Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
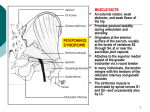
That nagging pain in the bum! What do we really know about piriformis muscle and how can it help us with exercise prescription. Brief History of Anatomy To understand a healthy, diseased or dysfunctional human body, a multidisciplinary approach to anatomical study is essential. It is not only crucial to understand the birth of the body’s unique single cells and their journey of development in to specific structures and systems but how they may relate to one another synergistically is vital. Mankind’s curiosity with the human body started as early as 380 BC with Hipprocrates. Although their knowledge was scant and their procedures were often crude by modern standards, Hippocrates the ‘father of medicine’ and other Greek physicians established the foundations that are the basis for the study and treatment of mankind as we know it today (Whiting & Zernicke, 2008). It must be recognised that their breakthroughs were extraordinary, albeit niave compared with our current understanding. Then came the fifteen hundreds when Vesalius promoted the practice of focusing on what was discovered at the time and not taking previous anatomical literature verbatim. With man’s interest in anatomical study growing day by day, acknowledging there is still so much to know about disease and dysfunction, clinical advancements in the diagnostics and treatment of the human body show no sign of slowing. It is imperative at this point that we appreciate that not all diagnostics are one hundred percent accurate and each have their own limitations to anatomical study. These flaws will be discussed further in this study. This study will be looking at investigating descriptive epidemiological studies; case studies and the distribution of disease or dysfunction, and analytical research that deals with the incidence, distribution and control of disease in a population: questioning the research strategies that reveal contributing factors of disease or dysfunction. Both will be examining numerous perspectives within the medical arena. The piriformis muscle is a central pillar to biomechanical dysfunction; research has shown that when it’s dysfunctional, not only can the pelvis be taken out of alignment but it can also affect the functional performance of the upper and lower limbs. Understanding the piriformis muscle and all its anomalies is imperative to understanding an individual’s needs and avoiding generalization. It is therefore the individual’s function that is interesting and if dysfunctional, then a common sense approach of different arenas would command the best method to rid the problems. Research studies of anatomical observations, imaging, functional screens, manual treatment will be examined throughout this paper. In the Sixteenth Century an Italian Professor at Padua, Spigelius, was the first anatomist to name the piriformis muscle. The piriformis muscle is one of six deep small hip external rotators. It is uppermost to the gluteal muscle group and imperative to the arrangement of the vessels and nerves in the buttocks. Key to understanding this muscle we must first become orientated with its anatomical features and functions; then later we shall be examining the literature with regards to the variety of its form and structure histology and the significant implications these have. The piriformis muscle largely fills the greater sciatic foramen, through which the branches of the sacral plexus and branches of the internal iliac vessels to the gluteal and pudendal regions leave the pelvis; therefore, the vessels and nerves that enter the buttock necessarily are closely related to this muscle (Williams 1999). The piriformis is a voluntary muscle, innervated by motor neurons whose cell bodies lie within the central nervous systems and whose axons extend peripherally to the muscles. It is pyramidal in shape whose muscle fibres run in a straight line from the origin to the insertion in the same plane as gluteus medius. Its proximal attachment starts at the anterior aspect of the second to fourth sacral segments and extends between the lateral to the anterior sacral formina – see figure 1. From its additional attachment on the gluteal surface of the ilium, near the posterior inferior iliac spine, and the pelvic surface of the sacrotuberous ligament it then feeds out of the pelvis through the greater sciatic foramen. Bouisson arcade is a lower convex fibrous arcade stretched from the anterior edge of the greater sciatic notch to the sacroiliac joint, immediately above the upper edge of the piriformis muscle (Paturet,1951). Its fibres continue downwards laterally and forwards narrowing into a rounded tendon to attach to the medial side of the greater trochanter of the femur. The innervation of the piriformis muscle comes from the piriformis nerve, from the sacral plexus L5, S2, but mainly S1. (Palastanga et al, 2006). It leaves the pelvis through the greater sciatic foramen and below through or above the piriformis muscle before extending distally between the greater tuberosity of the femur and the ischial tuberosity of the pelvis into the lower extremity. The Arterial Supply comes from the superior and inferior gluteal artery along with the lateral sacral artery. Most sciatic nerves lie inferior and posterior to the piriformis and bifurcate into common peroneal (fibular) and tibial nerves outside of the pelvis. The piriformis muscle has a unique, albeit very assorted, relationship with the sciatic nerve which is discussed later. Understanding the complete, although varied, anatomical relationship that the sciatic nerve has on the piriformis muscle may have a clinical importance in the cause and development of disease will lead to a superior management of sciatica. However, it is important to note that as far back as 1900’s the action and function of the piriformis muscle has been under much debate as has its anatomy. What does piriformis do? A considerable quantity of literature observes the action of the piriformis muscle from an anatomical position or in a seated upright position with hip flexion close to 90 degrees. In an anatomical position piriformis muscle is a lateral rotator, whilst in a seated position it assists in abduction at the hip. The additional action of the piriformis muscle is to stabilise the head of the femur in to the acetabulum whilst the superficial pelvic muscles perform their action. Cael (2009) observes that if there is excessive contraction of the piriformis muscle causing posterior tilt of the pelvis and external rotation of the hip then excessive lengthening leading to anterior tilt of the pelvis, hip adduction and hip medial rotation is inevitable. However, it is also important to consider that this may only be true if the surrounding musculoskeletal systems are also dysfunctional. It is important to consider that the piriformis muscles’ functional capacity depends upon the position of the hip joint with respect to flexion, extension, adduction and abduction. Gaining the correct knowledge and full understanding of the biomechanics and anatomical anomalies of the piriformis will we then be able to provide the therapist/physician/Biomechanics Coach with a superior management of dysfunction and disease and possibly the prevention of future injury. Understanding the various anomalies within the hip joint region would be of great advantage during surgical procedures and for post-operative management. Kapandji (1970b) and Steindler (1977) took investigative biomechanics and kinesiology of the pelvis to another level when they observed the piriformis muscle changes from an external rotator in hip extension to an internal rotator in hip flexion. Biomechanics Coaches today have embraced this understanding and use it successfully in the management programmes of hypertonic piriformis muscles. In most cases the distinction between disease and injury is clear, however there are times when these two distinctions crossover i.e. Osteoporosis can cause bone fractures (Whiting & Zernicke, 2008). What affect can it have on the sciatic nerve? Cael (2009) observed tightness in piriformis may compress the sciatic nerve, causing radiating pain, weakness, and altered sensation in the lower extremity. This mimics the symptoms of nerve root compression associated with a protruding intervertebral disc or degenerative changes in the spine. These factors are known as ‘risk factors’ and are classified as Intrinsic or Extrinsic factors. Intrinsic risk factors are characteristics of a biomechanical, biological or psychological nature that may predispose and individual to the disease or injury. Extrinsic risk factors are the external or environmental characteristics that influence a person’s injury risk. Intrinsic risk factors are thought to predispose an individual to injury, and once a person is susceptible, extrinsic or ‘enabling’ factors may interact with predisposing factors to increase the likelihood of injury (Meeuwisse, 1994). Many clinical studies are investigating the positional relationships between the piriformis muscle and the nerves within this area. Russell et al, (2008) set an objective to evaluate the relationship of the sacral nerve roots in relation to the piriformis muscle. It’s interesting to note that although most literature teaches most of piriformis innervations is from S1, there are however anomalies to this. Magnetic Resonance Imaging (MRI) was used on patients who had no history or clinical suspicion of piriformis syndrome. Anatomical Variations in piriformis Windisch et al (2007) conducted a cadaveric study investigating lumbosacral and buttock pain in patients history where piriformis muscle was the contributing factor to the pain. The main focus of the study was to detail the form and structure of the piriformis muscle with a particular interest in the shape and the musculotendinous junction. Emphasis throughout this study was given to specific detail of piriformis tendon diameter, insertion and its fusion with adjacent tendons. The etiology and the clinical manifestation of piriformis syndrome have been examined and reviewed. Certain cadavers were removed from the study due to the malformation of bones or tears in the piriformis muscle. The action of piriformis muscle and it’s relationship with the sciatic nerve varies considerably. The fusion of these different tendons can be explained by the development of the limb, taking place over a 5-week period from the fourth to the eighth weeks. During the fifth week, the primary germ layers of an embryo invades the limb bud and forms two large condensations, one dorsal to the axis resembling a column and one ventral to it. The dorsal muscle mass (gluteus group, piriformis) gives rise in general to the extensors and abductors of the lower limb, whereas the ventral mass gives rise to the flexors and adductors (obturator internus, gemellus superior and inferior). The piriformis spreads out from the dorsal aspect of the pelvis through the greater sciatic foramen to reach the inner side of the sacrum. Consider techniques used in Sports Massage such as trigger point technique. Testut (1884) describes the ‘Type’ variants of the relationship between the piriformis muscle and the sciatic nerve in their books about anatomical abnormalities in humans. Does size matter? Grimaldi et al, (2009) investigated the changes that occur in the deep abductor muscles in association with differing stages of unilateral degenerative hip joint pathology. The chosen method was cross sectional MRI eliciting muscle morphology from the study as they believed this is not the most accurate tool for this purpose. The study summarised the findings with no significant change in the piriformis muscle volume of the affected legs of the diseased group compared to the healthy legs of the controlled group; however they found an increase of muscle volume in the piriformis muscle of the unaffected leg. Although the study found an increase in muscle volume they have not identified whether the piriformis muscle is hypertrophied or hypertonic. According to Donofrio et al (1988) relevant to the biomechanical conditions, an increase in piriformis muscle tension, due to dysfunction of the pelvis, causes the form and structure of the piriformis muscle. Therefore, is size of piriformis important or just academic? It would be important to distinguish the difference of these findings as the management of a hypertonic muscle would be completely different to the treatment of a hypertrophied muscle, if at all. Ratnatunga et al (2010) summarised from their findings that posttraumatic spasm and contracture of the piriformis is thought to be the usual cause of piriformis syndrome. Jiri Dorvak who is a professor of neurology and is the FIFA Chief Medical Officer has established that a muscle relaxes maximally after it has been contracted sub-maximally and for a prolonged period, providing the muscle with the capacity to relax. Papadopoulos et al. (1990) states that intrinsic pathology of the piriformis muscle (e.g. myofascial pain, anatomic variations, and myositis ossificans) as primary piriformis syndrome, and all other aetiology as secondary. Difficulties arise when the identification of risk factors because in most situations, factors act in concert, and injury or disease is a result of this interaction Diop (2002) has shown in his study an increase in muscle volume of the piriformis may cause sciatic pain. The treatment plan to relieve the pressure on the nerve was cutting of the piriformis muscle. However, is it the increased volume of the piriformis muscle or the dysfunctional pelvis that may be causing this? Therefore, if the cause of sciatic pain is by a dysfunctional pelvis, by cutting the piriformis muscle are we likely to eliminate the pain? Piriformis Syndrome Recent literature has linked much of the anatomical relationship of the sciatic nerve and piriformis muscle as contributing factors to piriformis syndrome and a disputed cause of very low back or buttock pain since the idea was first postulated by Yeoman, 1928. Since then, present day included, the piriformis muscle has been quite a celebrity when it comes to understanding the cause’s piriformis syndrome. Many researchers have made impressive attempts to find the most accurate diagnosis of piriformis syndrome, with a superior management programme for recovery. Freiburg and Vinke (1934) considered the negative behaviour of the piriformis muscle and its fascia might be due to inflammation of the sacro-iliac joint or the overlying lumbosacral plexus. Four million years ago the body was built for hunting and gathering, however, for the past 100 years we have been sitting. These daily movement patterns are far from our original design and possibly creating the piriformis to be more active than the original design was for as it has not had time to adapt given the relatively short period of time over which these daily tasks have evolved. “Human evolution has been outpaced by the industrial revolution”. It is not, therefore, surprising that strain of this muscle is quite common, but unfortunately quite overlooked. (Palastanga et al, 2006). Management Guvencer et al (2008) used cadaveric study to investigate what occurs between the piriformis muscle and sciatic nerve after a functional screen. The embalming method was not discussed within this paper, however, through the process of embalming the malleability of human tissue becomes more rigid therefore the question arises of the internal and external validity of this study. Post piriformis stretch showed there was a significant stenosis of the notch by volume increase or hypertrophy of the piriformis muscle; this will consequently compress the sciatic nerve. The question remains as to the credibility of this work on cadavers and its relevance to a functional unit. If it was a live subject then although there is little evidence to support stretching for a tight muscle, anecdotally subjects seem to feel better initially, but then their stiffness or tightness often recurs after a short period of time. If this evidence from Guvencer is to be considered relevant then this may explain why the problems persist post stretching of a muscle, and perhaps we can theorize that any short term benefits which may be merely proprioceptive bombardment. Furthermore the work by Dorvak and many others has shown that stretching is not the management of choice for a muscle that is hyperactive which throws further doubt on the relevance of this piece of work. A manual therapy practice is either of the Beatty, Pace, and Frieburg manouvers stretch of the piriformis muscle in isolation. Work by Dorvak and many others has shown that a low grade contraction of a muscle that is in spasm or is hyperactive improves its capacity to relax. If this so-called piriformis syndrome is due to piriformis hyperactivity, the stretching management for this condition may be one that becomes less popular. What came first is irrelevant, it’s the individual presentation that is the key feature into understanding the various morphological symptoms. These anomalies and understandings are important in all arenas of clinical and therapy work. Examination and management methods should consider the response of muscles of the abductor synergy and function to joint pathology and note; it is not homogenous between muscles or across stages of pathology. The gluteal region is also a common area for intramuscular injections of medication which may endanger the vast variables of the neurovascular complex within this area. From the results above we have to question why most trigger point techniques and massage literature distinguishes the lateral third nearest the insertion is the best place to palpate piriformis muscle. it would be interesting to see the results from a piece of work looking at performing trigger points in the distal 1/3 of the ‘tendon’ versus the proximal 1/3. If piriformis muscle size increase is the cause of non discogenic sciatic and low back pain, and we know sub maximal contraction of a muscle that is hypertonic releases the ‘grip’ of the muscle back to a normal state; then is this all that is necessary to reduce such symptoms that all to often are treated aggressively? Conclusion This paper has probably stimulated more questions than it has provided answers with the need for further research in to the true understanding of the piriformis muscle; action, function, healthy and dysfunctional. Without this research Piriformis syndrome will remain a controversial and nebulous diagnosis. There are no studies reporting an established pathology in enough patients to satisfactorily validate the existence of piriformis pathology and anatomical causes of piriformis syndrome are rare. From a biomechanical perspective it would be interesting also to research other factors that may cause piriformis loading. It has been postulated that a number of other dysfunctions can cause piriformis problems and therefore pelvic dysfunction, such as; upper limb and neural tension, spinal stiffness, muscle spasm in quadratus lumborum, infraspinatus and others as well as muscle weaknesses. Research into these and other areas will provide more information to enable an objective view on the role and function of piriformis and hopefully provide a means by which Biomechanics Coaches and therapists can manage and prevent issues with this muscle and its associated structures.