Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
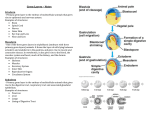
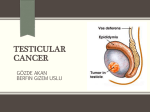
MEDICAL POLICY For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS ALPHA FETOPROTEIN (AFP) Policy Number: CMP - 014 Effective Date: January 21, 2017 Table of Contents BACKGROUND POLICY REFERENCES POLICY HISTORY/REVISION HISTORY Page 1 3 4 5 INSTRUCTIONS FOR USE This Medical Policy provides assistance in interpreting UnitedHealthcare benefit plans. When deciding coverage, the enrollee specific document must be referenced. The terms of an enrollee's document (e.g., Certificate of Coverage (COC) or Summary Plan Description (SPD)) may differ greatly. In the event of a conflict, the enrollee's specific benefit document supersedes this Medical Policy. All reviewers must first identify enrollee eligibility, any federal or state regulatory requirements and the plan benefit coverage prior to use of this Medical Policy. Other Policies and Coverage Determination Guidelines may apply. UnitedHealthcare reserves the right, in its sole discretion, to modify its Policies and Guidelines as necessary. This Medical Policy is provided for informational purposes. It does not constitute medical advice. UnitedHealthcare may also use tools developed by third parties, such as the MCG™ Care Guidelines, to assist us in administering health benefits. The MCG™ Care Guidelines are intended to be used in connection with the independent professional medical judgment of a qualified health care provider and do not constitute the practice of medicine or medical advice. BACKGROUND Alpha fetoprotein (AFP), a glycoprotein antigen, is a normally produced by a developing fetus. AFP levels begin to decrease soon after birth and are usually undetectable in the blood of healthy adults, except during pregnancy. Maternal serum screening is a noninvasive way to identify pregnancies at high risk for fetal chromosomal and structural abnormalities in the first or second trimester in pregnancy. Clinical use of maternal serum screening to evaluate risk of fetal abnormalities began in the 1970s, when high maternal serum AFP levels were shown to be correlated with increased risk of open spina bifida (OSB). In addition to maternal serum screening, an elevated level of AFP serves as a non-specific tumor associated antigen and strongly suggests the presence of either primary liver cancer, or germ cell cancer of the ovary or Proprietary Information of UnitedHealthcare. Copyright 2015 United HealthCare Services, Inc. Page 1 CMP-014_Alpha Fetoprotein_20170121_v2.2 testicle. It is generally accepted that serial measurements of AFP are performed to diagnose germ cell tumors in patients with adenocarcinoma, or carcinoma not otherwise specified, involving mediastinal nodes; or the diagnosis and monitoring of hepatocellular carcinoma (e.g., before considering liver transplantation). Additionally, serial measurements of AFP and HCG together are used to diagnose and monitor testicular cancer and some germ cell tumors of the ovary. Pregnancy Screening The current guidelines for clinical use of maternal serum screening are from the American College of Obstetricians and Gynecologists (ACOG). In 2007, ACOG recommended first trimester, integrated, or sequential screening to identify pregnancies at increased risk of Down syndrome if the patient presents in the first trimester. For women who present after first trimester for screening, ACOG recommends Quadruple Marker screening. The Quadruple Marker Screen or “Quad” screen is available for women who present between 15 and 20 weeks gestation. It combines measurements of maternal serum AFP, human chorionic gonadotropin (HCG), dimeric inhibin A (DIA), and unconjugated estriol (uE3) with maternal age risk. Low maternal serum AFP, in the second trimester, is correlated with increased risk of Down syndrome and trisomy 18, and high maternal serum AFP is correlated with increased risk of OSB. Hepatocellular Cancer (Liver Cancer) Serum AFP is the most widely used tumor marker for detecting patients with liver cancer. Liver cancers can cause elevated levels of AFP. As AFP is an established test for the diagnosis and monitoring, it is used as a screening tool to rule out the presence of a liver neoplasm before liver transplantation. This is especially pertinent in cases (such as alcoholic cirrhosis, cirrhosis of viral etiology, hemochromatosis, and alpha 1antitrypsin deficiency) where there is an increased risk of developing a primary liver tumor. AFP can also be used to help figure out the best treatment for liver cancer and to follow patients after curative surgery or other treatment. Liver cancer is not very common in the US, so AFP testing is not used as a general population screening test. Screening with AFP has been successful in parts of Asia where liver cancer is common. Germ Cell Tumors AFP is also elevated in certain germ cell tumors, such as some testicular cancers (those containing embryonal cell and endodermal sinus types), certain rare types of ovarian cancer (yolk sac tumor or mixed germ cell cancer), and germ cell tumors that start in the chest (mediastinal germ cell tumors). Most testicular cancers are germ cell tumors. For treatment planning, germ cell tumors are broadly divided into seminomas and nonseminomas because they have different prognostic and treatment algorithms. Nonseminomas include embryonal carcinomas, teratomas, yolk sac tumors, and choriocarcinomas. Human chorionic gonadotropin (HCG) is almost always elevated and AFP is never elevated in choriocarcinoma, however AFP, but not HCG, is elevated in yolk sac tumor or endodermal sinus tumor. However, many tumors are made up of a mixture of different types of non-seminoma and elevation of serum AFP is seen in 40% to 60% of men with non-seminomas. About 10% of men with testicular cancer will have a seminoma, which will have elevated HCG, but will not have elevated AFP as seminomas do not produce AFP. Proprietary Information of UnitedHealthcare. Copyright 2015 United HealthCare Services, Inc. Page 2 CMP-014_Alpha Fetoprotein_20170121_v2.2 Accepted guidelines provide that AFP and HCG measurements are valuable for determining prognosis and monitoring therapy in patients with non-seminomatous germ cell cancer and should be measured prior to removing the involved testicle. For patients with non-seminomas, the degree of tumor-marker elevation after the cancerous testicular has been removed is one of the most significant predictors of prognosis. Because of the low incidence of elevated AFP and HCG levels in early stage cancer, these markers have little value in screening for testicular cancer. Extragonadal germ cell tumors form from developing sperm or egg cells that travel from the gonads to other parts of the body. These tumors may begin to grow anywhere in the body but usually begin in organs such as the pineal gland in the brain, in the mediastinum, or in the abdomen. Extragonadal germ cell tumors can be benign (noncancer) or malignant (cancer). Malignant extragonadal germ cell tumors are divided into two types, non-seminoma and seminoma. Non-seminomas tend to grow and spread more quickly than seminomas. They usually are large and cause symptoms. If untreated, malignant extragonadal germ cell tumors may spread to the lungs, lymph nodes, bones, liver, or other parts of the body. Possible signs of extragonadal germ cell tumors include chest pain and breathing problems. AFP has been used as a screening modality for germ cell tumors when an adnexal mass in discovered in a premenopausal gynecologic patient. It is also used to follow female patients after removal of a germ cell tumor of the ovary such as immature teratomas and endodermal sinus tumors. POLICY For the following CPT code(s) in Table 1, the patient should have a diagnosis (ICD-10-CM) code(s) listed in the attached files below. Table 1. HCPCS Codes (Alphanumeric, CPT AMA) HCPCS Code 82105 Description Alpha-fetoprotein; serum ICD-10 Diagnosis Codes (Proven) CMP-014 Alpha Fetoprotein ICD10 v2.2 Proprietary Information of UnitedHealthcare. Copyright 2015 United HealthCare Services, Inc. Page 3 CMP-014_Alpha Fetoprotein_20170121_v2.2 REFERENCES 1. Bigbee W, Herberman RB. Tumor markers and immunodiagnosis. In: Bast RC Jr., Kufe DW, Pollock RE, et al., editors. Cancer Medicine. 6th ed. Hamilton, Ontario, Canada: BC Decker Inc., 2003. 2. National Cancer Institute Fact Sheet. Tumor Markers. Available at: http://www.cancer.gov/cancertopics/factsheet/detection/tumor-markers (Accessed: January 3, 2012) 3. American Cancer Society Fact Sheet. Tumor Markers. Available at: http://www.cancer.org/acs/groups/cid/documents/webcontent/003189-pdf.pdf (Accessed: January 3, 2012) 4. Tatsuta M. Yamamura H. Iishi H. Kasugai H. Okuda S. Value of serum alpha-fetoprotein and ferritin in the diagnosis of hepatocellular carcinoma. Oncology. 43(5):306-10, 1986. 5. Centers for Medicare and Medicaid Services (CMS) Medicare National Coverage Determinations (NCD) Coding Policy Manual and Change Report dated October 2011. Available at: https://www.cms.gov/CoverageGenInfo/04_LabNCDs.asp#TopOfPage. (Accessed: December 5, 2011). 6. ACOG educational bulletin. Maternal serum screening. Number 228, September 1996 (replaces no. 154, April 1991). Committee on Educational Bulletins of the American College of Obstetricians and Gynecologists. Int J Gynaecol Obstet. 1996;55(3):299-308. 7. ACOG Practice Bulletin No. 77: Screening for fetal chromosomal abnormalities. Obstet Gynecol. 2007;109(1):217-227. 8. Zhou L, Liu J, Luo F. Serum tumor markers for detection of hepatocellular carcinoma. World J Gastroenterol. 2006;12 (8): 1175-81. 9. Gilligan TD, et al. ASCO Clinical Practice Guidelines on uses of serum tumor markers in adult males with germ cell tumors. J Clin Oncol. 2010 Jul 10;28(20):3388-3404. 10. National Cancer Institute of National Institutes of Health information on Hepatocellular cancer. Available at: http://www.cancer.gov/cancertopics/pdq/screening/hepatocellular/healthprofessional/page3 (Accessed: January 17, 2012). 11. National Cancer Institute of National Institutes of Health information on Testicular cancer. Available at: http://www.cancer.gov/cancertopics/types/testicular (Accessed: January 17, 2012). 12. Sturgeon CM, Duffy MJ, Stenman UH, et al. National Academy of Clinical Biochemistry laboratory medicine practice guidelines for use of tumor markers in testicular, prostate, colorectal, breast, and ovarian cancers. Clin Chem. 2008;54 (12): e11-79. 13. International Germ Cell Consensus Classification: a prognostic factor-based staging system for metastatic germ cell cancers. International Germ Cell Cancer Collaborative Group. J Clin Oncol. 1997;15 (2): 594-603. 14. ACOG Practice Bulletin No 83: Management of Adnexal Masses. Obstet Gynecol. 2007;110(1):201-214. Proprietary Information of UnitedHealthcare. Copyright 2015 United HealthCare Services, Inc. Page 4 CMP-014_Alpha Fetoprotein_20170121_v2.2 POLICY HISTORY/REVISION HISTORY Date 01/21/2017 12/03/2015 Action/Description Updated ICD10 codes as per CMS recommendations. Removed ICD9 code file. Annual Policy Review Completed – changes made: Added ICD9 diagnosis codes related to liver neoplasm: 790.5, 790.6 Added ICD10 diagnosis codes related to liver neoplasm: R74.8, R74.9, R79.89, R79.9 10/01/2015 Removed ICD9 table. Embedded ICD9/ ICD10 PDF files. Proprietary Information of UnitedHealthcare. Copyright 2015 United HealthCare Services, Inc. Page 5 CMP-014_Alpha Fetoprotein_20170121_v2.2