Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
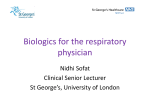
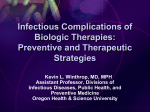
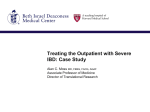
Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 To Print: Click your browser's PRINT button. NOTE: To view the article with Web enhancements, go to: http://www.medscape.com/viewarticle/503520 Tumor Necrosis Factor Alpha Inhibitors for the Treatment of Dermatologic Diseases Jennifer T. Trent; Francisco A. Kerdel Dermatol Nurs. 2005; 17 (2): 97-108. ©2005 Jannetti Publications, Inc. Abstract and Introduction Abstract Tumor necrosis factor alpha (TNF α) is involved in cell differentiation, mitogenesis, cytotoxic responses, inflammation, immunomodulation, and wound healing. Because of its numerous roles, it was thought that inhibition of TNF may aid in the treatment of certain dermatologic diseases such as psoriasis, hidradentitis suppurativa, pyoderma gangrenosum, Behcet's syndrome, and graft versus host disease. The efficacy of these agents has proven impressive and short-term side effects have been few and relatively benign. Introduction Tumor necrosis factor alpha (TNFα) is a cytokine involved in various activities in the human body (Gottlieb, 2001; Gottlieb & Bos, 2002; Lebwohl, 2003; Williams & Griffiths, 2002). It can be synthesized mainly by monocytes and macrophages; however, in the skin, keratinocytes, melanocytes, Langerhans cells, activated T cells, NK cells, and mast cells can produce TNFα. Synthesis can be induced by a variety of stimuli, including infectious organisms and even keratinocyte death. Trans forming growth factor beta, and interleukin 4 and 10 can inhibit the synthesis of TNFα (LaDuca & Gaspari, 2001). TNFα exerts its affects through the interaction with its cell surface receptors TNFα-R1 and R2, which are present on most cells of the body. Three soluble TNFα mono mers join together to form a homotrimer. This homo trimer can bind a maximum of three receptors. The cross linking of these receptors initiates a signal transduction pathway that activates nuclear factor kappa B, activation protein 1, interleukin (IL) 6, and cAMP responsive element binding protein, thereby causing the transcription and expression of various genes. TNFα is involved in cell differentiation, mitogenesis, cytotoxic responses, inflammation, immuno-modulation, and wound healing (LaDuca & Gaspari, 2001; Victor & Gottlieb, 2002). Because of its numerous roles, it was thought that inhibition of TNFα may aid in the treatment of certain diseases. Thus, infliximab (Remicade® ) and etanercept (Enbrel® ), both inhibitors of TNFα, were born. More recently, adalimumab (Humira ® ), a fully humanized monoclonal antibody to TNFα, has also joined this group (Weinblatt et al., 2003). Various studies and reports in the literature have extolled the benefits and success of these agents in the treatment of many conditions. The use of infliximab and etanercept for the treatment of psoriasis and psoriatic arthritis, hidradenitis suppurativa, pyoderma gangrenosum, and graft versus host disease will be discussed. Psoriasis Psoriasis is a chronic, inflammatory disease which can affect the skin, tendons, ligaments, and joints (Gottlieb, 2001; Gottlieb & Bos, 2002; Lebwohl, 2003). It has a multifactorial inheritance in which several genes interact with environmental factors to produce varying degrees of severity. Prevalence rates range from 0.5% to 4.6% depending on the country and race (Lebwohl, 2003). It more commonly affects Caucasians and patients living at higher latitudes (Lebwohl, 2003). Although it is not a life-threatening condition, it can lead to significant impairment and psychological stress. Patients who are severely afflicted can have up to 100% body surface area involvement. There are several clinical variants of psoriasis, including plaque, guttate, erythrodermic, and pustular (Lebwohl, 2003). Plaque type is the most common form, representing 80% of cases, while guttate, erythrodermic, and http://www.medscape.com/viewarticle/503520_print Page 1 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 pustular account for 10%, 3%, and 3% of patients respectively. Cutaneous lesions usually precede joint disease in 70% of patients with psoriasis. Psoriatic arthritis, a seronegative arthopathy, can affect upwards of 42% of patients with psoriasis (Lebwohl, 2003). Several forms exist, including polyarticular, oligoarticular, distal interphalangeal, arthritis mutilans, spondylitis, and sacroiliitis. Like rheumatoid arthritis, psoriatic arthritis can lead to joint deformities, disability, and increased mortality. Pathogenesis While the entire pathogenesis of psoriasis remains largely unknown, recent discoveries have been made which have elucidated the pivotal role of T cells (Lebwohl, 2003). This discovery was made through the use of severe combined immunodeficiency mouse models and further supported by the dramatic response to agents such as methotrexate, cyclosporin, and denileukin diftitox, all of which modulate T-cell activity (Gottlieb, 2001). This process begins with the presence of antigens, which cause the maturation of Langerhans cells and the migration of antigen-presenting cells (APC) to the lymph node. Once in the lymph node, the APCs interact with naEFve T cells, causing T-cell activation and subsequent T-cell proliferation. Some of these proliferating T cells are memory T cells, which ultimately migrate to the inflamed target areas of the skin. When these T cells are activated, they will release type 1 cytokines (Th1), such as interferon gamma, IL-2 and IL-12, and TNF (Gottlieb, 2001; Gottlieb & Bos, 2002). These cytokines are responsible for keratinocyte proliferation and lack of maturation, and vascular changes characteristic of psoriasis. Treatment Three broad categories of treatment options exist for psoriasis, including topical modalities, phototherapy, and systemic therapy (Lebwohl, 2003). Topical treatments are effective for patients with mild-to-moderate psoriasis, while phototherapy and systemic medications are appropriate for more severe cases. These topicals include topical steroids, tar, anthralin, vitamin D analogues, and retinoids. Phototherapy encompasses treatment with PUVA, broadband and narrowband UVB, and the 308 nm excimer laser (Lebwohl, 2003). Prior to beginning PUVA, laboratory tests, such as antinuclear antibodies, should be performed. This is to ensure that the patient does not harbor undiagnosed collagen vascular disease/photosensitivity. Also, since psoralen, which is ingested prior to UVA exposure, is a photosensitizer and can cause heptotoxicity, liver function tests should be obtained. In patients afflicted with severe psoriasis, systemic therapies have been effective, but some carry significant side effects (Lebwohl, 2003). Several systemic medications can be used for psoriasis, such as methotrexate, cyclosporin, retinoids, and more recently targeted immunotherapies (biologics). Patients treated with methotrexate must be monitored for bone marrow and hepatic toxicities. Retinoids can cause mucocutaneous side effects, hair loss, nail thinning, and teratogenicity. Cyclosporin use can lead to nephrotoxicity, hypertension, or development of lymphomas with prolonged use; therefore, its use is usually limited to 1 year. Recently targeted immunotherapies have become popular alternatives for patients with severe psoriasis. These treatments target specific cells, cytokines, or interactions to achieve remission (Lebwohl, 2003). Not only are these alternatives effective, but they have a more favorable side effect profile than the traditional systemic agents. Alefacept (Amevive ® ) and denileukin diftitox (Ontak ® ) are fusion proteins which eliminate activated T cells by targeting the interaction between LFA3 on APC and CD2 on T cells, and by binding to IL2 receptor (CD25) to release diphtheria toxin, respectively. Inhibition of T-cell activation/proliferation has been achieved with several therapies, including a monoclonal antibody to anti-CD4, anti-CD80, anti-CD25 (daclizumab), anti-CD11a (efalizumab), and anti-CD2 (siplizumab). Also, CTLA4Ig is a fusion protein which binds to CD80 and CD86 on APCs to inhibit T-cell activation. Immune deviation has been achieved through the use of IL4 and 10, which are type 2 cytokines (Th2) that counteract the Th1 predominance found in psoriasis. Finally, inhibition of cytokines is accomplished with infliximab (Remi cade ® ), a chimeric mouse-human monoclonal antibody which inhibits TNFα (see Figures 1 & 2); etanercept (Enbrel® ), a fusion protein which inhibits TNFα (see Figures 3-6); adalimumab (Humira ® ), a fully humanized monoclonal antibody to TNFα; and anti-IL8. http://www.medscape.com/viewarticle/503520_print Page 2 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 Figure 1. Severe psoriatic involvement of most of the trunk, prior to the start of infliximab therapy. http://www.medscape.com/viewarticle/503520_print Page 3 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 Figure 2. Resolution of psoriasis, after completion of infliximab therapy. http://www.medscape.com/viewarticle/503520_print Page 4 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 Figure 3. Significant psoriatic involvement of the hands, prior to the use of etanercept. Figure 4. Resolution of psoriasis, after 16 weeks of etanercept therapy. http://www.medscape.com/viewarticle/503520_print Page 5 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 Figure 5. Large psoriatic plaques on the breast, prior to starting etanercept. Figure 6. Complete resolution of psoriatic plaques, after 16 weeks of etanercept. http://www.medscape.com/viewarticle/503520_print Page 6 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 Infliximab (Remicade® ) Infliximab is a chimeric monoclonal IgG antibody which inhibits TNFα activity and triggers complement mediated lysis of TNFα expressing cells in vitro (Gottlieb, 2001; Gottlieb & Bos, 2002; LaDuca & Gaspari, 2001; Lebwohl, 2003; Victor & Gottlieb, 2002; Williams & Griffiths, 2002). It is made from human constant and mouse variable regions of IgG. It neutralizes soluble and blocks membrane-bound TNFα. It is FDA approved for the treatment of Crohn's disease and rheumatoid arthritis (RA) at intravenous doses of 5 mg/kd and 3 mg/kg respectively. The infusion is given over at least 2 hours and has a half life of 8 to 10 days (Williams & Griffiths, 2002). Crohn's disease without fistulas is treated with one dose of infliximab at 5 mg/kg, while the presence of fistulas requires three doses of 5 mg/kg at weeks 0, 2, and 6. RA is treated with 3 mg/kg at weeks 0, 2, 8, and every 8 weeks thereafter. It was discovered that infliximab was effective in treating psoriasis after a patient with recalcitrant Crohn's and psoriasis was treated with infliximab for her Crohn's (LaDuca & Gaspari, 2001; Victor & Gottlieb, 2002). After the infusion, not only did her Crohn's improve, but also her psoriasis. In a randomized double blind placebo controlled trial, 33 patients were randomized to a placebo arm, a 5 mg/kg arm, or a 10 mg/kg arm and treated on weeks 0, 2, 6 (Chaudhari et al., 2001). Eighty-two percent of patients in the 5 mg/kg arm, 91% of patients in the 10 mg/kg arm, and 18% of patients in the placebo arm achieved a greater than 75% improvement on Psoriasis Index and Severity Score (PASI) after 10 weeks. Treatment began working within 2 weeks and sustained this improvement for more than 6 months. Immunohistochemical staining showed decreased epidermal inflammation and normalization of keratinocyte differentiation. No serious adverse effects were noted. Phase II open label data showed that 55% of patients with psoriasis treated with infliximab retained a 50% or greater reduction in the original PASI scores after 26 weeks, with no further infusions (Gottlieb, Chaudhari, Mulcahy, Dooley, & Baker, 2003). Infliximab was also successful in the treatment of pustular psoriasis, a severe, debilitating, and recalcitrant variant of psoriasis. Elewski (2002) treated two patients with infliximab 5mg/kg on weeks 0, 2, and 6. The patients tolerated the infusion well without any side effects. Clearance began within the first few days after the first infusion with continued improvement until complete clearance. This complete clearance was maintained for 10 weeks after the last infusion. Newland, Weinstein, and Kerdel (2002) reported one case of pustular psoriasis treated successfully with one infusion of infliximab 5 mg/kg. Complete resolution of the pustules occurred by day 4. The infusion was well tolerated without any side effects. In a 6-month trial, 12 patients with recalcitrant psoriatic arthritis were treated with infliximab 5 mg/kg on weeks 0, 2, 6, 14, 22 along with their previous treatments of steroids and methotrexate (Provenzano, Termini, Le Moli, & Rinaldi, 2003). No infusion reactions were noted. Two patients were withdrawn from the study, one for angina pectoris and one for pulmonary malignancy, which were not considered a result of the infliximab infusions. Significant improvement was noted in all patients. An open label pilot study was conducted with 21 patients with recalcitrant spondyloarthropathy, 9 of which had psoriatic arthritis (Van Den Bosch et al., 2000). They were treated with infliximab 5 mg/kg at weeks 0, 2, 6, along with methotrexate. Rapid and significant improvement was noted in all patients without any significant side effects. PASI scores showed significant improvement at day 14 compared to baseline, and this improvement was sustained at day 84. Global and peripheral assessment of psoriatic arthritis showed significant improvement in all areas at day 14 compared to baseline, and this significant improvement was maintained at day 84. Drawbacks are few and include headache, diarrhea, rash, pharyngitis, rhinitis, cough, upper respiratory infection, and urinary tract infection (LaDuca & Gaspari, 2001; Lebwohl, 2003; Mease, 2002; Provenzano et al., 2003; Van Den Bosch et al., 2000; Williams & Griffiths, 2002). Rare instances of more severe side effects have occurred, such as reactivation of pulmonary tuberculosis, aseptic meningitis, sepsis, and development of anti-dsDNA and systemic lupus. Keane et al. (2001) reported 70 cases of TB developing after the use of infliximab, 40 of which had extrapulmonary disease. The incidence of TB with infliximab is much higher than with etanercept. This reactivation of TB has been attributed to immune system disruption, manifested as the failure of granulomas to compartmentalize the bacilli, and inhibition of macrophage apoptosis after the use of infliximab. Patients are required by the Food and Drug Administration to have a negative purified protein derivative (PPD) test and negative chest radiograph prior to starting infliximab therapy. There is also concern of long-term development of antibodies to the drug. In patients with Crohn's treated with repeated infusions of infliximab, 13% developed antibodies against the medication (Tan, Gordon, Lebwohl, George, & Lebwohl, 2001). The presence of these antibodies has lead to the loss of clinical efficacy, the development of infusion reactions, chest pain, bronchospasm, and anaphylactic shock. The rate of antibody formation is inversely related to dose and decreases http://www.medscape.com/viewarticle/503520_print Page 7 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 with the addition of low-dose methotrexate (Lebwohl, 2003). How this will translate in patients with psoriasis remains to be seen. Infusion reactions, such as anaphylaxis and bronchospasm, can occur rarely, and can be treated by slowing the infusion rate and pretreating with antihistamines or steroids. Relative contraindications to the use of infliximab include congestive heart failure, demyelinating disorders, lupus, lymphoma/malignancy, antibody formation to infliximab, hypersensitivity to murine products, and sepsis. Infliximab is a pregnancy class B drug. Etanercept (Enbrel® ) Etanercept is a recombinant human TNFα receptor fusion protein, which consists of the extracellular domains of two TNFα receptor p75 receptors and the constant (Fc) region of IgG1, which inhibits soluble TNFα. In contrast to infliximab, etanercept binds to and inhibits only soluble TNFα (Gottlieb, 2001; Gottlieb & Bos, 2002; LaDuca & Gaspari, 2001; Lebwohl, 2003; Victor & Gottlieb, 2003; Williams & Griffiths, 2002). It is FDA approved for the treatment of adult rheumatoid (RA) and psoriatic arthritis (PA) at doses of 25 mg twice a week administered subcutaneously. It was noted that in the treatment of patients with PA, their psoriasis improved as well (Davison, Bunker, & Basarab, 2002; Galadari, Fuchs, & Lebwohl, 2003; Iyer, Yamauchi, & Lowe, 2002; Kurschat et al., 2001). Mease et al. (2002a) enrolled 60 recalcitrant psoriatic arthritis patients in a double-blind placebo-controlled study comparing subcutaneous injections of etanercept 25 mg twice a week to placebo. Patients continued on metho trexate. After 12 weeks, 87% of etanercept-treated patients versus 23% of placebo-treated patients responded significantly based on the Psoriatic Arthritis Response Criteria (PsRC). Using the American College of Rheumatology criteria (ACR20), statistically significant improvement was noted in 73% of the etanercept-treated patients and 13% of the placebo-treated patients at 12 weeks. Also, 26% of the etanercept-treated patients had a 75% improvement in PASI scores, while none of the placebo patients improved. Only 20 of the patients reported side effects, namely injection site reactions, but no significant side effects were noted. After 4 months of followup, five patients had no joint pain and 55 had only mild symptoms. In the phase III trial of etanercept for PA, there was a median improvement in PASI in 33% in the etanercept group and none in the placebo groups (Mease et al., 2000a). In a subsequent 12-week double-blind placebo-controlled study of etanercept for psoriasis, 70% of patients given etanercept had improvement in their PASI scores (Gottleib, Matheson, Lowe, & Zitnik, 2002). Fifty-six percent of patients treated with etanercept and 5% of placebo-treated patients had a 75% reduction in PASI scores at 24 weeks. The most common side effect was injection site reactions (Gottleib et al., 2002; Mease et al., 2000a; Mease, Goffe, & Betz, 2000b). Other uncommon side effects were upper-respiratory infections, headache, rhinitis, abdominal pain, vomiting, pharyngitis, nausea, gastrointestinal infection, and rash. Antibody formation is less likely to occur in etanercept-treated patients compared to infliximab (Lebwohl, 2003). Thirteen cases of TB reactivation have been reported (Goffe & Cather, 2003; Keane et al., 2001). Unlike infliximab, etanercept-associated TB occurs sporadically and later in the course of treatment. Even though the FDA does not require a negative chest radiograph and PPD, both should be performed. More serious reactions have occurred, including demyelinating disorders, aplastic anemia, allergic reactions, and development of positive ANA, anti-dsDNA, and drug-induced systemic lupus. No malignancies have been discovered during the FDA trials; however, Smith and Skelton (2001) reported seven cases of squamous cell carcinoma occurring in patients with RA treated with etanercept (Smith & Skelton, 2001). It has been found in long-term RA studies using etanercept that the incidence of malignancy was not increased over age-matched controls (Goffe & Cather, 2003). Relative contraindications to use of etanercept include sepsis, malignancy, congestive heart failure, and demyelinating diseases. It is a pregnancy class B drug. Hidradenitis Suppurativa Hidradenitis suppurativa (HS) is a chronic, inflammatory scarring cutaneous condition affecting the apocrine sweat glands, which usually presents after puberty (Katsanos, Christodoulou, & Tsianos, 2002). Stage 1 HS presents with solitary or multiple isolated abscesses without scarring or sinus tracts, while stage 2 HS is characterized by scarring and sinus tract formation. Extensive, multi-region involvement with multiple interconnected sinus tracts and scarring typifies stage 3 HS. HS has a female predominance, affecting 4% of women in the general population (Freedberg et al., 1999). Patients present with deep-seated abscesses that ultimately progress to sinus tract and fistula formation with fibrosis and scarring. Extensive scarring can lead to decreased mobility, and vaginal, urethral, and anal strictures. Secondary bacterial infection with Staphylococcus, Streptococcus, Pseudomonas, and Escherichia is common and produces a foul-smelling odor. Rarely, squamous cell carcinoma can arise within the chronic wounds of HS, which behaves aggressively and may metastasize. Patients with HS often feel socially isolated and suffer severe psychological impact of their illness. http://www.medscape.com/viewarticle/503520_print Page 8 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 Pathogenesis The exact pathogenesis of HS is unknown (Katsanos et al., 2002). It was thought that HS was a dysfunction of the apocrine glands since HS targets primarily these areas of the body. However, since it has been diagnosed in association with follicular occlusion disorders, such as acne conglobata and dissecting cellulitis of the scalp, it was thought that these three conditions may share the same pathogenesis. Follicular occlusion leads to overgrowth of bacteria and subsequent neutrophilic inflammation. This inflammation ultimately progresses to involve the apocrine glands. Chronic inflammation of these structures leads to fibrosis and destruction. Other observations include the role of androgens/hormones, obesity, and genetics (Ostlere, Langtry, Mortimer, & Staughton, 1991; Tsianos, Dalekos, Tzermias, Mer kouropoulos, & Hatzis, 1995). Since HS begins after puberty, improves with pregnancy, and improves with cyclic elevations of estrogen during the menstrual cycle, these serve to support the role of hormonal influence in the pathogenesis of HS. Obesity, which negatively affects sex hormone metabolism, also plays a role in HS development. Finally, a positive family history of HS suggests a genetic component. More recently, the association of HS with Crohn's disease has been elucidated (Katsanos et al., 2002). It was then postulated that these two conditions may share the same pathogenesis with the possible involvement of similar immune mechanisms, such as the proliferation of TNFα with resultant neutrophilic chemotaxis (Katsanos et al., 2002; Tsianos et al., 1995). Person and Bernhard (1986) proposed that bowel-related skin diseases may be the result of auto-intoxication (Ostlere et al., 1991). Dysfunction of gut mucosa may lead to the failure to inactivate bacterial or dietary antigens, which would allow the formation of IgA immune complexes that ultimately deposit in the skin. Treatment Early intervention with medical management is preferred to prevent scarring, which will ultimately require surgical intervention (Freedberg et al., 1999). Daily use of antibacterial soaps or Burow's soaks should be utilized. Intralesional or systemic steroids, cyclosporin, isotretinoin, and cyproterone have been used with minimal success. Oral antibiotics often are needed on a chronic basis, and should be adjusted based on the bacterial culture sensitivities and rotated accordingly. Frequently, incision and drainage of HS abscesses with concurrent immunosuppression is needed. When patients progress to stage 3 HS, surgical intervention is necessary. This includes wide local excision of the affected areas with subsequent healing by secondary intention. CO 2 laser also may yield good results with minimal complications. Infliximab Because of the concurrent presentation of HS and Crohn's, it was postulated that these two conditions share the same pathogenesis, namely excess TNFα production (Katsanos et al., 2002; Tsianos et al., 1995). This was supported by several reports in the literature of patients with HS and Crohn's who responded to infliximab infusions (5 mg/kg) (Katsanos et al., 2002). These patients had been treated with standard im munosuppressants but remained recalcitrant until the addition of infliximab. Not only was healing rapid, but also sustained for up to 1 year (see Figures 7 & 8). http://www.medscape.com/viewarticle/503520_print Page 9 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 Figure 7. Hidradenitis suppurativa involvement in the groin, buttocks, and thighs. Figure 8. Resolution of hidradenitis suppurativa after completion of infliximab treatment. Sullivan, Welsh, Kerdel, Bur dick, and Kirsner (2003) successfully treated five patients with HS with infliximab. Three of the five patients had two infliximab infusions at 5 mg/kg, while two had one infusion at 5 mg/kg. All patients experienced improvement within 3 to 7 days. These patients were able to either stop or decrease the http://www.medscape.com/viewarticle/503520_print Page 10 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 dose of all other systemic immunosuppressants. All patients significantly improved with infliximab. Pyoderma Gangrenosum Pyoderma gangrenosum (PG) is a rare inflammatory, neutrophilic dermatosis characterized by one or many chronic ulcerations with violaceous undermined borders (Mimouni, Anhalt, Kouba, & Nousari, 2003; Triantafillidis, Cher acakis, Sklavaina, & Apostol opoulou, 2002). PG affects mainly adults, typically between the ages of 40 to 60 years and its usual course is that of recurring destructive ulcers, which begin as pustules, and resolve with cribriform scars. Several clinical variants of PG have been described, such as ulcerative, pustular, bullous, vegetative, and periostomal types. As no diagnostic test confirms a diagnosis of PG and a number of other conditions may resemble it clinically, the diagnosis of PG is often a diagnosis of exclusion. PG is associated with other conditions in up to 75% of patients, including inflammatory bowel disease (Crohn's disease or ulcerative colitis), arthritis (rheumatoid or seronegative), monoclonal gammopathy (usually IgA gammopathy), and hematologic malignancies (especially acute myelocytic leukemia) (Mimouni et al., 2003). Pathogenesis The exact pathogenesis of PG is unknown; however, it is believed that pathergy may play a role (Tan et al., 2001). Pathergy is defined as development of lesions in areas of trauma. PG lesions may result from minimal trauma or irritation to the skin, debridement, graft harvest sites, stoma placement sites, surgical wounds, and even old scars. The implication of pathergy may suggest an uncontrolled, exaggerated, altered inflammatory response to nonspecific stimuli. Further evidence proposes that there is an underlying dysfunction of the immunoregulatory and immunologic effectors in patients with PG. Various pro-inflammatory cytokines may be expressed in PG (Ljung et al., 2002; Mimouni et al., 2003). IL-8, which is chemotactic for neutrophils, is normally not detected in human skin; however, IL-8 is overproduced in PG. Laboratory studies have shown that when IL-8 is injected into human skin xenografts, which are grafted onto mice, PG-like ulcers develop. This suggests a role for IL-8 in the etiology of PG. Also, TNFα, a potent pro-inflammatory cytokine, has been implicated in the pathogenesis of Crohn's and PG (Ljung et al., 2002; Tan et al., 2001). Over expression of TNF in PG leads to recruitment of inflammatory cells, like neutrophils, to local tissue sites of inflammation. Treatment There is no specific treatment available for PG. For limited or mild disease, topical or intralesional steroids may be utilized (Tan et al., 2001). For more severe or widespread disease, a variety of systemic therapies can be used, such as systemic steroids, cyclosporin, mycophenolate mofetil, methotrexate, chlorambucil, and thalidomide. Antibiotics with anti-inflammatory properties, such as minocycline or dapsone, are often used as first-line therapies. Anecdotal reports of the use of nicotine patches and topical tacrolimus have shown promise. Infliximab Since TNFα production is involved in the pathogenesis of PG, and PG is often found in association with Crohn's disease, several patients reported in the literature were treated successfully with infliximab (Ljung et al., 2002; Mimouni et al., 2003; Tan et al., 2001; Triantafillidis et al., 2002). These patients were all treated with infliximab 5 mg/kg with remissions from 5 months to over 1 year. Patients were treated with different dosing schedules. Triantafillidis et al. (2002) and Ljung et al. (2002) gave loading doses of infliximab at weeks 0, 2, 6; however, Triantafillidis et al. repeated this loading dose subsequently depending on the status of the patient's condition. Tan et al. (2001) did not report their dosing schedule, but gave two to five infusions of infliximab. Mimouni et al. (2003) administered infliximab at weeks 0, 2, 4, 8, 10, and then every 6 to 8 weeks thereafter as needed. Results were noted within 12 to 24 hours of the infusion, with continuous improvement over the following week. Only rash and reactive arthritis were noted in two different patients, necessitating permanent suspension of their infusions. Geren, Kerdel, Falabella, and Kirsner (2003) successfully treated 13 ulcers in five patients with PG with infliximab. Three patients received one infusion of infliximab at 5 mg/kg, while two patients received three infusions at 5 mg/kg. Twelve of the 13 ulcers healed within 22.2 weeks. Therapy had to be held in one patient secondary to flushing and pruritus, which lead to nonhealing of one ulcer. However, the patient later healed on systemic steroids. Infliximab was used as monotherapy in two patients and adjuvant therapy in three patients. Other therapies used in conjunction with infliximab in these three patients included oral steroids, cyclosporin, clofazimine, and topical tacrolimus. http://www.medscape.com/viewarticle/503520_print Page 11 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 Behcet's Syndrome Behcet's syndrome (BS) is a chronic, relapsing multisystem vasculitis of unknown cause (Sfikakis, 2002). It is endemic in certain Asian and Middle Eastern countries. Criteria for diagnosis includes oral apthous ulcers occurring at least three times a year and two or more of the following: recurrent genital ulcers, skin lesions, eye findings, or positive pathergy test (Travis, Czajkowski, McGovern, Watson, & Bell, 2001). Ocular disease is the most frequent cause of morbidity, with blindness occurring in 25% of patients (Sfikakis, 2002). It affects men and women equally, and usually presents in the 2nd and 3rd decades of life. Diagnosis is based solely on clinical findings. Death may occur from neurologic involvement, bowel perforation, vasculitis, and cardiopulmonary disease. Pathogenesis While the pathogenesis of BS remains largely unknown, several theories have been offered, such as genetic, infectious, and immunologic (Freedberg et al., 1999; Sfikakis, 2002; Travis et al., 2001). Genetic predisposition has been suggested based on the link between BS and HLA-B51, and familial clustering. Extensive investigation has been unable to confirm an infectious etiology; however, homology between herpes simplex virus and lymphocyte DNA has been noted. Also, it is postulated that exposure to Streptococcus may trigger an immunologic response. Circulating immune complexes have been recovered from serum of patients with BS and correlate with disease activity (Freedberg et al., 1999). It is thought that these immune complexes trigger a neutrophilic reaction/vasculitis by binding to endothelial cells and releasing oxygen radicals and proteolytic enzymes, which cause tissue damage. Pathergy may set in motion this chain of events. Also, patients have elevated levels of T cells expressing the gamma/delta receptor, which leads to the excess production of TNFα and other Th1 cytokines (Sfikakis, 2002; Travis et al., 2001). Increased levels of TNFα and soluble TNFα receptors have been recovered from serum and vitreous humor. Treatment Treatment options for BS can be divided into two types: mucocutaneous and systemic (Freedberg et al., 1999; Sfikakis, 2002; Travis et al., 2001). Mucocutaneous disease has responded to topical and intralesional glucocorticoids, topical anesthetics, thalidomide, dapsone, interferon alpha, and colchicine. Systemic disease requires more aggressive treatment with the use of prednisone alone or in combination with cyclosporin, mycophenolate mofetil, azathioprine, cyclophosphamide, and chlorambucil. Infliximab With the recent discovery of the role of TNFα in the pathogenesis of BS, multiple reports of the benefits of infliximab have been reported in the literature (Goossens, Verburg, & Breedveld, 2001; Licata et al., 2003; MunozFernandez, Hidalgo, & Schlincker, 2001; Mussack et al., 2003; Rozenbaum, Rosner, & Portnoy, 2001; Sfikakis, Theodossiadis, Katsiari, Kaklamanis, & Markomichelakis, 2001; Travis et al., 2001; Triolo et al., 2002). Infliximab has been used successfully in treating CNS vasculitis, colonic ulcerations, esophageal ulcerations, panuveitis, mucocutaneous ulcers, and polyarthritis. Doses of 3, 5, or 10 mg/kg were dispensed. Infusions were given one to four times in a 2-month period with or without regular maintenance doses thereafter. Remission was achieved in all patients, with followup ranging from 2 months to 2 years. No significant side effects were noted during or after the infusions. Results were usually seen within the first 24 hours of the infusion. These infusions were given as adjuvants to systemic immunosuppressant therapy. The use of infliximab permitted the tapering down or off of these immunosuppressant agents, thus decreasing their side effects. Etanercept Recently, a 4-week double-blind placebo controlled study of the use of etanercept in Behcet's was completed after a 4-week washout of systemic immunosuppressants (Sfikakis, 2002). Patients with mucocutaneous lesions and arthritis were treated with etanercept 25 mg subcutaneously twice a week. Good results were seen after only the first week and were maintained throughout the study. Patients treated with etanercept had a 40% chance of remaining free of ulcers versus 5% from placebo. Another study utilized etanercept at the same dose for 6 months in patients with ocular involvement on systemic immunosuppressants. The benefits gleaned from use of etanercept were not sustained after 6 months post-treatment followup. Graft versus Host disease http://www.medscape.com/viewarticle/503520_print Page 12 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 Graft versus host disease (GVHD) is a condition which can occur after bone marrow or organ transplantation, or blood transfusion (Kobbe et al., 2001; Rivkina & Stump, 2002). The acute stage, which occurs in 75% of patients, begins within 11 to 16 days and targets the skin, gastrointestinal tract, and liver (27). Ten percent of patients develop chronic stage GVHD, which occurs after 100 days. Patients may progress to chronic stage from acute stage or de novo. This stage affects the skin, liver, salivary glands, mucosa and muscles. Pathogenesis While the exact pathogenesis is unknown, it is thought that GVHD occurs when immunologically competent donor T cells in the graft/blood attack antigens on the cells of the immunodeficient recipient (Freedberg et al., 1999; Kobbe et al., 2001; Rivkina & Stump, 2002). Various cytokines have been implicated in the pathogenesis of GVHD, such as interleukin 1, 2, 6, 12; interferon gamma, and TNFα. TNFα is released by donor T cells and leads to damage of recipient tissue. Treatment Acute GVHD is treated with systemic steroids and possibly immunosuppressants, such as cyclosporin, tacrolimus, methotrexate, and anti-thymocyte globulin (Freedberg et al., 1999). Skin manifestations may also be treated with topical steroids and PUVA. Chronic GVHD is treated similarly with systemic steroids with or without concurrent immunosuppressants, including cyclosporin, azathioprine, methotrexate, and photopheresis. PUVA, retinoids, and topical steroids may be of some use for chronic cutaneous disease. Infliximab Rivkina and Stump (2002) reported four cases of GVHD treated with infliximab at 10 mg/kg weekly for 4 to 5 weeks. One patient died from pneumonia after responding to infliximab. Another patient suffered cytomegalovirus and aspergillosis infections. Three of the four patients improved after infliximab infusions. Kobbe et al. (2001) showed success in patents with acute GVHD treated with infliximab at 10 mg/kg. Patients received one to three infusions of infliximab. Three of the four patients responded to the infliximab. Two survived free of GVHD for 292 and 275 days. One patient died from his underlying myeloma, not GVHD. Finally, one patient died from GVHD despite three infusions of infliximab. Serious infections were encountered in two patients. Couriel et al. (2000) treated 25 patients with GVHD with one to eight infusions of 10 mg/kg of infliximab. Twenty patients had acute and five had chronic GVHD. A complete response was seen in 55% of acute patients, 85% with GI, 75% with cutaneous, and 33% with liver involvement. Patients with chronic GVHD showed partial response of skin involvement in 2/4, and complete response of diarrhea in 4/4. Hicks et al. (1999) treated 16 patients with acute GVHD with infliximab 10 mg/kg for one to eight infusions. Complete response was achieved in 63% of patients with 80% having GI involvement. Other Off-Label Uses of Infliximab Patients with Sneddon-Wilkinson, a chronic superficial pustular disorder; toxic epidermal necrolysis, a rare hypersensitivity reaction to certain medications which leads to loss of the epidermis; and sarcoidosis, a systemic granulomatous disease, have been successfully treated with infliximab (Baughman, Lower, & Du Bois, 2003; Fischer, Fielder, Marsch, & Wohlrab, 2002; Mallbris, Ljungberg, Hedblad, Larsson, & Stahle- Backdahl, 2003; Voigtlander, Luftl, Schuler, & Hertl, 2001). Other Off-Label Uses of Etanercept Patients with scleroderma, an inflammatory disease characterized by systemic sclerosis; cicatricial pemphigoid, a chronic autoimmune blistering disease; histiocytosis X, a systemic disease characterized by infiltration with Langerhans cells; and Wegenergranulomatosis, an autoimmune granulomatous vasculitic disease, have been successfully treated with etanercept (Henter et al., 2001; Sacher et al., 2002; Sapadin & Fleischmajer, 2002; Stokes & Kremer, 2003; Tutuncu, Morgan, & Kavanaugh, 2002). Conclusion Recent advances in the understanding of the pathogenesis of psoriasis, psoriatic arthritis, hidradenitis suppurativa, http://www.medscape.com/viewarticle/503520_print Page 13 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 pyoderma gangrenosum, Behcets, and graft versus host disease have led to the development of revolutionary antiTNFα biologic therapies, which target this cytokine. Various other diseases may also benefit from these agents. While the efficacy of these agents has proven impressive and short-term side effects have been few and relatively benign, the long-term side effects have not been studied since these drugs are new to the scene. Further trials are needed to assess effects of prolonged use. Longer, controlled trials are also required to verify the efficacy in lesscommon diseases. However, this should not dissuade clinicians from adding these novel agents to their armamentarium. CE Information The print version of this journal was orginally certified for CE credit. For accreditation details please contact the publisher, Jannetti Publications,Inc.; East Holly Avenue Box 56; Pittman, NJ 08071. References Baughman, R.P., Lower, E.E., & Du Bois, R.M. (2003). Sarcoidosis. Lancet, 361 (9363), 1111-1118. Chaudhari, U., Romano, P., Mulcahy, L.D., Dooley, L.T., Baker, D.G., & Gottleib, A.B. (2001). Efficacy and safety of infliximab monotherapy for plaque-type psoriasis: A randomized trial. Lancet, 357 (9271), 18421847. Couriel, D., Hicks, K., Ippoliti, C., et al. (May, 2000) Infliximab for the treatment of graft versus host disease in allogeneic transplant recipients . Paper presented at 36th Annual Meeting of the American Society of Clinical Oncology, New Orleans, LA. Davison, S.C., Bunker, C.B., & Basarab, T. (2002). Etanercept for severe psoriasis and psoriatic arthritis: Observations on combination therapy. British Journal of Dermatology, 147 (4), 831-832. Elewski, B.E. (2002) Infliximab for the treatment of severe pustular psoriasis. Journal of the American Academy of Dermatology, 47 (5), 796-797. Fischer, M., Fiedler, E., Marsch, W.C., & Wohlrab, J. (2002). Antitumour necrosis factor alpha antibodies (infliximab) in the treatment of a patient with toxic epidermal necrolysis. British Journal of Dermatology, 146 (4), 707-708. Freedberg, I.M., Eisen, A.Z., Wolff, K., Austen, K.F., Goldsmith, L.A., Katz, S.I., et al. (1999). Fitzpatrick's dermatology in general medicine . New York: McGraw-Hill Co. Galadari, H., Fuchs, B., & Lebwohl, M. (2003). Newly available treatments for psoriatic arthritis and their impact on skin psoriasis. International Journal of Dermatology, 42 (3), 231-237. Geren, S.M., Kerdel, F.A., Falabella, A.F., & Kirsner, R.S. (2003). Infliximab: A treatment option for ulcerative pyoderma gangrenosum. Wounds, 15 , 49-53. Goffe, B., & Cather, J.C. (2003). Etanercept: An overview. Journal of the American Academy of Dermatology, 49 (2 Suppl.) S105-S111. Goossens, P.H., Verburg, R.J., & Breedveld, F.C. (2001). Remission of Behcet's syndrome with tumour necrosis factor alpha blocking therapy. Annals of the Rheumatic Diseases, 60 (6), 637. Gottlieb, A.B. (2001). Psoriasis: Im munopathology and immunomodulation. Dermatologic Clinics, 19 (4), 649- 657. Gottlieb, A.B., & Bos, J.D. (2002). Recombinantly engineered human proteins: Transforming the treatment of psoriasis. Clinical Immunology, 105 (2), 105-116. Gottleib, A.B., Chaudhari, U., Mulcahy, L.D., Dooley, L.T., & Baker, D.G. (2003). Infliximab monotherapy provides rapid and sustained benefit for plaque-type psoriasis. Journal of the American Academy of Dermatology, 48 (6), 829-835. Gottleib, A.B., Matheson, R.T., Lowe, N.J., & Zitnik, R.J. (2002). Efficacy of etanercept in patients with psoriasis. Journal of Investigative Dermatology, 119 , 234. Henter, J., Karlen, J., Calming, U., Bernstand, C., Andersson, U., & Fadeel, B. (2001). Successful treatment of Langerhan-cell histiocytosis with Etanercept. New England Journal of Medicine, 345 (21), 1577-1578. Hicks, K., Ippoliti, C., Donato, M., et al. (1999, December). Infliximab for the treatment of steroid refractory graft versus host disease in allogeneic transplant recipients . Paper presented at American Society of Hematology Annual Meeting, New Orleans, LA. Iyer, S., Yamauchi, P., & Lowe, N.J. (2002). Etanercept for severe psoriasis and psoriatic arthritis: Observations on combination therapy. British Journal of Dermatology, 146 (1), 118-121. Katsanos, K.H., Christodoulou, D.K., & Tsianos, E.V. (2002). Axillary hidradenitis suppurativa successfully treated with infliximab in a Crohn's disease patient. American Journal of Gastroenterology, 97 (8), 21552156. Keane, J., Gershon, S., Wise, R.P., Mirabile-Levens, E., Kasznica, J., Schwieterman, W.D., et al. (2001). Tuberculosis associated with infliximab, a tumor necrosis factor alpha-neutralizing agent. New England http://www.medscape.com/viewarticle/503520_print Page 14 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 Journal of Medicine, 345 (15), 1098-1104. Kobbe, G., Schneider, P., Rohr, U., Fenk, R., Neumann, F., Aivado, M., et al. (2001). Treatment of severe steroid refractory acute graft versus host disease with infliximab, a chimeric human/mouse anti-TNFα antibody. Bone Marrow Transplantation, 28 (1), 47-49. Kurschat, P., Rubbert, A., Poswig, A., Scharffetter-Kochanek, K., Kreig, T., & Hunzelmann, N. (2001). Treatment of psoriatic arthritis with etanercept. Journal of the American Academy of Dermatology, 44 (6), 1052. LaDuca, J.R., & Gaspari, A.A. (2001). Targeting tumor necrosis factor alpha. Dermatologic Clinics, 19 (4), 617- 635. Lebwohl, M. (2003). Psoriasis. Lancet, 361 (9364), 197-1204. Licata, G., Pinto, A., Tuttolomondo, A., Banco, A., Ciccia, F., Ferrante, A., et al. (2003). Anti-tumour necrosis factor alpha monoclonal antibody therapy for recalcitrant cerebral vasculitis in a patient with Behcet's syndrome. Annals of the Rheumatic Diseases, 62 (2), 280-281. Ljung, T., Staun, M., Grove, O., Fausa, O., Vatn, M.H., & Hellstrom, P.M. (2002). Pyoderma gangrenosum associated with Crohn disease: Effect of TNFα blockade with infliximab. Scandinavian Journal of Gastro enterology, 37 (9), 1108-1110. Mallbris, L., Ljungberg, A., Hedblad, M.A., Larsson, P., & Stahle-Backdahl, M. (2003). Progressive cutaneous sarcoidosis responding to anti-tumor necrosis factor alpha therapy. Journal of the American Academy of Dermatology, 48 (2), 290-293. Mease, P.J. (2002). Tumour necrosis factor (TNF) in psoriatic arthritis: Pathophysiology and treatment with TNF inhibitors. Annals of Rheumatic Diseases, 61 (4), 298-304. Mease, P.J., Goffe, B.S., Metz, J., VanderStoep, A., Finck, B., & Burge, D.J. (2000a). Etanercept in the treatment of psoriatic arthritis and psoriasis: A randomized trial. Lancet, 356 (9227), 385-390. Mease, P.J., Goffe, B.S., & Metz J. (2000b). Enbrel ® (Etanercept) in patients with psoriatic arthritis and psoriasis. Arthritis and Rheumatism, 43 , S403. Mimouni, D., Anhalt, G.J., Kouba, D.J., & Nousari, H.C. (2003). Infliximab for peristomal pyoderma gangrenosum. British Journal of Dermatology, 148 (4), 813-816. Munoz-Fernandez, S., Hidalgo, V., & Schlincker, A. (2001). Effect of infliximab on threatening panuveitis in Behcet's disease. Lancet, 358 (9293), 1644. Mussack, T., Landauer, N., Ladurner, R., Schiemann, U., Goetzberger, M., Burchardi, C., et al. (2003). Successful treatment of cervical esophageal perforation in Behcet's disease with drainage operation and infliximab. American Journal of Gastroenterology, 98 (3), 703-704. Newland, M.R., Weinstein, A., & Kerdel, F.A. (2002). Rapid response to infliximab in severe pustular psoriasis, von Zumbusch type. International Journal of Dermatology, 41 (7), 449-452. Ostlere, L.S., Langtry, J.A.A., Mortimer, P.S., & Staughton, R.C.D. (1991). Hidradenitis suppurativa in Crohn's disease. British Journal of Dermatology,125 (4), 384-386. Person, J.R., & Bernhard, J.D. (1986). Autointoxication revisited. Journal of the American Academy of Dermatology, 15 (3), 559-563. Provenzano, G., Termini, A., Le Moli, C., & Rinaldi, F. (2003). Efficacy of infliximab in psoriatic arthritis resistant to treatment with disease modifying antirheumatic drugs: An open pilot study. Annals of Rheumatic Diseases, 62 (7), 680-681. Rivkina, A.M., & Stump, L.S. (2002). Infliximab in graft versus host disease. American Journal of HealthSystem Pharmacy, 59 , 1271-1275. Rozenbaum, M., Rosner, I., & Portnoy, E. (2001). Remission of Behcet's syndrome with TNFα blocking treatment. Annals of Rheumatic Diseases, 61 (3), 283-284. Sacher, C., Rubbert, A., Konig, C., Scharffetter-Kochanek, K., Krieg, T., & Hunzelmann, N. (2002). Treatment of recalcitrant cicatricial pemphigoid with the tumor necrosis factor alpha antagonist etanercept. Journal of the American Academy of Dermatology, 46 (1), 113-115. Sapadin, A.N., & Fleischmajer, R. (2002). Treatment of scleroderma. Archives of Dermatology, 138 (1), 99105. Sfikakis, P.P. (2002). Behcet's disease: A new target for anti-tumour necrosis factor treatment. Annals of the Rheumatic Diseases, 61 (Suppl. 2), ii51-ii53. Sfikakis, P.P., Theodossiadis, P.G., Katsiari, C.G., Kaklamanis, P., & Markomichelakis, N.N. (2001). Effect of infliximab on sight-threatening panuveitis in Behcet's disease. Lancet, 358 (9278), 295-296. Smith, K.J., & Skelton, H.G. (2001). Rapid onset of cutaneous squamous cell carcinoma in patients with rheumatoid arthritis after starting tumor necrosis factor alpha receptor IGG1-FC fusion complex therapy. Journal of the American Academy of Dermatology , 45 (6), 953-956. Stokes, D.G., & Kremer, J.M. (2003). Potential of TNF neutralizing strategies in rheumatolgic diseases other than rheumatoid arthritis. Seminars in Arthritis and Rheumatism, 33 (1), 1-18. Sullivan, T.P., Welsh, E., Kerdel, F.A., Burdick, A.E., & Kirsner, R.S. (2003). Infliximab for hidradenitis suppurativa. British Journal of Dermatology, 149 (5), 1046-1049. http://www.medscape.com/viewarticle/503520_print Page 15 sur 16 Tumor Necrosis Factor Alpha Inhibitors for Dermatologic Diseases 075/03/Thursday 08h54 Tan, M.H., Gordon, M., Lebwohl, O., George, J., & Lebwohl, M.G. (2001). Improvement of pyoderma gangrenosum and psoriasis associated with Crohn disease with anti-tumor necrosis factor alpha monoclonal antibody. Archives of Dermatology, 137 (7), 930-933. Travis, S.P.L., Czajkowski, M., McGovern, D.P.B., Watson, R.G.P., & Bell, A.L. (2001). Treatment of intestinal Behcet's syndrome with chimeric tumour necrosis factor alpha antibody. Gut, 49 (5), 725-728. Triantafillidis, J.K., Cheracakis, P., Sklavaina, M., & Apostolopoulou, K.A. (2002). Favorable reponse to infliximab treatment in a patient with active Crohn disease and pyoderma gangrenosum. Scandinavian Journal of Gastroenterology, 37 (7), 863-865. Triolo, G., Vadala, M., Accardo-Palumbo, A., Ferrante, A., Ciccia, F., Giardina, E., et al. (2002). Anti-tumour necrosis factor monoclonal antibody treatment for ocular Behcet's disease. Annals of the Rheumatic Diseases, 61 (6), 560-561. Tsianos, E.V., Dalekos, G.N., Tzermias, C., Merkouropoulos, M., & Hatzis, J. (1995). Hidradenitis suppurativa in Crohn's disease. Journal of Clinical Gastroenterology, 20 (2), 151-153. Tutuncu, Z., Morgan, G.J., & Kavanaugh, A. (2002). Anti-TNF therapy for other inflammatory conditions. Clinical and Experimental Rheuma tology, 20 (6 Suppl. 28), S146-S151. Van Den Bosch, F., Kruithof, E., Baeten, D., De Keyser, F., Mielants, H., & Veys, E.M. (2000). Effects of a loading dose regimen of three infusions of chimeric monoclonal antibody to tumour necrosis factor alpha (infliximab) in spondyloarthropathy: An open pilot study. Annals of Rheumatic Diseases, 59 (6), 428-433. Victor, F.C., & Gottlieb, A.B. (2002). TNF alpha and apoptosis: Implications for the pathogenesis and treatment of psoriasis. Journal of Drugs in Dermatology, 3 (1), 264-275. Voigtlander, C., Luftl, M., Schuler, G., & Hertl, M. (2001). Infliximab: A novel highly effective treatment of recalcitrant subcorneal pustular dermatosis (Sneddon-Wilkinson disease). Archives of Dermatology, 137 (12), 1571-1574. Weinblatt, M.E., Keystone, E.C., Furst, D.E., Moreland, L.W., Weisman, M.H., Birbara, C.A., et al. (2003). Adalimumab, a fully humanized anti-tumor necrosis factor alpha monoclonal antibody, for the treatment of rheumatoid arthritis in patients taking concomitant methotrexate: The ARMADA trial. Arthritis and Rheumatism, 48 (1), 35-45. Williams, J.D.L., & Griffiths, C.E.M. (2002). Cytokine blocking agents in dermatology. Clinical and Experi mental Dermatology, 27 (7), 585-590. Jennifer T. Trent , MD , is a Resident, Department of Dermatology and Cutaneous Surgery, University of Miami School of Medicine, Miami, FL. Francisco A. Kerdel , MBBS, BSc, is Chief, Dermatology and Director, Inpatient Dermatology Service, Cedars Medical Center, Miami, FL. http://www.medscape.com/viewarticle/503520_print Page 16 sur 16