accepted for consideration The completed form must be sent by the hospital commissioning team to the High Cost Drugs Team at [email protected] If the patient does not fulfil routine commissioning criteria The responsible commissioner will not normally fund any treatment where the patient does not meet the agreed criteria as outlined in this patient specific funding application form. Following a clinical trial, the responsibility for ongoing funding remains with the provider or pharmaceutical company. The commissioner will only fund treatment that meets the commissioned pathway. Applications can be made via the Individual Funding Requests process ONLY where the patient has exceptional clinical circumstances. Please check the commissioner websites for contact details of the IFR team. Please complete below to demonstrate that the patient meets the commissioning criteria: 1. Patient has wet age-related macular degeneration? 2. Which eye(s) is treatment for? 3. 3. What are the current visual acuity scores for each eye? Treatment will be routinely commissioned where best-corrected visual acuity in the eye(s) to be treated is between 6/12 and 6/96 (Snellen), in line with NICE TA 155 and TA 294 4. Confirm that there is permanent structural damage to the central fovea? 5. Confirm the lesion size is less than or equal to 12 disc areas in greater linear dimension? Lesion size (in disc areas) 6. Is there evidence of recent presumed disease progression (blood vessel growth, as indicated by fluorescein angiography, or recent visual acuity changes)? Please include any other relevant details: Pharmacy and Medicines Optimisation Team Herts Valleys Clinical Commissioning Group (HVCCG) Yes Right Right: No Left Left: Date: Yes Date: No Yes No Yes No Both 1 7. Is the eye(s) being considered for treatment anti-VEGF naïve? i.e. has previously not been treated with ranibizumab? Yes Please complete question 8 below 8. For eyes which are anti-VEGF naïve, please confirm the drug you are applying for: Aflibercept Please note: Aflibercept is the preferred choice of treatment in anti VEGF naïve patients as treatment requires less frequent follow-up visits. 9. Has this patient previously been treated with ranibizumab in the eye for which application received? If yes, please complete question 10 below Yes No Please complete questions 9 & 10 below Ranibizumab No 10. The following relates to the eye for which treatment is requested: When did the patient receive their first ranibizumab injection? Date: How many injections has the patient received within the last 12 consecutive assessments? Please provide the dates of the last 3 injections: Date , Date , Date If less than 7 injections in the last 12 consecutive assessments please give the reason for the switch: Clinician’s Declaration I confirm that I have discussed with the patient and that they understand and consent to their personal information being shared with commissioning and commissioning support organisations. I have also recorded this discussion in the patient’s notes. I confirm the risks and benefits of treatment have been fully discussed with the patient and documented. I confirm that funding approval is subject to initiation and follow up of treatment response being undertaken by a specialist ophthalmology team. I acknowledge and adhere to the criteria and cost effective use of this treatment as advocated in NICE TAs 155 & 294 and believe that within this Trust the above patient would be best managed using the treatment as requested above. If this patient is being jointly managed by a second consultant, please state name here: Name of supervising consultant: Date: Signature: Name: Date: Signature (or email confirmation) by Trust Chief Pharmacist (or deputy) Name: Signature: Date: Pharmacy and Medicines Optimisation Team Herts Valleys Clinical Commissioning Group (HVCCG) 2 National Institute of Clinical Excellence Ranibizumab for age-related macular degeneration: TA 155: Updated June 2012 Aflibercept for age-related macular degeneration: TA 294: July 2013 Treatment is commissioned for: 1. Patients who have not previously been treated with an Anti-VEGF injection (Anti-VEGF naïve patients) – aflibercept (preferred choice as requires fewer follow ups) and ranibizumab. 2. Patients on ranibizumab who have benefitted but require frequent injections - by local agreement, the use of aflibercept 2nd line in a sub-group of ARMD patients who have already been ‘heavy users’ of ranibizumab for a number of years. This group is defined as patients who have required more than 7 injections from the previous 12 assessments which should be in the last 12-16 months, with the last 3 injections at 4-6 week intervals. Fully informed consent should be given by the patient to change the treatment. An audit of outcomes of these patients will be requested. 3. If treating both eyes at the same time, the same treatment should be used. What is not commissioned: Aflibercept is not commissioned for non-responders to ranibizumab. The reason for this is that the effectiveness of aflibercept in this patient group is not known. Ranibizumab is not commissioned for patients who require frequent injections of aflibercept or who have not responded to aflibercept. These treatments are commissioned in line with the criteria outlined below: Commissioning criteria: Ranibizumab and aflibercept, within their marketing authorisation, are recommended as options for the treatment of wet age-related macular degeneration if all of the following circumstances apply in the eye to be treated: the best-corrected visual acuity is between 6/12 and 6/96 there is NO permanent structural damage to the fovea the lesion size is less than or equal to 12 disc areas in greatest linear dimension there is evidence of recent presumed disease progression (blood vessel growth, as indicated by fluorescein angiography, or recent visual acuity changes) the manufacturer provides the drug for injection with the discount agreed in the patient access scheme (PAS). Pharmacy and Medicines Optimisation Team Herts Valleys Clinical Commissioning Group (HVCCG) 3 In line with the NICE, the RCOphth has developed national guidelines for continuation and cessation of ranibizumab. Commissioners within Hertfordshire will commission in line with these national guidelines. Discontinuation criteria To be in line with Guidelines for Ranibizumab produced by the Royal College of ophthalmologists on http://www.rcophth.ac.uk/page.asp?section=451§ionTitle=Clinical+Guidelines From summary of Product Characteristics (SPC): RANIBIZUMAB (Lucentis®) The recommended dose for Lucentis is 0.5 mg given monthly as a single intravitreal injection. Treatment is given monthly and continued until maximum visual acuity is achieved i.e. the patient`s visual acuity is stable for three consecutive monthly assessments performed while on ranibizumab treatment. Thereafter patients should be monitored monthly for visual acuity. Treatment is resumed when monitoring indicates loss of visual acuity due to wet AMD. Monthly injections should then be administered until stable visual acuity is reached again for three consecutive monthly assessments (implying a minimum of two injections). The interval between two doses should not be shorter than one month. AFLIBERCEPT (Eylea®) The recommended dose for Eylea is 2 mg aflibercept. Eylea treatment is initiated with one injection per month for three consecutive doses, followed by one injection every two months. There is no requirement for monitoring between injections. After the first 12 months of treatment with Eylea, the treatment interval may be extended based on visual and anatomic outcomes. In this case the schedule for monitoring should be determined by the treating physician and may be more frequent than the schedule of injections. Pharmacy and Medicines Optimisation Team Herts Valleys Clinical Commissioning Group (HVCCG) 4