Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
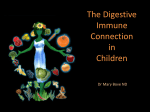
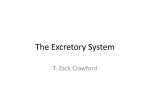
Renal Nutrition Forum A Peer Reviewed Publication of the Renal Dietitians Dietetic Practice Group Volume 33 • Number 1 In This Issue 1 Feature Article 2 Letter from the Editor 8 Advances in Practice 12 MNT Update 15 Transplant Update 20 Awards and Scholarships 21 App Review 22 Website Extras 24 Recently Published 25 Calendar of Events 26 RPG Chair Message 27 RPG Executive Committee www.renalnutrition.org The Relationship Between Gut Microbiota and CKD: Why Use Prebiotics in CKD Patients? Lindsey Zirker, RD, CSR, LD Consultant Dietitian Idaho Kidney Center Idaho Falls, ID Email: [email protected] This article has been approved for 1.0 CPE unit. The online CPEU quiz and certificate of completion can be accessed in the Members Only section of the RPG website via the My CPEU link. This CPE offering is available to current RPG members only and the expiration date is January 15, 2015. Abstract Intestinal integrity and gut microbiota play a significant role in immunity and in digestion of carbohydrates and protein. Chronic kidney disease (CKD) progression and current treatment modalities disrupt normal intestinal microbiota, cause increased production of organic solutes, and are associated with bacterial translocation and inflammation. These may play a role in the poor outcomes currently observed in CKD. As dietitians better understand this important relationship, therapeutic recommendations such as pro- and prebiotics may help to restore balance to the gut and improve outcomes for those with CKD. Introduction Dialysis patients present an interesting challenge for renal dietitians. Each patient is unique and requires specific nutritional recommendations to provide optimal care. Despite the differences however, one challenge ties them all together: improving albumin levels. It is known that multiple variables contribute to low albumin: inflammation, (CKD, diabetes or other chronic disease, infection, recent surgeries, inadequate dialysis and the hemodialysis process itself are pro-inflammatory), low protein intake or assimilation, protein wasted during peritoneal and hemodialysis, acidosis, and blood loss. Although dietitians educate, order supplements, provide meal plans, and re-educate, nutritional status may remain compromised. Perhaps it is because for many patients there is a major source of inflammation that is largely overlooked: the gut. It is widely known and accepted that the gut is a source of uremic toxins, which contribute to increased inflammation and cardiovascular disease- two major reasons for high mortality rates among CKD patients (1,2). Yet, most of the research and treatment for CKD focuses on managing other symptoms and does not consider the effect these symptoms and treatments have on the microbiota, the microbes present in the intestine. Outcomes for CKD may be improved by examining the relationship between CKD and microbiota in the gut, and then implementing therapy to restore the symbiotic relationship. The Symbiotic Relationship The intestine is home to billions of microbes, with 400 to 500 different types of bacteria that account for 40 to 60% of the contents of the intestine. There is a symbiotic relationship between the body and the bacteria in the gut (3). Intestinal microbiota play a role in immunity, digestion of carbohydrates – Continued on page 3. Renal Nutrition Forum 2014 • Vol. 33 • No. 1 1 Feature Article... and protein, and micronutrient homeostasis by metabolism of carbohydrates and amino acids (4). Intestinal Role in Immunity About 80% of the body’s immune system is connected to the intestines (5). This indicates that numerous mechanisms, such as the protective effects of probiotics and the intestinal wall barrier help or harm the immune system. Beneficial bacteria help to prevent bacterial translocation, when bacteria cross the intestinal barrier and gain entry to the blood stream. They compete with pathogenic microbes for growth and keep them in small enough numbers to be harmless. However, pathogenic microbiota may cause illness, inflammation and strain on the immune system if they are left unchecked (6). In addition to beneficial bacteria in the intestine, the body has a mechanical barrier- a thin epithelial layer that prevents bacteria translocation. This barrier’s protective effect is accomplished in part by a mucus layer and antimicrobial proteins. The proteins act as a type of armor to prevent actual contact between the epithelial layer and the microbiota (7). The highly controlled transport systems within the intestinal wall also play a protective role (4,8). Microbiota in Carbohydrate and Protein Metabolism Anaerobic bacteria in the gut help the body to further digest carbohydrates and protein through a process called fermentation. Saccharolytic bacteria ferment carbohydrates and produce hydrogen, methane, and short-chain fatty acids such as butyrate, propionate, and acetate. These end-products are beneficial to the individual. For example, butyrate is a source of energy for the epithelium in the colon (1,3). Proteolytic bacteria metabolize protein in the gut when proteases and peptidases hydrolyze polypeptide chains to create small peptides and amino acids. The proteolytic bacteria in the colon ferment the amino acids. This process creates end-products, like short and branched chained fatty acids as well as ammonia, phenols, indoles, and amines. Some of these end-products are toxic, necessitating removal from the body via the intestines or the kidney (1,3). Pathology of Dysbiosis in CKD It is common that those with chronic disease have abnormal microbiota when compared to healthy individuals (1). Diet and impaired protein absorption, increased intestinal transit time, medications, and uremia may all contribute to unfavorable changes in microbiota. Renal Nutrition Forum 2014 • Vol. 33 • No. 1 www.renalnutrition.org Renal Diet and Protein Absorption Dietitians are well acquainted with the limitations of the renal diet. Potassium restriction often limits fruit, vegetable and whole grain intake, which in turn reduces dietary fiber present in the intestine and may play a role in altering microbiota (3,4). Protein malnutrition is common and associated with increased morbidity and mortality among CKD patients. In an observational study that evaluated protein assimilation, it was found that those with CKD had impaired assimilation compared to those without CKD (9). The high protein diet, if on dialysis, and impaired protein digestion and absorption increases protein availability in the gut. This favors proteolytic bacterial activity and increases uremic organic solute production (1). Malnutrition also reduces intestinal cell replication which may lead to breakdown of the intestinal wall and promote bacterial translocation (8). Increased Transit Time Constipation is common among dialysis patients. Constipation is reported for more than half of patients on hemodialysis, 63%, and about 29% of patients on peritoneal dialysis, compared to only 10 to 20% of healthy individuals (3). This is likely related to decreased fiber and fluid intake, but may also be related to a more sedentary lifestyle, use of phosphate binders, and primary disease states such as diabetes which can lead to gastroparesis. Increased transit time leads to increased amounts of proteolytic bacteria traveling upstream in the intestines, decreasing saccharolytic bacteria activity as well as increasing time for bacteria metabolism and intestinal absorption of organic solutes (3). Medications Antibiotic use is common among those with CKD. In 2007, 41% of dialysis patients were prescribed an antibiotic (10). Unfortunately, probiotics are easily killed by antibiotics, while more pathogenic strains seem to become resistant. Often, pathogenic bacteria that are left to grow freely will remain at higher than normal levels even though the competing bacteria are once again present. Although the individual may be reintroduced to the bacteria that were destroyed, the levels will not return to normal (6). Uremia Uremia is a multifaceted aspect of CKD. Although the exact mechanisms are unclear at this time, it seems that organic solutes contribute to the breakdown of the intestinal wall barrier and bacterial translocation (7). 3 Feature Article... Organic solutes provide significant insight into the glomerular filtration rate (GFR). As GFR declines, organic solutes in the blood will rise, namely creatinine and urea (11). When this occurs, passive diffusion and other glandular secretions transport urea into the intestine in an effort to reduce the levels in the blood stream. Bacteria in the intestine hydrolyze urea via urease and form ammonia. This leads to an acidic (decreased) intestinal pH and inflammation in the intestine known as uremic enterocolitis (4). Protein-bound Uremic Solutes Organic solutes are typically classified by their molecular weight (MW) and ability to bind to protein. There are three basic categories: small MW and water soluble compounds, protein bound compounds, and larger MW compounds or “middle molecules” (12). Dialysis (peritoneal and hemodialysis) is able to filter out many of these organic compounds, but appears to be particularly ineffective at removing protein-bound organic solutes. Two organic solutes in particular are p-cresyl sulfate (PCS) and indoxyl sulfate (IS). PCS is metabolized by anaerobic bacteria in the gut. Tyrosine and phenylalanine are metabolized to 4-hydroxyphenylacetic acid and then decarboxylated to p-cresyl, which is then metabolized to PCS by cystolic sulfotransferase (12). IS is also produced by bacterial metabolism in the gut. Protein that has been broken down to tryptophan is metabolized in the intestine by bacteria to indole. It is then absorbed and transported to the liver where it is converted to IS (12). Many studies have shown that these two protein-bound organic solutes contribute significantly to renal and vascular toxicity (12). In the kidney, IS increases expression of inflammatory markers such as transforming growth factor beta 1 (TGF 1) and decreases superoxide scavenging activity. This leaves the kidney vulnerable to free radical activity and speeds the progression of kidney failure and complications (13). Inflammation and free radical activity are not limited to the kidney. IS and PCS may also contribute to cardiovascular disease (CVD). In the case with IS, endothelial cell repair is reduced by production of oxidative stress and promotes atherosclerosis. IS levels have also been positively correlated with aortic calcification and vascular stiffness (12). These factors significantly contribute to poor cardiovascular health. In addition, Mejiers et al showed a positive correlation between PCS and increased cardiovascular events independent of GFR and other studies have shown a strong relationship between PCS levels and CVD (12,14). 4 Probiotic and Prebiotic Therapy Clearly, there is a an opportunity to support intestinal health and improve outcomes for CKD patients. One of the major therapies being investigated is supplementation of probiotics. The World Health Organization defines probiotics as “live microorganisms, which, when administered in adequate amounts, confer a health benefit on the host” (15). Probiotics can be found in dietary supplements, fermented dairy foods, as well as in fermented soy and vegetable products and some juices. When ingested, the probiotics enter into the intestine and begin to replenish the friendly bacterial environment. The current body of evidence support probiotics uses independent of CKD for constipation; diarrhea (travelers, antibiotic associated and infectious); vaginal, respiratory, stomach and skin infections; periodontal disease; inflammatory bowel disease and irritable bowel disease (15). Prebiotics are defined as “a nondigestible food ingredients that beneficially affect the host by selectively stimulating the growth and/ or activity of one or a limited number of bacteria in the colon, and thus improve host health” (16). There are several substances that may leave the small intestine undigested, but only certain ones are also able to promote saccharolytic bacterial growth: inulin, oligofructose, galactos-oligosaccharides, high molecular weight inulin, and fructooligosaccharides (FOS) (16). Probiotic and Prebiotic Therapy in CKD Probiotics and prebiotics present several possibilities for improving outcomes in CKD patients. Based on current knowledge, probiotic supplementation may alter the microbiota in the gut and will likely increase saccharolytic activity and promote increased amounts of beneficial by-products for the host. Increased saccharolytic activity may also decrease proteolytic activity, thus decreasing production of protein-bound uremic solutes and intestinal inflammation (2,3). Decreased inflammation may result in a healthier intestinal wall which will help to prevent bacterial translocation and interruption of the intestinal transport systems (4,7,8). Prebiotics work symbiotically with the probiotics to benefit the host. In addition to providing fuel for saccharolytic bacteria, prebiotics may also increase transit time (alleviate constipation), increase fecal weight (improve diarrhea) with fewer side effects and increase quality of life among patients (16). The increased transit time will also provide a friendly environment for saccharolytic bacteria thus decreasing proteolytic bacteria production of PCS and IS (3). Research on Probiotics in CKD Patients The current body of research has established that the process of CKD alters gut microbiota. More specifically, there are increased levels of Renal Nutrition Forum 2014 • Vol. 33 • No. 1 www.renalnutrition.org Feature Article... PCS and IS from proteolytic bacteria activity, and this contributes to the poor outcomes due to the impact on the cardiovascular system (1,3,4,12,17). Use of probiotics to decrease IS and PCS is not well established. To date, only one study has shown a significant decrease in IS and PCS with treatment using prebiotics in hemodialysis patients (19). Studies using probiotics in CKD populations have shown promising results. A double-blind, placebo, crossover study in CKD patients found that blood urea nitrogen (BUN) levels were significantly lower with probiotic therapy, although creatinine differences were insignificant (20). Another randomized, doubleblind placebo, crossover trial investigated the benefit of using probiotics. Results indicated that BUN and creatinine levels decreased, although not significantly. However, the quality of life assessment reflected an 86% overall improvement (p<0.05) (5). Rossi et al conducted a meta-analysis of studies evaluating use of probiotics and prebiotics in reducing PCS and IS (19). They concluded that there seems to be a beneficial effect of using probiotics and prebiotics to reduce PCS and IS in hemodialysis and healthy populations despite small sample size. The review of Table 1. Health Benefits of Probiotic Strains (6,22) Species and Strain General GI Health Health B. animalis DN-173 010, (1) B. infantis 35624 B. lactis Bb-12 B. lactis HN019, DR10 (2) L. acidophilus NCFM (2) L. casei DN-114 001, (3) L casei Shirota L. fermentum RC-14 L. plantarum 299v L. reuteri SD2112, ING1, MM53, ATCC 55730 (4) L. rhamnosus GG, LGG, (5) L. rhamnosus GR-1 Viral Diarrhea x x x x x x x x x x x x x x x x x * x x x x x studies shows a high tolerance of probiotic therapy with only 15% reporting intolerance to the therapy. Recommendations for Therapy More research is needed to support the hypothesis that probiotics can improve outcomes by decreasing IS and PCS. However, there is sufficient evidence supporting the use of probiotics in CKD patients due to antibiotic associated diarrhea, C. difficile and other maladies probiotics have shown to alleviate (6). While foods are a preferable source for most nutrients, many probiotic foods are also high in potassium and phosphorus which must be limited in a renal diet. Because of this, supplements are likely to show the most therapeutic benefit for those with CKD, although inclusion of some probiotic foods may be beneficial as recommended. Probiotic Recommendations It is impossible to recommend a blanket dose and strain for all CKD patients due to the unique make up and multitude of factors influencing microbiota in the gut. However, based on available research, some general recommendations are appropriate. Table 1 is a summary of probiotic strains and their potential health benefits. Antibiotic Assoc. Diarrhea C. Difficile Urinary Cold & Diarrhea Tract Resp Infection Virus x x x x x x x Product including species Activia Align Yo-Plus Danisco DanActive Yakult x GoodBelly x * x x Culturelle Femdophilus L. rhamnosus HN001, DR200 (2) x x S. boulardii lyo x x * * * Florastor x: strain shows positive response in human and animal studies *: recommended by 2005 Yale Note: This table shows the species that have been used in studies, not the products. The product University Workshop simply contains the species studied. Renal Nutrition Forum 2014 • Vol. 33 • No. 1 www.renalnutrition.org 5 Feature Article... Probiotic Safety There are some who question the safety of providing bacteria to immune-compromised individuals. Of the few studies that have been conducted, a minimal number of negative events have been reported (17,23). Probiotic strains are not pathogenic and probiotic-related infections are rare occurrences. Nevertheless, as with all supplements and medications, a healthcare provider should take the individual’s case into consideration before recommending probiotics and continue to monitor the individual (23). A patient’s dietary restrictions and serum levels of potassium and phosphorus should also be taken into consideration. While the studies reviewed for this article did not report altered potassium and phosphorus levels, food products and supplements should be investigated to determine if they fit within the patient’s diet parameters. In choosing a probiotic supplement, several considerations should be taken into account such as strain and dose. Below are listed a few resources available to guide healthcare providers. • Natural Medicine Comprehensive Database: for evaluation of specific products • References from this article (2,6,17,19,22) • Manufacturer’s Website: in the section for professionals, many will have studies listed In recommending an amount, dose will vary by strain and the overall health of the individual, however many studies use doses from 1 to 10 billion CFUs and see beneficial results (19). Prebiotics will also facilitate bacterial growth (24). Table 2. Partial List of Commercial Food Products Containing Prebiotics that are Available to Consumers. Reprinted from Journal of the American Dietetic Association, 108(3), Douglas LC, Sanders ME, “Probiotics and prebiotics in dietetics practice”, Pages 510-21, Copyright 2008, with permission from Elsevier (22). 6 Renal Nutrition Forum 2014 • Vol. 33 • No. 1 www.renalnutrition.org Feature Article... Prebiotic Recommendations To date no specific recommendations for prebiotics have been made for CKD patients. However, health benefits are seen with an intake of 3 g of short-chain FOS up to 8 g for mixed short and long-chain inulin. In the case of resistant starches, 20 g per day is recommended although lower doses have shown benefits (22). Table 2 shows common products containing various types of prebiotics as well as health claims. Conclusion CKD outcomes may be improved by addressing CKD-induced dysbiosis with pre- and probiotic supplementation. More research will help to further explain the exact processes and appropriate probiotic therapy. In the meantime, evidenced-based use of prebiotics and probiotics may prove helpful in restoring normal gut microbiota and improving patient quality of life. References 1. Poesen R, Meijers B, Evenepoel P. The colon: an overlooked site for therapeutics in dialysis patients. Semin Dial. 2013;26(3):32332. 2. Vitetta L, Gobe G. Uremia and chronic kidney disease: the role of the gut microflora and therapies with pro- and prebiotics. Mol Nutr Food Res. 2013;57(5):824-32. 3. Evenepoel P, Meijers BK, Bammens BR, Verbeke K. Uremic toxins originating from colonic microbial metabolism. Kidney Int Suppl. 2009;(114):S12-9. 4. Vaziri ND, Wong J, Pahl M, et al. Chronic kidney disease alters intestinal microbial flora. Kidney Int. 2013;83(2):308-15. 5. Ranganathan N, Ranganathan P, Friedman EA, et al. Pilot study of probiotic dietary supplementation for promoting healthy kidney function in patients with chronic kidney disease. Adv Ther. 2010;27(9):634-47. 6. Huffnagle GB, Wernick S. The Probiotics Revolution: The Definitive Guide to Safe, Natural Health Solutions Using Probiotic and Prebiotic Foods and Supplements. Bantam; 2008. 7. Anders HJ, Andersen K, Stecher B. The intestinal microbiota, a leaky gut, and abnormal immunity in kidney disease. Kidney Int. 2013;83(6):1010-6. 8. Kotanko P, Carter M, Levin NW. Intestinal bacterial microflora: A potential source of chronic inflammation in patients with chronic kidney disease. Nephrol Dial Transplant. 2006;21(8):2057-60. Renal Nutrition Forum 2014 • Vol. 33 • No. 1 www.renalnutrition.org 9. Bammens B, Verbeke K, Vanrenterghem Y, Evenpoel P. Evidence for impaired assimilation of protein in chronic renal failure. Kidney Int. 2003;64(6):2196. 10. USRDS info. Available at: http://www.usrds.org/2009/ pres/06U_asn09_antibiotic_use. Accessed June 7, 2013. 11. Rennke HG, Denker BM. Renal Pathophysiology: The Essentials. Baltimore, MD: Lippincott Williams & Wilkins, 2007. 12. Liabeuf S, Drüeke TB, Massy ZA. Protein-bound uremic toxins: new insight from clinical studies. Toxins (Basel). 2011;3(7):911-9. 13. Mitsubishi Tanabe Pharma. (n.d.). The role of uremic toxins in chronic kidney disease progression [Pamphlet]. 14. Meijers BK, Claes K, Bammens B, et al. p-Cresol and cardiovascular risk in mild-to-moderate kidney disease. Clin J Am Soc Nephrol. 2010;5(7):1182-9. 15. NCCAM. An introduction to probiotics. Available at: http://nccam.nih.gov/health/probiotics. Accessed June 7, 2013. 16. Roberfroid D, Gibson M, Hoyles G. Prebiotic Effects: metabolic and health benefits. Br J Nutr. 2010; 104:S1-63. 17. Chow J. Probiotics and prebiotics: A brief overview. J Ren Nutr. 2002;12(2):76-86. 18. Meijers BK, Evenepoel P. The gut-kidney axis: indoxyl sulfate, p-cresyl sulfate and CKD progression. Nephrol Dial Transplant. 2011;26(3):759-61. 19. Rossi M, Klein K, Johnson DW, Campbell KL. Pre-, pro, and synbiotics: do they have a role in reducing uremic toxins? A systematic review and meta-analysis. Int J Nephrol. 2012;2012:673-631. 20. Ranganathan N, Friedman EA, Tam P, Rao V, Ranganathan P, Dheer R. Probiotic dietary supplementation in patients with stage 3 and 4 chronic kidney disease: A 6-month pilot scale trial in Canada. Curr Med Res Opin. 2009;25(8):1919-30. 21. Ranganathan N, Patel B, Ranganathan P, et al. Probiotic amelioration of azotemia in 5/6th nephrectomized SpragueDawley rats. Scientific World Journal. 2005;5:652-60. 22. Douglas LC, Sanders ME. Probiotics and prebiotics in dietetics practice. J Am Diet Assoc. 2008;108(3):510-21. 23. Sanders ME, Akkermans LM, Haller D, et al. Safety assessment of probiotics for human use. Gut Microbes. 2010;1(3):164-85. 24. Kopp-Hoolihan L. Prophylactic and Therapeutic Uses of Probiotics. J Am Diet Assoc. 2001;101(2):229-41. 7