Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
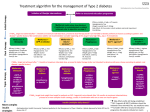
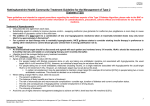
Keele’s ‘Important News and Evidence’ Service KINES Rapid Update January 2016 Updated NICE guidance on Type-2 Diabetes – recommendations on drug treatments The long-awaited update of NICE Guideline on Type-2 Diabetes (NG28) was published in December 2015. This guideline had been subject to a second round of consultation following concerns raised about the first draft published in January 2015. Some important changes have now been made in the final guideline to address these concerns. Key to these changes, and to implementing the new guidance, is the emphasis on working with patients to personalise care. Treatment should be tailored to their needs and circumstances, taking into account personal preferences, comorbidities, risks from polypharmacy, and ability to benefit from long-term interventions where there is reduced life expectancy. Such an approach is especially important in the context of multi-morbidity. This has particular relevance in helping patients decide on management of blood glucose control, a topic covered in a new Patient Decision Aid developed by NICE. Below we consider the guideline’s recommendations on drug treatments, including blood pressure management and lipid modification, as well as blood glucose lowering therapies. Regarding future iterations of this guideline, NICE has indicated there are plans in place to establish a Standing Update Committee on diabetes. This may enable more rapid updating of this guidance, to better keep pace with developments in this rapidly evolving clinical area. Key documents/resources: Type 2 diabetes in adults (NG28). December 2015. www.nice.org.uk/guidance/ng28 Algorithm for blood glucose lowering therapy in adults with type 2 diabetes. NICE. December 2015 http://www.nice.org.uk/guidance/ng28/resources/algorithm-for-blood-glucose-lowering-therapy-in-adults-with-type-2-diabetes2185604173. Patient decision aid: first intensification of blood glucose therapy. NICE. December 2015. http://www.nice.org.uk/guidance/ng28/resources/patient-decision-aid-2187281197 What are the key drug recommendations for managing cardiovascular (CV) risk in adults with type 2 diabetes? Blood pressure management: Recommendations in the new guideline (NG28) largely follow those in previous guidance published in 2009. It sets thresholds for medication use if lifestyle advice does not reduce blood pressure to below 140/80 mmHg (or below 130/80 mmHg if there is kidney, eye or cerebrovascular damage). As previously, the mainstay of first-line antihypertensive drug treatment is an angiotensin converting enzyme (ACE) inhibitor, with addition of a calcium channel blocker, or a thiazide or thiazide-related diuretic. (See NG28 for full recommendations). This differs somewhat with the NICE 2011 hypertension guideline (CG127) for people without type 2 diabetes, which favours thiazide-like diuretics (e.g. indapamide), in preference to conventional thiazide diuretics, such as bendroflumethiazide or hydrochlorothiazide. Antiplatelet therapy for primary prevention: NG28 advises not to offer antiplatelet therapy (aspirin or clopidogrel) for adults with type 2 diabetes without cardiovascular disease (CVD). This change in guidance follows evidence that has emerged in recent years that the risks of adverse events, such as bleeding, exceed the benefits in this population. Lipid modification with statins: Lipid modification is an important intervention in type 2 diabetes. As recommended in section 1.5 (antiplatelet therapy) of NG28, people with type 2 diabetes should be managed according to the 2014 Clinical Guideline on Lipid Modification (CG181): o QRISK2 should be used to estimate risk in those who do not have established CVD and people offered atorvastatin 20 mg daily with >10% 10-year risk of CVD. o For type 2 diabetes, it advises considering increasing the dose up to 80 mg atorvastatin daily, if a 40% reduction in non HDL-cholesterol is not achieved. o For secondary prevention, all should be given atorvastatin 80 mg daily. o Fibrates are no longer recommended. What are the key drug recommendations on managing blood glucose in adults with type 2 diabetes? Summary of targets for HbA1c in NG28: For adults with type 2 diabetes managed either by lifestyle and diet, or by lifestyle and diet combined with a single drug not associated with hypoglycaemia, support the person to aim for an HbA 1c level of 48 mmol/mol (6.5%). For adults on a drug associated with hypoglycaemia (for example, a sulfonylurea), support the person to aim for an HbA1c level of 53 mmol/mol (7.0%). In adults with type 2 diabetes, if HbA1c levels are not adequately controlled by a single drug and rise to 58 mmol/mol (7.5%) or higher: o reinforce advice about diet, lifestyle and adherence to drug treatment, and o support the person to aim for an HbA1c level of 53 mmol/mol (7.0%), and o intensify drug treatment. Consider relaxing the target HbA1c level on a case-by-case basis, with particular consideration for people with type 2 diabetes who are older or frail: o who are unlikely to achieve longer-term risk-reduction benefits, for example, people with a reduced life expectancy o for whom tight blood glucose control poses a high risk of the consequences of hypoglycaemia, for example, people who are at risk of falling, people who have impaired awareness of hypoglycaemia, and people who drive or operate machinery as part of their job o for whom intensive management would not be appropriate, for example, people with significant comorbidities. The above ‘personalisation’ or ‘relaxation’ of HbA1c levels appear to address concerns raised during consultation that these targets do not have a strong evidence base, and that uncritical adherence may cause harm, particularly with regard to the risks of hypoglycaemia. These risks have been seen in some randomised controlled trials (RCTs), such as ACCORD, and observed in some large database studies, e.g. Currie at al., 2010. It is important that these ‘relaxations’ are carefully explored when considering intensification of treatment. Drug treatments to reduce blood glucose: Blood glucose lowering therapy recommendations are summarised in the guideline’s algorithm, reproduced at the end of this document. Some important considerations follow: The use of sodium glucose co-transporter 2 (SGLT2) inhibitors is not described in the guideline or the algorithm. o Instead NG28 advises that NICE guidance on canagliflozin in combination therapy for treating type 2 diabetes (TA315), dapagliflozin in combination therapy for treating type 2 diabetes (TA288) and empagliflozin in combination therapy for treating type 2 diabetes (TA366), should be referred to. o In some respects these omissions could cause confusion. Because of the rapidly emerging evidence for these drugs (for example, the EMPA-REG OUTCOME study), this may be the type of issue that lends itself to rapid revision by a NICE Standing Update Committee for diabetes. Metformin remains a key role as the first-line drug treatment. (Note - the need to monitor renal function and modify treatment, if necessary.) If metformin is contraindicated or not tolerated, consider initial drug treatment with: a dipeptidyl peptidase-4 (DPP-4) inhibitor, or pioglitazone, or a sulfonylurea (SU). A preference for one of these is not stated. This now means that an SU is no longer the main second-line therapy. If metformin has not continued to control HbA1c to below the individually agreed threshold for intensification, consider dual therapy with: metformin and a DPP-4 inhibitor or, metformin and pioglitazone (taking into account risks of adverse events specific to pioglitazone, such as heart failure), or metformin and an SU. Although repaglinide had a prominent place in the draft guidelines, this has not carried over into the final guideline. Three recently published, large RCTs have looked at whether DDP-4 inhibitors have an effect on CV outcomes in type 2 diabetes (SAVOR-TIMI 53, TECOS and EXAMINE). In these studies, DPP-4 inhibitors did not reduce CV events. (Further information on the TECOS study is available in the July 2015 KINES Rapid Update, available via our website http://centreformedicinesoptimisation.co.uk/.) NG28 gives guidance on triple oral therapy (see the algorithm) in those who can take metformin. NG28 also looks at when to consider introducing injectable glucagon-like peptide 1 (GLP-1) mimetic drugs (exenatide, liraglutide, lixisenatide and dulaglutide). These are associated with weight loss. o It advises to consider using these in severely obese people (generally BMI 35 kg/m 2 or higher) with associated physical or psychological problems if triple therapy is not effective, not tolerated or contraindicated (see algorithm). o They should be used in combination therapy with metformin and an SU. o They can also be considered for people with less severe obesity where weight loss is particularly beneficial or where insulin might cause occupational problems (driving or operating machinery). It advises to stop the GLP-1 mimetic if the person has not had a beneficial metabolic response (a reduction of at least 11 mmol/mol [1.0%] in HbA1c and a weight loss of at least 3% of initial body weight in 6 months). These ‘starting and stopping rules’ remain important as audit criteria. The advice for triple oral therapy and the GLP-1 mimetic drugs only applies in the guideline if the person is taking metformin; in those who cannot take metformin or who are intolerant, the next step after dual therapy (e.g. an SU and DDP-4, or pioglitazone and an SU, or pioglitazone and DDP-4) would be to consider insulin therapy. Another important recommendation is only to offer a GLP-1 mimetic in combination with insulin with specialist care advice and ongoing support from a consultant-led multidisciplinary team. There has been enthusiasm to combine a GLP-1 mimetic with insulin, as this use may offset the weight gain seen with insulin. Guidance on use of insulin is similar to that in the previous guideline, with the mainstay of basal insulin treatment being NPH insulin for most people (see algorithm). When this is started, metformin should be continued in those people able to take it. The guideline advises not to routinely offer self-monitoring of blood glucose (SMBG) levels, unless the person is on insulin or has had episodes of hypoglycaemia, or the person is on oral medication that may increase their risk of hypoglycaemia while driving or operating machinery. SMBG should also be offered if the person is pregnant, or is planning to become pregnant (see NICE 2015 guideline [NG3] on diabetes in pregnancy). KINES is produced by The Centre for Medicines Optimisation at Keele University for subscriber CCGs. The views expressed are Keele’s and may not reflect local prescribing guidance. External hyperlinks are provided as a convenience but are out of Keele’s control and do not constitute an endorsement by Keele.