Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
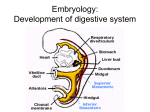
Oral peripheral examination for cleft palate/velopharyngeal dysfunction Cecyle Carson, Ph.D. & Alejandro Brice, Ph.D. University of Central Florida University of South Florida, St. Petersburg Abstract: An oral peripheral examination protocol will be presented specifically for those who have cleft lip and/or palate or velopharyngeal dysfunction (VPD). The protocol differs from common oral peripheral exams in that it has the clinician observe specific structural dysmorphologies and other issues associated with overt and submucous clefts. Examples include detailed observation of the velum and posterior pharyngeal wall, as well as questions regarding nasal regurgitation and upcoming dental/orthodontic plans. Summary: Clefts of the lip and/or palate occur in approximately 1 in 750 newborns, making this deformity the fourth most common birth defect, and first most common facial birth defect. Children born with clefts of the palate are susceptible to specific types of speech and resonance problems associated with overt or covert clefts and/or VPD, including hypernasality, nasal emission on or weak production of pressure consonants, compensatory articulation errors, and articulation errors related to dental, occlusal, or VPD issues; thus, specialized evaluation tasks are required. Standardized oral mechanism examinations do not account for the special structural and functional problems associated with those who have overt or covert (i.e., submucous or occult) clefts. Suggestions on assessing the oral mechanism in this population are available via articles (e.g., Dworkin, Marunik, & Krouse, 2004; Kummer & Lee, 1996) or books (e.g., Peterson-Falzone, Trost-Caramone, Karnell, & HardinJones, 2006). An oral examination protocol is needed that is specific for this population, especially since a primary purpose of the exam is to provide an initial impression of velopharyngeal functioning. The oral peripheral exam protocol developed by the authors follows. Oral Peripheral Examination Protocol ORAL STRUCTURES 1. LIPS Unremarkable Short Upper Lip Tight Upper Lip Unremarkable Missing Anterior malalignment Lateral malalignment Ectopic Diastema Comments: 2. TEETH Comments: 3. OCCLUSION Unremarkable Open bite Overbite/closed bite Collapsed alveolar arch(es) Anterior Cross Bite/Underbite 3a. Class of occlusion Class I Class II Class III Comments: 4. Hard PALATE Unremarkable High Arch Prominent Ridges Comments: Prolong “ah” loudly. Then say “ah” “ah” “ah” “ah” or “ha” “ha” “ha” 5. Soft PALATE/VELUM Unremarkable Short Asymmetric Elevation Limited Elevation Blue Line midline1 Notch/V-shape at posterior portion of hard palate1 Comments: 6. UVULA Bifid1 Unremarkable Absent/hypoplastic Comments: 7. POST PHARYNGEAL WALL Unremarkable No or Minimal Lateral Wall Movement Appears Too Deep Enlarged Palatine Tonsils Passavant’s Ridge Comments: 8. FISTULA(s) Absent 8a. FISTULA(s) LOCATION Present Alveolar Ridge2 Hard Palate3 Is the fistula size >4.5 mm? [Must be larger than this to have effect on velar movement] Comments: Soft Palate Yes No 9. SECONDARY PROCEDURE None Pharyngeal Flap Sphincter Pharyngoplasty Other Comments: 10. ORTHODONTICS/PROSTHODONTICS None Expander Ortho Bands (braces) Obturator 10 a. What are orthodontic plans? 10b. If present, does prosthetic affect speech? Yes No Comments: 11. HEARING Otitus Media in past year? 1-3 bouts 4-6 PE tubes? Present None >6 Comments: 12. Present FEEDING ISSUES Yes No Yes No Comments: 13. NASAL REGURGITATION Comments: Notes: 1= signs of a submucous cleft; not all have to be present for a diagnosis of submucous cleft 2= sounds that could be affected by the fistula are anterior anterior pressure consonants /p,b,t,d,f,v,s,z/ 3 = sounds that could be affected by the fistula are posterior pressure consonants /k,g/ Note: Factors not visible that can affect VP closure are: enlarged tonsils, pharyngeal web, deficiency of muscle mass on nasal surface of velum (absent musculus uvulae), abnormal direction of pull of velar muscles, and inadequate movement of pharyngeal wall for closure. Dworkin, J.P., Marunick, M.T., & Krouse, J.H. (2004). Velopharyngeal dysfunction: Speech characteristic, variable etiologies, evaluation techniques, and differential treatment. Language, Speech, and Hearing Services in Schools, 35, 333-352. Kummer, A.W., & Lee, L. (1996). Evaluation and treatment of resonance disorders. Language, Speech, and Hearing Services in Schools, 27, 271-281. Peterson-Falzone, S.J., Trost-Cardamone, J.E., Karnell, M.P., & Hardin-Jones, M.A. (2006). The clinician’s guide to treating cleft palate speech. St. Louis, MO: Mosby.