Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Discovery and development of integrase inhibitors wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Discovery and development of ACE inhibitors wikipedia , lookup
Metalloprotease inhibitor wikipedia , lookup
Psychopharmacology wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Discovery and development of antiandrogens wikipedia , lookup
Neuropharmacology wikipedia , lookup
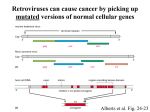
Iressa: The Development of an Effective EGFR Inhibitor Kevin Batten PHCY 503: Research Paper November 9, 2015 Cancer has always been a troublesome disease to treat because it has so many variations and we are continuing to learn new mechanisms behind it. One such mechanism is EGFR (epidermal growth factor receptor) mutations, which are particularly difficult to manage because they are not responsive to chemotherapy and many other common treatments for cancer.5 EGFRs are associated with lung, prostate, bladder, renal, breast, and ovarian cancers.2 After ligands bind the receptor they require dimerization and transphosphorylation in order to become active and lead to cell proliferation. Iressa is a recent tyrosine kinase inhibitor that prevents transphosphorylation and thus stops unregulated growth of cancer cells.1 Iressa, also known as ZD1839 or Gefitnib, belongs to the 4-anilinoquinazoline class of drugs.3 These drugs all share electron donating groups at positions 6 and 7, a lipophilic group at the meta position of the aniline, a CH group at positions 2, 5, and 8, and a free amine group at the fourth position.3 They made slight changes to the structure and went through 3 prototype drugs before the discovery of Iressa. ZD1839 is different in that it has a chlorine replacing the methyl group and a fluorine at the para position of the aniline (Figure 1).3 These changes prevent it from being metabolized as quickly as the previous versions, which increases its bioavailability and allows it to be useful as an oral drug.3 It is less potent than the prototypes, but the bioavailability makes up for it and it is potent enough to be taken once daily.3 The optimum dose is 250 mg/day, and side effects include diarrhea, acne/rash, nausea, asthenia, and vomiting.1, 2 Some side effects are more common than others (Figure 2). It is important to determine the optimal dose of a drug, but other doses also need to be tested to find out what other side effects the drug may have. Once study focused on this as they tested 88 patients who were diagnosed with various tumor types.5 They found that higher doses of Iressa led to toxicity and an increase in the severity of side effects. It was better tolerated at doses less than 600 mg/day and diarrhea and rash were the most common. There was antitumor activity at all levels of dosing, but at 250 mg/day there is the best balance between anticancer activity and ill effects.5 Also, they found that the mean half-life of the drug was 30.5 hours, which confirms that it has good bioavailability.5 They also tested its use with a combination of other drugs such as cisplatin and found that the therapy was still well tolerated. Cisplatin is a DNA damaging agent, so it can attack the DNA replication of cancer cells while they are slowed down by Iressa.5 It is now used in combination with other drugs so cancer has less of a chance to resist treatment.5 Iressa is selective for tumors because they display a lot more EGFRs on their surface than normal tissues.1 When a ligand binds the EGFR it dimerizes and then is phosphorylated. After phosphorylation, secondary messengers are activated such as SOS, MEK and RAS.1 Inhibiting the EGFR leads to an accumulation of p27 kinase inhibitor and hypophosphorylated Rb protein that leads to cell arrest at G1 of the cell cycle.5 The second messengers normally lead to gene transcription and progression of the cell cycle, and high activity of the EGFR causes cancer because cell growth is no longer regulated. This also leads to invasion, resistance to apoptosis, metastasis, and angiogenesis (Figure 3).1 Iressa prevents this by binding to the receptor and not allowing it to complete transphosphorylation. It is important to prevent growth of the tumor before it is able to metastasize and spread throughout the body. Once that happens it is difficult to contain and the prognosis for the patient is much worse. EGFR mutations have been resistant to chemotherapy and standard treatment, so it is essential to come up with new drugs to counter it. The net result of Iressa is a decrease in tumor size and in some cases regression of the cancer (Figure 4).2 The fight against cancer continues on, but there continues to progress in the world of pharmacy. EGFR inhibitors such as Iressa add another way to suppress cancer selectively rather than just trying to kill it by increasing the dose of radiation. This way tumors can be approached with multiple mechanisms of treatment because Iressa can be combined with traditional therapy to have a greater impact. It may not be a cure, but it will help extend the lives of patients and give hope to those who have not benefitted from standard treatment. ZD1839 showed that a few modifications to a structure can make all the difference during drug development. Innovations such as EGFR inhibitors are essential if we want to be serious about putting an end to cancer. References 1. Armour A.A, Watkins C.L. The challenge of targeting EGFR: experience with gefitinib in nonsmall cell lung cancer. ERS Publication. September 2010. DOI: 10.1183/09059180.00005110 2. Herbst Roy, Maddox Anne-Marie, Rothenberg Mace, Small Eric, Baselga Jose, Rojo Federico, Hong Waun Ki, Swaisland Helen, Averbuch Steven, Ochs Judith, and Lorusso Partricia Mucci. Selective Oral Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitor ZD1839 Is Generally Well-Tolerated and Has Activity in Non–Small-Cell Lung Cancer and Other Solid Tumors: Results of a Phase I Trial. Journal of Clinical Oncology. September 2002. DOI: 10.1200/JCO.2002.03.038 3. Barker AJ, Gibson KH, Grundy W, Godfrey AA, Barlow JJ, Healy MP, Woodburn JR, Ashton SE, Curry BJ, Scarlett L, Henthorn L, Richards L. Studies leading to the identification of ZD1839 (iressa™): an orally active, selective epidermal growth factor receptor tyrosine kinase inhibitor targeted to the treatment of cancer. Bioorganic and Medicinal Chemistry Letters. Volume 11, Issue 14, Pages 1911–1914. July 2001. DOI: 10.1016/S0960-894X(01)00344-4 4. Wakeling Alan P, Guy Simon P, Woodburn Jim R, Ashton Susan E, Curry Brenda J, Barker Anderw J, and Gibson Keith H. ZD1839 (Iressa): An Orally Active Inhibitor of Epidermal Growth Factor Signaling with Potential for Cancer Therapy. Cancer Research. October 2002. 62; page 5749-5754. 5. Baselga J, Rischin D, Ranson M, Calvert H, Raymond E, Kieback D.G, Kaye S.B, Gianni L, Harris A, Bjork T, Averbuch S.D, Feyereislova A, Swaisland H, Rojo F, and Albanell J. Phase I Safety, Pharmacokinetic, and Pharmacodynamic Trial of ZD1839, a Selective Oral Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitor, in Patients With Five Selected Solid Tumor Types. Journal of Clinical Oncology. November 2002. Volume 20. DOI: 10.1200/JCO.2002.03.100 Figure 1: The chemical structure of Iressa. Taken from:Wakeling Alan P, Guy Simon P, Woodburn Jim R, Ashton Susan E, Curry Brenda J, Barker Anderw J, and Gibson Keith H. ZD1839 (Iressa): An Orally Active Inhibitor of Epidermal Growth Factor Signaling with Potential for Cancer Therapy. Cancer Research. October 2002. 62; page 5749-5754. Figure 2: A graph showing the proportion of patients who experienced different grades of side effects while on Iressa (all dose levels were tested). Taken from: Herbst Roy, Maddox Anne-Marie, Rothenberg Mace, Small Eric, Baselga Jose, Rojo Federico, Hong Waun Ki, Swaisland Helen, Averbuch Steven, Ochs Judith, and Lorusso Partricia Mucci. Selective Oral Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitor ZD1839 Is Generally Well-Tolerated and Has Activity in Non–Small-Cell Lung Cancer and Other Solid Tumors: Results of a Phase I Trial. Journal of Clinical Oncology. September 2002. DOI: 10.1200/JCO.2002.03.038 Figure 3: This image shows the EGFR Iressa inhibits. It includes the tyrosine kinase area Iressa binds, the secondary messengers, and the overall effects. Taken from: Armour A.A, Watkins C.L. The challenge of targeting EGFR: experience with gefitinib in nonsmall cell lung cancer. ERS Publication. September 2010. DOI: 10.1183/09059180.00005110 Figure 4: Image is a tomographic scan of a patient after one month of Iressa treatment. They are already having a partial response to treatment as seen by the decrease in tumor size; this was after no response from chemotherapy. Taken from: Herbst Roy, Maddox Anne-Marie, Rothenberg Mace, Small Eric, Baselga Jose, Rojo Federico, Hong Waun Ki, Swaisland Helen, Averbuch Steven, Ochs Judith, and Lorusso Partricia Mucci. Selective Oral Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitor ZD1839 Is Generally Well-Tolerated and Has Activity in Non–Small-Cell Lung Cancer and Other Solid Tumors: Results of a Phase I Trial. Journal of Clinical Oncology. September 2002. DOI: 10.1200/JCO.2002.03.038