Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cognitive Behavioral Therapy of
Depressive Disorders and Suicidality in
Children and Adolescents
Daniel Stein, M.D.
Pediatric Psychosomatic Department
The Edmond and Lily Safra Children’s Hospital
The Chaim Sheba Medical Center, Tel Hashomer
Affiliated with the Sackler Faculty of Medicine
Tel Aviv University, Tel Aviv
References
Beck JS: Cognitive Therapy: Basics and Beyond. New York: Guilford Press, 1995
Beck JS: Cognitive Therapy for Challenging Problems. New York: Guilford Press, 2005
Brent DA, Poling K: Cognitive Therapy Treatment Manual for Depressed and Suicidal
Youth. Pittsburgh, PA: Services for Teen at Risk (STAR) Publications, 1997
Brent DA: Assessment and treatment of the youthful suicidal patient.
Annals of the New York Academy of Science. 932:106-28; discussion 128-31, 2001
Sherrill JT, Kovacs M: Nonsomatic treatment of depression: Child and Adolescent
Psychiatric Clinics of North America 2002 11:579-93, 2002
Butler AC, Chapman JE, Forman EM, Beck AT: The Empirical Status of CognitiveBehavioral Therapy: A Review of Meta-Analyses. Clinical Psychology Review, 26:17-31,
2006
References
Vitiello B, Brent DA, Greenhill LL, Emslie G, Wells K, Walkup
JT, Stanley B, Bukstein O, Kennard BD, Compton S, Coffey B,
Cwik MF, Posner K, Wagner A, March JS, Riddle M, Goldstein T,
Curry J, Capasso L, Mayes T, Shen S, Gugga SS, Turner JB,
Barnett S, Zelazny J. Depressive symptoms and clinical status
during the Treatment of Adolescent Suicide Attempters (TASA)
Study. Journal of the American Academy of Child and Adolescent
Psychiatry 2009;48(10):997-1004.
Butler AC, Chapman JE, Forman EM, Beck AT. The empirical
status of cognitive-behavioral therapy: A review of meta-analyses.
Clinical Psychology Review 2009; 26 (1): 17-31.
References
• דאי-גבאי א ,מור נ .דכאון .מתוך :מור נ ,מאיירס י ,מרום צ ,גלבוע-
שכטמן א .טיפול קוגניטיבי התנהגותי בילדים .הוצאת דיונון ,תל אביב,
,2011ע' 167-190
• סטארק קד ,סטרייסנד ו ,ארורה פ ,פאטל פ .דיכאון בגיל הילדות .מתוך:
טיפול בילדים ובמתבגרים .עורך קנדל פס ,תרגום אבישי י' ,2012 ,ע' -
373302
• ספיריטו א ,אספוסיטו-סמיתרס כ ,ויסמור ג' ,מילר א .התנהגות אבדנית
אצל מתבגרים .מתוך :טיפול בילדים ובמתבגרים .עורך קנדל פס ,תרגום
אבישי י' ,2012 ,ע' 374-409
Lecture Plan
Cognitive Behavioral Therapy (CBT) – Basic Principles
Core Beliefs (Schemas)
Intermediate Beliefs
Automatic Thoughts
Principles of CBT
Structure of Therapeutic Session
Treatment of Suicidal Adolescents TASA-CBT
CBT in Children & Adolescents – Clinical Considerations
Advantages
Limitations
Lecture Plan
TASA-CBT-Key Characteristics & Primary Techniques
Safety Plan
Chain Analysis
Development of Adaptive Coping Skills
Cognitive Restructuring
Distress Tolerance
Problem Solving
Behavioral Family intervention
Relapse Prevention
Practical Considerations
Cognitive Behavioral Therapy (CBT) –
Basic Principles
Cognitive behavioral therapy (CBT) is defined in terms of the cognitive
model rather than the specific set of techniques employed
The CBT model emphasizes the importance of the individual’s perception of
the world - primacy of meaning of event
Psychopathological disorders are conceptualized in terms of persistent
disordered thinking, derived from embedded dysfunctional beliefs
Improvement results from evaluation and modification of dysfunctional
thinking
Evidence-based treatment
Principles of CBT in depression
• of non-depression related behaviors the
risk for the development of depression
• in dysfunctional depression-related
cognitions may also the risk for the
development of depression
Principles of CBT in depression
• These cognitions include:
• in competence; in helplessness
• in hope; in hopelessness
• in rumination of these negative cognitions
in the ability to distract from these cognitions
& in the ability to problem-solve
•
Core Beliefs (Schemas)
Core beliefs – early-onset, deep-seated (unconscious) & persisting
beliefs concerning oneself, significant others, & the
world around
Characteristics in psychopathology:
rigid, global, (always, never)
considered absolute truth )"("ככה
self-critical, negative ,
irrational
dysfunctional
Characteristic Core Beliefs
Lack of self-esteem (eating disorders, narcissistic disturbances, depression)
Beck’s cognitive triad in depression – negative perception of
oneself (helpless, unlovable, worthless)
the world around (inefficiency)
the future (hopelessness)
Insecurity, vulnerability, nothing is certain, catastrophic misinterpretation
of sensations (anxiety disorders)
HELPLESSNESS CORE BELIEFS
I am inadequate, ineffective, incompetent, can’t
cope.
I am powerless, out of control, trapped.
I am vulnerable, likely to be hurt, weak, needy, a
victim.
I am inferior, a failure, a loser, not good enough,
defective, don’t measure up.
UNLOVABLE CORE BELIEFS
I am unlovable, unwanted, will be rejected or
abandoned, will be always alone.
I am undesirable, unattractive, ugly, boring, have
nothing to offer.
I am different, defective, not good enough to be
loved by others.
WORTHLESSNESS CORE
BELIEFS
I am worthless, unacceptable, bad, crazy, broken,
nothing, a waste.
I am hurtful, dangerous, toxic, evil.
I don’t deserve to live.
Intermediate Beliefs in Depression
Core beliefs- worthlessness/helplessness/hopelessness
General beliefs – People feel this way because nothing they do is
good enough; as there is no way to change this condition, the best
thing is not do anything, just wait till things are over, till something
happens, although this will, likely, not be the case
Personal rules/personal expectations – I expect nothing from
myself or others; no one should expect anything from me
Intermediate Beliefs in Depression
Conditional assumptions – If I do nothing, or if no one
sees me, no one will criticize me. Self criticism will
prevent/ compensate for criticism from others
Compensatory strategies – rigid, dichotomous,
prevailing, constant, avoidance, seclusion, self-criticism,
self-blame (carried out to protect oneself, but only
cognitive distortions)
Characteristics of
Automatic Thoughts
Arise spontaneously
Unnoticed (preconscious), associated emotions more
often recognized
Specific thoughts → specific affects:
I am a failure → depression
I do not know what will happen tomorrow → anxiety
Individual unaware of presence, but easy to elicit
Characteristics of Automatic
Thoughts
Often brief & fleeting, in telegraphic form (I am worthless)
Verbal and/or imagery
Accepted as true, no reflection/evaluation
Universal; evaluated according to validity & functionality
In psychopathology - rigid, absolute truth, dysfunctional
Dysfunctional Automatic Thoughts
(Cognitive Distortions)
All or nothing (dichotomous) thinking
Catastrophizing
Emotional reasoning
Mind reading
Overgeneralization
Personalization
Discounting positive/magnifying negative
Eliciting Automatic Thoughts
• What thoughts, images, feelings went through your mind when the
specific event occurred (when thinking about the event)
• Ask question when noting a shift in affect during session
IF NEEDED
• Have the client describe a problematic situation. When noting
affective shift ask “what was going through your mind just then”
• Focus on emotions (what were you feeling), then ask about connected
thoughts
• Imagine situation
• Role-playing
Principles of CBT
Focus on present (here & now), problem-oriented
Structured (each session, whole treatment process, homework,
supervision)
Time-limited (improvement continues also after termination of )
treatment
Psychoeducational (familiarizes client with the CBT model, emphasizes
relapse prevention)
Importance of clients’ active role between sessions (homework )
Emphasizes therapist/client collaboration
Structure of Therapeutic Session
1. Setting agenda
2. Bridge from last session
3. Reviewing homework assignment from last session (e.g.,
mood check, activity chart, identification of
dysfunctional automatic thoughts)
Structure of Therapeutic Session
• Important to provide rationale for homework
• Ensure that client sees homework as
meaningful, understands assignment, agrees to
perform assignment & is able to perform
homework (experience of success)
• Give explicit instructions
• Start & rehearse assignment in session
• Insistence on completion of assignment.
Structure of Therapeutic Session
• Important to provide rationale for homework
• Ensure that client sees homework as
meaningful, understands assignment, agrees to
perform assignment & is able to perform
homework (experience of success)
• Give explicit instructions
• Start & rehearse assignment in session
• Insistence on completion of assignment.
Principles of CBT
Principles similar regardless of specific
psychopathology
Three stages
1. Psychoeducation on cognitive model, introduction of
behavioral techniques to replace maladaptive
with adaptive behavior
2. Cognitive technique to modify dysfunctional cognitions
3. Maintenance of change, prepare patient for termination,
relapse prevention
TREATMENT PLANNING
1. Initial Stage
• Establishing the therapeutic relationship
• Providing psychoeducation
• Setting goals
• Socializing patient with the cognitive model
• Socializing patients with the process of therapy
• Solving current problems/working toward
goals
• Eliciting, evaluating, responding to automatic
thoughts
• Modifying dysfunctional behaviors
• Teaching coping strategies
2. MIDPHASE
•
Continue previous activities
• Identify/conceptualize/modify dysfunctional
assumptions/beliefs
• Identify and modify dysfunctional coping
strategies
3. Final Phase
• Continue above activities
• Prepare patients for termination
• Problem-solving for predicted difficulties
3. Final Phase
• Teach self-therapy
• Identify early warning signs of relapse/
recurrence
• Develop (written) plans for relapse/recurrence
•3. Final Phase
• Restart mood check, activity chart
• Plan every day ahead
• Plan alternative activities & social contacts at
times of risk
• Confide in trustful others
CBT in depressed children and
adolescents
• Treatment of depression in children &
adolescents includes two stages
• 1. Amelioration of depressive symptoms in the
acute stage
• 2. Continuation of treatment to integrate the
skills learned in the acute stage in the long-run
CBT in depression in children and
adolescents - Principles
• Definition of treatment goals: focused, limited
(minimal), hierarchy, written plan
• Psychoeducation for kid & parents: e.g.,
difference between anergia and laziness;
written handouts
• Self-monitoring of mood, hopelessness,
suicidality, weekly goal checking
CBT in depression in children and
adolescents - Principles
• Behavioral activation & integration of
enjoyable activities: structured time table of
ADL with increasing hierarchy of challenge
• Behavioral activation may both depressive
symptoms & negative dysfunctional cognitions
• In severe depression, start with behavioral
activation & maintain it until some
improvement in depressive symptoms is
achieved before moving to cognitive module
CBT in depression in children and
adolescents - Principles
• Development of problem solving & personal
and interpersonal coping techniques
• Cognitive restructuring:
• Patient & therapist work together in the “court
of thoughts”
• What is the evidence supporting the
dysfunctional cognition
• Is there another possibility (raise doubts)
• What is the evidence supporting the new, more
functional cognition
CBT in depression in children and
adolescents - Principles
• Involvement of parents, goals for parents: depend on
the developmental phase of the kid & the abilities of the
family; individual or group parental consultation; goals
can change during treatment
• social skills & social relations; solving social
problems
• Consolidation of change & relapse prevention; the
importance of booster sessions
CBT in depression in children and
adolescents - Principles
• CBT in depressed children & adolescents
usually requires 12-16 individual sessions
• If required, specific modules may added for
comorbid problems, e.g. anxiety, impulsivity,
mood dysregulation, family & social problems
The Treatment of Adolescents with
Depression Study (TADS, March, 2004,
2007)
• 439 adolescents with varying severity of MDD
• 12 CBT sessions, Fluoxetine, CBT + Fluoxetine,
Placebo
• Hierarchy of improvement
• CBT + Fluoxetine (71%)
• Fluoxetine (61%)
• CBT (43%; not significantly different from placebo) vs.
60% in Brent et al’s (1997) study
• Placebo (35%)
The Treatment of Adolescents with Depression
Study (TADS, March, 2004, 2007)
• No differences after 9 months (86% improved in the
combined treatment; 81% in each separate treatment)
• No depression after 9 months:
• 55% Fluoxetine
• 64% CBT
• 60% CBT + Fluoxetine
• SSRIs speed the reaction to treatment rather than
enhance it
• Suicidal attempts/ideation: Fluoxetine 14.7%; CBT
6.3%; CBT + Fluoxetine 8.4%
ACTION Model for the treatment of depressed
young adolescents (NIMH; Stark et al, 2005a,b )
•
•
•
•
•
•
•
•
158 depressed girls age 9-13
CBT parents consultation vs. TAU (minimal contact)
22 biweekly sessions; small groups in school settings
No post-treatment depression:
84% in CBT
81% percent in CBT + parents consultation
46% in the control condition
Multiple specific CBT elements were associated with
improvement (but not non-specific therapist-related
factors)
Trials in Depressed Suicidal
Adolescents
• Treatment trials for depressed adolescents typically
exclude:
– Actively suicidal teens
– Often exclude those who are not acutely suicidal but
have a history of suicidal behavior
– Analyzing data of “new occurrences” of suicidal
behavior in the context of these trials is problematic
Treatment of Depressed Suicidal
Adolescents: State of the Art
• Only a few psychosocial trials of existing therapies
show efficacy data targeting suicidal behavior in
teens, with decreased attempts as outcome
• Only a few empirically supported, accessible
treatments for suicidal teens specifically target
suicidal behavior (DBT is geared more for
borderline personality disorder than for
depression)
Treatment of Depressed Suicidal Adolescents
TASA-CBT
• David Brent, Kim Poling - Pittsburgh PA
• Greg Brown - University of Pennsylvania, PA
• John Curry, Karen Wells - Duke University, NC
• Betsy Kennard - Southwestern University, TX
• Barbara Stanley, Larry Greenhill - Columbia
University, New York, NY
Modules of TASA-CBT
• Cognitive interventions - based on CT (Beck and
colleagues)
• Behavioral interventions - based on dialectical
behavioral therapy (DBT) (Linehan and
colleagues)
• Family therapy with behavioral focus
• Psychoeducation about depression & suicide
Key Characteristics of TASACBT
• Treatment is brief & goal-oriented, narrow in
focus and narrow in goals - prevention of future
suicidal behavior
• Depressive adolescents have in addition multiple
emotional problems, difficult family situations,
frequent school difficulties & comorbid disorders,
requiring other interventions in combination with
TASA-CBT
Key Characteristics of TASA-CBT
• In a brief treatment, only the most
important & immediate treatment goals are
addressed
• The target suicide attempt is the centerpiece
of the treatment
• Other problems are addressed primarily in
the way that they relate to suicidality
Key Characteristics of TASA-CBT
• Case conceptualization
– Identify skills, deficits & dysfunctional thinking
that led to the suicidal behavior
– Identify the adolescent’s strengths & natural
approach to problem solving – e.g., cognitive vs.
behavioral - and enhance these strengths first
Primary Techniques
1.
Safety plan: Emergency plan
2. Chain Analysis: Awareness of circumstances that
resulted in the attempt - “Behavior is understandable.
Things do not just happen.”
3.
Development of skills to cope in the future with
circumstances similar to those leading to present suicide
attempt. How to cope with:
a. immediate precipitants
b. long term vulnerability factors
3.
Relapse prevention: Revisiting the suicidal event with the
new skills developed in treatment
Safety Plan: What it is
• Hierarchically-arranged list of coping strategies
for use during a suicidal crisis or when suicidal
urges emerge
• Plan is a written document
• Uses a brief, easy-to-read, format
• Involves a commitment to the treatment process
Safety Plan: What it is not
• Safety plans are not “no-suicide contracts”
• No-suicide contracts ask patients to promise to stay alive
without telling them how to stay alive
• No-suicide contracts may serve to “protect” the institution
or therapist more than the patient
• Virtually no empirical evidence exists to support the
effectiveness of no-suicide contracts
Safety Plan: Overview of Process
• Safety plan includes a step-wise increase in
level of intervention from “within self”
strategies up to going to psychiatric ER
• Although the plan is hierarchically stepwise,
patients need to know that if they are
unable to carry out a specific step they do
not continue to try until succeeding, but
move on to the next step
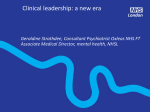
Safety Plan Form
Safety Plan Form
• A. Steps to make the environment safe: 1,2,3…
• B. Warning signs that problems may be
•
developing: 1,2,3
• C. Internal Coping Strategies: 1,2,3…
Safety
Plan
Form
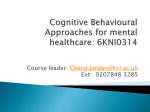
Safety
Plan
Form
D. External Strategies:
• People (peers, adults) who can help distract
me:1,2,3…
• Adults whom I can ask for help: 1,2,3…
• Professionals I can ask for help: 1,2,3…
• Therapist’s Name/Phone number
• Other Professionals’ Name/Phone number:1,2,3…
• Hospital ER Address/Phone number
Safety Plan - Summary
1. Adolescent agrees not to hurt himself/herself
2. Adolescent, parents & therapist construct & rehearse
strategies to cope with suicidal thoughts if significant
stressful precipitants occur (call a friend/parent, put a
video of a funny cartoon)
3. Adolescent tells parents/therapist if suicidal thoughts
continue
Safety Plan – Summary
4. Adolescent will present himself/herself to an
emergency service if no one is available to help
(emergency service personnel informed in advance).
5. In the period between sessions adolescent structures
activities that reduce suicidal risk with assistance of
parents/therapist (e.g., always has someone to call,
alcohol/weapons removed from the immediate
surroundings)
Next Steps in TASA-CBT
• Chain analysis
• Skills development & cognitive
restructuring
Connecting Safety Plan & Chain Analysis
• Link safety plan to relevant points in the patient’s chain
analysis description of the evolvement of suicidality
• Each strategy evaluated in the chain analysis can be tied to
a factor (vulnerability, cognitive, or behavior) that had an
influence on the evolvement of the attempted suicide
• Emphasize that the plan is fluid, and skills/strategies will
be added to the plan as required throughout the evaluation
& treatment
Chain Analysis - Case Example
• 15-year-old male adolescent who lives with his
parents, 12-year-old sister & 8 year old brother.
• Father is an electrician, mother worked as a
secretary, currently unemployed; financial
problems at home
• Chronic problems with sleep & parents; bad
student, despite over-average potential
Chain Analysis - Case Example
• Prior attempt (cut wrists) that parents did not
take seriously at the time; no intervention;
currently in treatment because of the abovementioned problems
• In the past week failed two tests, was told by the
school’s principal that he will not continue next
year if things do not change drastically
• Talked with his two-years girlfriend; she calmed
him for a while, as she usually does
Chain Analysis - Case Example
• Could not sleep. At 2am went to bathroom to take
Acamol (to sleep)
• Feelings: sad, desperate.
• Thoughts: “I Cannot handle these feelings
anymore”, “This is not going to end”.
• Felt a “wave of depression” & severe pressure in
chest & within a few seconds impulsively changed
his mind to take the pills in order to kill himself.
Swallowed 18-20 pills without water. Stopped
because he said it hurt him.
Chain Analysis - Case Example
• Calmed down and decided to go back to sleep.
• Did not tell anyone until the upcoming planned
psychological evaluation two days later
• Reaction to attempt: parents angry, girlfriend
supportive
Chain Analysis – Case Conceptualization
Predisposing Factors:
- Demographics
- Vulnerability factors:
Psychopathology (e.g. comorbidity)
Parental psychopathology (e.g. parental comorbidity, mother’s
unemployment, financial problems at home)
Other (e.g., chronic problems with sleep, school and parents,
prior attempt, parental reaction to prior attempt )
Triggers - e.g. failing tests, threat of being expelled
Protective Factors – e.g., good relations with girlfriend, good cognitive
potential
Chain Analysis – Conceptualization: Condition
before, during & following Attempt
• Cognitive: helplessness, hopelessness
• Emotional: sad, desperate
• Physiologic: severe pressure in chest
• Behavioral: impulsivity, not telling about attempt
• Contextual: told therapist, reactions of significant
others to the attempt
Next stage: Development of Adaptive
Coping Skills
• Identify with the adolescent skill deficits & areas
of adequate coping that can be strengthened
• Selection of skills is based on chain analysis
• Strategy - go with the teen’s natural strength do not try to remake the teen - & work with the
skills that are the most feasible & likely to prevent
future suicide attempts
Next stage: Development of Adaptive
Coping Skills
• If the teen takes to questioning and correcting
cognitive distortions, use that tactic
• If distress tolerance or emotion regulation skills
feel more natural, use these
Integration of Skills & Chain
Analysis
• Plans can be made for practicing the skill
• As new skills are learned, the chain is
revisited and the skill is fit into the chain
Intervention Strategies: Analysis of
Chain Segment
• Event: at 2am went to bathroom to take pills (to
sleep)
• Feelings: sad, hopeless, desperate.
• Thoughts: “I Cannot handle these feelings
anymore”. “This is not going to end”.
• Strategies: Cognitive restructuring; distress
tolerance; emotion regulation
Intervention Strategies: Analysis of
Chain Segment
• Felt “wave of depression” & within a few seconds
impulsively changed his mind to take the pills in
order to kill himself.
• Strategy: Invoke safety plan; problem solving
Intervention Strategies Treatment Planning Questions
• How can I help the patient feel better by
the end of the session?
• How can I help the patient have a better
week?
Intervention Strategies - Setting Goals
with Patients
WHAT DO YOU WISH TO CHANGE
• Make sure goals are rational & can be achieved
• Break larger goals into manageable ones
• Ensure goals are under the adolescent’s control
Intervention Strategies: Cognitive
Restructuring
Identification of Automatic thoughts:
“I Cannot handle these feelings anymore” –
Helplessness
“This is not going to end” –
Hopelessness
Cognitive Restructuring: Responding to
Automatic Thoughts
• Automatic Thought: “If I will be expelled from
school, there is nothing left for me to do ”
• Corrected response: “The principal still gives
me a chance; I can change my condition if I will
study with my girlfriend; even if I will be
expelled from school I can still go to another
school.”
Cognitive Restructuring: Developing
new Beliefs
• Avoid dichotomous beliefs; guide patient
toward adopting something in the middle
• “I am bad,” to “I can be okay.”
• “I’m incompetent, helpless” to “I have
strengths & weaknesses like everyone
else.”
Intervention Strategies: Cognitive
Restructuring
• Challenges to automatic thoughts:
Alternative possibilities, possible exceptions
• Cognitive restructuring coping cards:
Identify key cognitions that may evolve when the
individual becomes suicidal.
These thoughts are placed on one side of the card
On the other side, alternative, adaptive responses to these
thoughts are listed: “Although I am overwhelmed now, I
know that it can be temporary.”
Intervention Strategies: Distress
Tolerance (similar to DBT)
• Encourage use of distracting & self-comforting
techniques when urges to hurt oneself are high
• Identify with the patient which previously used
distracting & self-comforting techniques could
nave been useful in past attempts & can reduce
the risk of the next attempt
Intervention Strategies: Distress
Tolerance (similar to DBT)
• Example: listen to favorite music; watch TV; play
computer games; take a warm shower; talk to a
friend
• Identify with patient clues to decide when distress
tolerance techniques are needed again
Intervention Strategies: Distress Tolerance
Responses to Automatic Thoughts
• When I feel too depressed & anxious [to
cognitively respond to my automatic thoughts[
I can:
•
•
•
•
•
•
do controlled breathing
take a shower
listen to [specific music]
take a walk
call [specific friend]
read coping cards
Intervention Strategies– Distress
Tolerance Coping cards
When I am very distressed….
1. Read coping cards
2. Call:
Idan
Sarah
Ruth
3. Exercise:
Walk
Go to gym
Swim
Exercise videotape
Tell them I feel down but
then switch subject to
other everyday topics.
Intervention Strategies– Distress Tolerance
Coping cards
4. Relax:
Music
Magazine
Relaxation exercises
Controlled breathing
Intervention Strategies– Distress Tolerance
Coping cards
5.
Comfort myself:
Curl up with good book, quilt, stuffed bear
Take a shower, bath
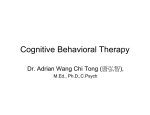
6.
Substitute to non-harming behaviors:
Ice cubes, rubber balls, hit pillow
פגיעה בעצמך
פגיעה באחרים
להכות בקיר
לזרוק דברים
שק אגרוף,מבקש משהו שיתפוס אותו
לצעוק ,לקלל ללא שליטה,
מרביץ לעצמי
נכנס מתחת לשמיכה ,מושך גומי על
האמה עד שיכאב
מקלל אחרים ,זז כל הזמן
מתקשר לחבר ,מכה בכר
קללות בתוך הראש /נושך אצבעות
רץ מחוץ לבית ,מוזיקה רועשת
מחשבות מתרוצצות ,כאב בטן ,בכי
יוצא מהבית ,מדבר לעצמו ,לוחץ כדור גומי
ביד,מסדר דברים ,סופר עד 10בלב
רעידות בידיים ,דפיקות לב ,מתעצבן ,קוצר נשימה
מעשן סיגריה ,מצייר,מקלחת חמה או
קרה
נשימות עמוקות,
שוטף פנים
הזעה ,סומק בפנים ,כוסס ציפורניים
תחושה של אי-שקט
רגוע
Intervention Strategies: Problem Solving
Module
•
Problem (s): Identify the problem(s), choose one
problem to work on (this step by itself cognitive
skills & flexibility)
•
Purpose: Brainstorm all possible solutions of this
problem (if no change is feasible use coping skills
to the influence of the situation)
•
Predict: Evaluate feasibility (pros & cons) of each
solution
•
Pick: Decide on one solution, based on the ability
to carry it out successfully
Intervention Strategies: Problem Solving
Module
• Plan steps required to carry out the
potential solution & check for potential
barriers
• Execution of solution
• Revaluation within the next 24 hours based
on process & outcome of the chosen
solution (to become an efficient problem
solver); positive reinforcement (pat on the
back) for effort
Intervention Strategies: Family Interventions
with Behavioral Focus
Brainstorm with family on alternative, more
efficient, coping strategies
• Too high expectations
• Positive reinforcement
• Attachment & commitment
• Negative emotions, criticism ( high EE)
Consolidation & Relapse Prevention – Core
Conceptualization
Set realistic goals
Differentiate between lapse and relapse
Have a prepared written plan
Consolidation & Relapse Prevention – Core
Conceptualization
Reinstitute past efficient techniques if
Worsening of problem
Sensing a risk of relapse
Significant expected imminent stress
Relapse Prevention
• Goals: To revisit the suicidal event with new
skills and ways of thinking to see how the
same circumstances may arise but the
outcome can be different
Steps in Relapse Prevention:
Introduction to Patient
• Provide a rationale for intervention & general
description
• Description of the steps involved in relapse
prevention
• Clinician determines that the patient understands
the nature of the module
Steps in Relapse Prevention:
Introduction of the program to the patient
• Clinician obtains permission from patient &
parents to introduce this module
• Clinician explains the potential for possible
negative emotional responses to the process & the
way to handle these response
• Clinician informs the patient that the task can be
stopped at anytime he/she desires
Relapse Prevention:
Review of Suicidal Event
• Patient & clinician determine if the patient is able
& willing to produce an image of the events
surrounding the past attempt
• This is done after the patient understands how this
process can be beneficiary. The patient can stop
the process at any time
Relapse Prevention: Review of Suicidal Event
• If this step is agreed upon, the clinician asks the
patient to:
• Imagine the sequence of events that led to the
attempted suicide
• Set the scene
• Elicit a detailed sequence of events
• Clinician focuses on key thoughts, assumptions,
emotions, physiologic reactions, behaviors &
contexts relevant to the attempt
Relapse Prevention: Review of Attempt
with new Skills
• Clinician encourages the patient to describe in
detail the coping skills and adaptive responses
developed during the treatment in the context of
specific key activating events of the attempt
• Clinician then asks the patient to imagine the
attempt again, this time taking into consideration
the influence of the new skills developed during
the treatment
Relapse Prevention: Future High Risk Scenarios
• Clinician asks the patient to imagine & describe a
hypothetical sequence of events that can lead to a future
attempt
• Clinician encourages the patient to identify specific
activating events & specific key thoughts, feelings, or
behaviors relevant to this future hypothetical attempt
• Clinician asks the patient to describe and imagine adaptive
responses - based on what has been learned during
treatment - to these activating events, cognitions &
behaviors
Relapse Prevention: Conclusion
• Patient summarizes what he/she has learned from
the whole intervention
• Clinician describes the changes that the patient
has made over the course of treatment.
• Clinician determines if there are issues identified
in this process that still remain a problem, and
how these should be handled.
• Clinician determines if the patient reports any
suicide ideation at the end of the intervention, and
how this should be handled.
Relapse Prevention: Conclusion
• Clinician reviews again the safety plan with
patient & family.
• Clinician emphasizes that the patient is able to
continue his/her progress during the next months
without being necessarily involved in an active
treatment regime (although some patients may
still require follow-up interventions)
• Clinician, patient & family decide on follow-up
procedure & other possible treatment
interventions in the future
TASA-CBT: Overview
Multimodal
Individual, family
psychoeducation
Safety first
Build on
Strengths
TASA-CBT
Targeted goal:
Skill
Relapse
Development
Prevention
Practical Considerations: Structure of
Treatment
• Individual sessions and family sessions (at least
one parent & teen)
• Frequency of sessions: weekly then biweekly
Practical Considerations: Structure of
Treatment
• Number of sessions
– Individual
– 12 sessions weekly, possibility of biweekly
– booster sessions up to week 22
– Family
– up to 6 sessions in first phase
– up to 6 in booster phase
– Maximum of 22 individual & 12 family sessions
Practical Considerations: Initial Sessions
• Description of treatment process
• Short term focus
• Development of safety plan: safety is
primary
• Chain analysis of suicide attempt
Practical Considerations: Middle Sessions
• Skills development: emotion regulation; mood
monitoring; distress tolerance; interpersonal
effectiveness
• Cognitive restructuring: identifying cognitive
distortions; generating alternative solutions
• Increasing hopefulness/decreasing hopelessness
• Focus on longer-term condition
Practical Considerations: Final Sessions
• Relapse prevention
• Review suicidal event
• Review event with new skills
• Plan post-treatment follow-up
TASA-CBT: Conclusions
• TASA-CBT is a skills focused, multimodal,
relapse prevention cognitive behavioral treatment
• TASA-CBT is based on the findings of previous
nonsomatic treatment studies in depressed suicidal
adolescents & on the vast clinical expertise of
clinicians specializing in the management of these
kids
• Although the results of the TASA-CBT are
promising, is still under investigation
CBT in Depressed Children & Adolescents:
Clinical Considerations
• CBT superior to TAU or no treatment for depressed
adolescents
• Between 50-85% of depressed adolescents treated with
CBT improve, compared to 20-75% of depressed
adolescents treated with TAU
• CBT (& IPT) can be considered an established
treatment for depressed adolescents as they have been
found efficacious in different samples investigated by
different independent teams
CBT in Depressed Children & Adolescents:
Clinical Considerations
• Empirical evidence regarding which intervention, or
which ingredient of a specific intervention, works best
for a given depressed adolescent, is still limited
• Gains following CBT are not uniform across all
domains of symptomatology & functioning
• Around 50% of depressed adolescents treated with
CBT may still show varying degrees of depression
following treatment
• Parents & other social agencies should be involved in
treatment, & should be considered important agents of
change
CBT in Children & Adolescents: Clinical
Considerations
CBT superior or as effective as any other nonsomatic therapy
in:
* Depression
* Substance use disorders, impulse control disorders, ADHD
* Anxiety disorders including panic disorder, agoraphobia,
social phobia, OCD, PTSD, separation anxiety disorder
* Bulimia nervosa, binge eating disorder
* Chronic insomnia, psychiatric disorders in patients with
significant medical illness, chronic pain
Advantages of CBT
• Improvement rate following treatment is around
60-70% in most DSM- IV Axis I disorders;
treatment effect may be maintained in the long run
• Combination of CBT and medications (e.g.,
SSRI’s) is probably superior to each treatment
modality alone in severe cases of depression,
substance use disorders, anxiety disorders & eating
disorders
Limitations of CBT
20-35% - no improvement
≥ 35% - dropout
Comorbid Cluster B personality disorders (particularly
borderline personality disorder) – unfavorable outcome; longer
modified CBT is required
Some treatment centers do not have access to CBT