Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
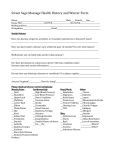
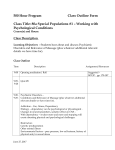
All Sports and Wellness 110 Dartmouth road Bedford N.S. B4A 2L7 Phone: (902) 431-5224 Cell: (902) 830-7677 HEALTH HISTORY FORM For your information : An accurate medical history is important to ensure that it is safe for you to recieve a massage treatment .All information gathered treatment purpose is confidential,except as required or allowed by law.If needed to be asked to provide written authorization for release of any information to other health care practitioners to facilate assessment or treatment. Name:___________________________________________ Date of birth :_______________________________________ Adress:_______________________________ City: _______________Postal Code : ________________________________ Phone N.(Home):______________________ (Cell) : ___________________ (Work):________________________________ E-mail Adress: _____________________________________Occupation:_________________________________________ General Practionner : ________________________________Who refered you ?__________________________________ Have you had a massage before ? Yes / No. How would you decribe your health ? Good / Fair /Poor Please describe your quality of sleep? Good / Fair /Poor. how much of water do you drink a day ? ____ Litres /Cups Please list all forms and frequency of stress reduction activities,Hobbies,exercise,sports Participation : ______________________________________________________________________ What is your primary complaint? ______________________________________________________ What symptoms are you experiencing ? _____________________ Are you experiencing any Night Pain ? : YES / NO Chose one or more to describe your pain :Dull / Aching, Sharp / Sharp shooting, Numbness / Tingling , Throbbing / Diffuse Mark “X”for conditions that pply to you CARDIOVASCULAR Aneurysm High Blood Pressure Low Blood Pressure Heart Disease Stroke Varicose Veins Phlebitis Bruise Easily Pace Maker Muscle/Joint Arthritis Type: Location: Fibromyalgia Pain/ stiffness in: Head Neck Jaw Back Low, Mid, Upper RESPIRATORY Bronchitis asthmas Emphysema Sinusitis Tuberculosis Breathing Problems Specify: SKIN Plantar Warts Eczema Psoriasis Fungal Infection/ Athletes Foot Herpes Simplex Skin Condition Specify: Nervous Multiple Sclerosis Seizure/ Epilepsy Carpel tunel Syndrome Altered Sensation: Where: Digestive Other Enviromental Illness Diabetes HIV/AIDS Cancer Chronic Fatigue Syndrome Women Only Menopausal problems Pregnant Due Date: Arms/Hands Other: Legs/Feet Endometriosis Osteoporosis Others (Specify): Other: SURGERIES PREVIOUS INJURIES: Type: TYPE: Type: DATE: SPECIAL NEEDS OTHER MEDICAL CONDITIONS CURRENT MEDICATIONS: (including aspirin,Ibuprofen, etc) Type: For: Type: For: ANY PIN, WIRE IMPLANTS, ARTIFICIAL JOINT? LIST: ANY ALLERGIES? Section Painful Menstruation Last Taken Last Taken All Sports and Wellness 110 Dartmouth road Bedford N.S. B4A 2L7 ADNAN RASSI, RMT 06086 Phone: (902) 431-5224 Cell: (902) 830-7677 INFORMED CONSENT TO MASSAGE THERAPY TREATMENT By signing below, I verify that the information given on the accompanying Health History form is true and accurately reflects Health status change in the future. I understand that, as in health care, in the practice of massage therapy there are some very slight risks to treatment including, but not limited to, aggravation of symptoms and residual muscle sorness, i do not expect the massage to be able to anticipate and explain all risks and complications and I wish to rely on the massage therapist to exersice judgment during the course of treatment, I understand that the beneficial effects and possible risk factors of massage therapy in general and the specific treatment of my condition will be explaind to me. I intend this consent to apply to all my recent and future massage therapy treatments. I understand that this consent(undress your comfort level, get ready between the sheet, question will be asked by the therapist about drapping and pressure,patient allow to ask question at any time during treatment,benefit of the treatment decrease pain and increase range of motion, side affects you may feels soreness for couples of days so you should increase fluid intake and do your home care exersices,treatment can be modified or withdrawn by me at any time. Appointments: Your appointment time is reserved especially for you. If you find it necessary to reschedule your appointment, a minimum of 24 hours is required so that others who need an appointment may be accomodated. Otherwise, you may be billed for your missed appointment. PATIENT FEES We accept Cash, Personal Cheques, Debit, Visa, Or Master card 30 Minutes 60 Minutes 75 minutes initial Assessment $ 80.00 $ 50.00 45 Minutes $ 80.00 90 Minutes There is a $25 charge for all NSF Cheques Printed Client’s Name:___________________________________ Signature of client (Or Parent Guardian):___________________ Date:__________________________ $ 65.00 $ 120.00