Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Lymphopoiesis wikipedia , lookup
Immune system wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Adoptive cell transfer wikipedia , lookup
Adaptive immune system wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Monoclonal antibody wikipedia , lookup
Cancer immunotherapy wikipedia , lookup
Innate immune system wikipedia , lookup
Polyclonal B cell response wikipedia , lookup
X-linked severe combined immunodeficiency wikipedia , lookup
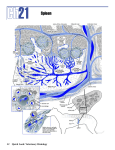
Hyposplenism Presented by: Melissa Smith Overview Definition of Hyposplenism Medical History The function of the spleen Congenital asplenia vs. splenectomy Immunological consequences of Hyposplenism Diagnosis and complications What is Hyposplenism? Hyposplenism is the lack of a spleen or its function The rare genetic disorder- Congenital Asplenia The surgical removal of the spleensplenectomy Results in severe immunological consequences. History Immunological importance of the spleen – Morris and Bullock-1919 First post-splenectomy infection – O’Donnell-1929 Effects of Hyposplenism – King and Shumacker-1952 The Spleen Largest lymphoid tissue of the body Serves two main functions – Filters blood to remove damaged/old RBC- red pulp – Serves as secondary lymphoid tissue by removing infectious agents and using them to activate lymphocyteswhite pulp A significant reservoir for T lymphocytes Plays an active role in the production of IgM antibodies and complement Has significant role in the functional maturation of antibodies Anatomy of Spleen Spleen Structure The white pulp is circular in structure and is made up mainly of lymphocytes. It functions in a manner similar to the nodules of the lymph node. The red pulp surrounds the white pulp and contains mainly red blood cells and macrophages. The main function of the red pulp is to phagocytize old red blood cells. White Pulp Red Pulp Congenital Asplenia Autosomal recessive genetic disorder Believed to be caused by absence of the Hox 11 gene in the embryo Causes decreased adaptive immune response Associated with structural abnormalities in other organs of the body- cause death in infancy Splenectomy Removal of spleen tissue (partial or complete) Usually needed because of trauma Residual splenic function in ¼ to ⅔ of patients IgM levels decreases, IgG levels remain constant or increase, IgA and IgE levels increase Immunological Consequences Causes slower and incomplete adaptive immune response against bacteria Low levels of tuftsin, which stimulates phagocytosis by neutrophils, macrophages, and monocytes Decreased neutrophil and macrophage activity Increased NK cell activity Limited capacity of circulating B-cells to differentiate into antibody-secreting cells Decreased level of T-cells Diagnosis Determined by anatomic presence or absence of the organ, its size, and any lesions. Function can be assessed by – Radiologic Techniques X-ray, ultrasound, tomography, MRI, radionucleotide scanning – Morphologically Peripheral blood smear- presence of Howell-Jolly bodies Howell Jolly bodies Howell-Jolly bodies are round, purple staining nuclear fragments of DNA in the red blood cell Complications Lifelong risk for Overwhelming Postsplenectomy infection (OPSI) – Caused by Streptococcus pneumoniae and gram negative bacteria – Initial Symptoms: fever, chills, muscle aches, headache, vomiting, diarrhea, and abdominal pain – Progressive symptoms: bacteremic septic shock, extremity gangrene, convulsions, and coma – Mortality rate of 50-80% from onset of initial symptoms, 68% of those deaths occur within 24 hours and 80% occur within 48 hours – Prevention: routine vaccinations and prophylactic antibiotics Summary Hyposplenism is the lack of a spleen or its function Can be either genetic or surgically induced It has detrimental effects on the immune system by decreasing the body’s ability to fight bacterial infections and reducing the adaptive immune response Resources Asplenia. Mudra Kumar, MD, MBBS, MRCP. EMedicine. 19 September 2005. http://www.emedicine.com/ped/topic150.htm Asplenia Defined. Families.com. 19 September 2005. http://encyclopedias.families.com/asplenia-112115-gecd Bowdler, Anthony J.. The complete spleen : structure, function, and clinical disorders . 2nd ed. Totowa, N.J. : Humana Press, 2002. Brigden, M. L. Detection, education and management of the asplenic or hyposplenic patient [a patient information handout is provided]. American Family Physician v. 63 no. 3 (February 1 2001) p. 499-508 Feder, H. M. J., et. al., Assessment of splenic function in familial asplenia. The New England Journal of Medicine v. 341 no. 3 (July 15 1999) p. 210-12 Gilbert-Barness, Enid., Diane E. Debich-Spicer. Handbook of pediatric autopsy pathology. Totowa, N.J. : Humana Press, c2005. Kanzler, B., et. al., Hox11 acts cell autonomously in spleen development and its absence results in altered cell fate of mesenchymal spleen precursors. Developmental Biology v. 234 no. 1 (June 1 2001) p. 231-43 Neiman, Richard S., Attilo Orazi. Disorders of the spleen . 2nd ed. Philadelphia : W.B. Saunders, c1999. Romanovsky, A. A., et. al., The spleen: another mystery about its function [Editorial]. American Journal of Physiology v. 284 no. 6 (June 2003 pt2) p. R1378-9 Sunder-Plassmann, G., et. al., Functional asplenia and vasculitis associated with antineutrophil cytoplasmic antibodies. The New England Journal of Medicine v. 327 (August 6 1992) p. 437-8 Tice, A. Hope for patients with asplenia or hyposplenism [editorial]. American Family Physician v. 63 no. 3 (February 1 2001) p. 439-40