Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
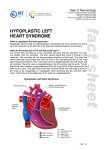
Commentary & & & & & & & & & & & & & & Dying of a Broken Heart: Ethics and Law in a Case of Hypoplastic Left Heart Syndrome Chet K. Pager, MD The short life of Baby P is reviewed. Baby P was an infant girl who was born with hypoplastic left heart syndrome and died at the age of 30 days. Effective, aggressive surgical treatment for this condition is rapidly developing in some countries, but is rarely available or successful in most. Baby P died without intervention. After presenting the history and background, the legal and ethical issues raised by this case regarding decision - making, futility, and best interests are reviewed. Journal of Perinatology 2000; 20:535 ± 539. CASE REPORT Baby P was born at term without complications, and weighing 3140 gm, in an Australian rural hospital. On day 2, Baby P's condition began to deteriorate, involving tachypnea, pallor, oliguria, and poor oxygen saturation. Treatment with lasix and morphine was commenced, and at 45 hours she was intubated and transferred by air ambulance to a tertiary referral hospital. Echocardiogram and cardiac catheterization confirmed critical aortic stenosis (pressure gradient 55 mm Hg) and a hypoplastic left ventricle. A balloon valvotomy was performed. Postoperatively, Baby P remained in cardiac failure. Further surgery was thought not to be appropriate, and after discussion with Baby P's parents, their agreement was obtained. However, the doctors saw no real treatment alternative within Australia, and none was offered to them overseas. On day 28, Baby P was returned to the rural hospital where she was born. By this time her weight had fallen to 2873 gm, and her medications included fursemide, spironolactone, digoxin, and chloral hydrate. Baby P's cardiac failure worsened despite maximal medical therapy, and her chest X-rays showed increasing cardiomegaly with pulmonary edema. Baby P remained in cardiac failure, with a heart rate of 140 to 150 and marked pulsus alternans, no palpable pulses, and virtually nonexistent capillary refill. Her liver was palpable 4 cm below the coastal margin, and X-ray revealed gross cardiomegaly and patchy lung consolidation. On day 30, Baby P was noted to be increasingly unsettled, requiring more frequent doses of chloral hydrate for ``sedation and comfort.'' At 6:25 PM, she suddenly ceased breathing. Resuscitation was not attempted, Royal Prince Alfred Hospital, Sydney, Australia. Address correspondence and reprint requests to Chet K. Pager, MD, C /- 67 Missenden Road PO, Camperdown, NSW 2050, Sydney, Australia. and the cause of death was thought to be a sudden arrhythmia or cardiac arrest. Medical Overview: Hypoplastic Left Heart Syndrome (HLHS) HLHS accounts for 25% of all deaths from congenital heart disease in the first month of life,1 with an incidence of 1:6000 births,2 although this is decreasing now that 37% of cases are detected prenatally with ultrasound.3 Until recently, HLHS was considered to be a uniformly fatal condition.1,4,5 Untreated, the median age of death is 4 to 5 days;2 and with maximal medical therapy median survival is only 60 days.6 Recent years have seen tremendous advancement in surgical technique and outcome for the surgical treatment of HLHS in specialized centers, using the Norwood and Fontan procedures. Hospital survival rates from large patient series in the United States are now routinely quoted well above 70%,4,5,7 with 5-year survivals in the range of 58% to 70%.5,8 ± 10 However, staged reconstruction does require multiple operations, and the infant would spend most of his or her first year of life in hospital. Neonatal heart transplantation has also significantly developed in recent years. Five-year survival rates now approach 80% for cardiac transplantation. Although a quarter of all HLHS patients will die waiting for transplantation,2,7 even with this mortality factored in, the survival rates for transplant are comparable with Norwood and Fontan-staged reconstructions, with improved quality of life and physical development.7,11 HLHS accounts for 60% of all pediatric heart transplantations in the United States.12 Both staged repair and transplantation are exceedingly complex procedures, and success is correlated directly with ongoing experience13; neither operation could be considered a routine or successful intervention except for specialist centers in select countries. Australian hospitals only receive about 50 cases of HLHS per year, and although some Australian surgeons are willing to attempt the Norwood and Fontan procedures, outcomes have generally been quite poor and the HLHS population insufficient to develop or maintain a satisfactory level of skill. Autonomy and Decision-Making Contemporary medical ethics is firmly placed within the individualist tradition of western philosophy, in which the increasingly dominant principle (both legally and ethically) is autonomy. However, the inability of the infant to express any preferences, the difficulty in accurately estimating prognosis, the long potential life span that might be enjoyed, and the family context in which the child exists all make such best-interest estimations quite difficult.14 Journal of Perinatology 2000; 20:535 ± 539 # 2000 Nature America Inc. All rights reserved. 0743-8346/00 $15 www.nature.com/jp 535 Pager Most societies acknowledge the preeminence of the parents' role in determining their child's best interests and their right to make decisions on their children's behalf. The important distinction is that parents have a responsibility to ensure their children's welfare; children are not their parents' possessions. The right of parents to make decisions for their children, therefore, is not absolute, and can be overridden in cases of parental incompetence, abuse, neglect, or decisions deemed inappropriate or contrary to the child's best interests. This latter point is the most difficult to define, and must be considered in the context of socially shared values; the most classic example being the Jehovah's Witness parent who refuses a life-saving blood transfusion for his or her child. This has been widely judged in law and ethics to be a decision that should be overturned.15 In fact, even some very reasonable decisions are denied parents in order that the state, parens patriae, may protect the best interests of its not-competent children with caution and disinterest. For instance, the decision to sterilize an intellectually disabled minor is one that should not be made by the child's parents or medical practitioners, but rather by the family court.16 In the case of Baby P, doctors appropriately related to her parents as the primary decision-makers. The parents were in agreement with her doctors' treatment plan. However, as the situation was presented to them, there was no real involvement in the decision-making process or true exercise of autonomy, only an after-the-fact acquiescence. It was suggested that there was really only one appropriate course of action; it was further hinted that should they make what was felt to be an inappropriate decision (for surgery), it might be refused to protect their baby's best interests. No mention was made of treatment alternatives available overseas. Although the decisions made may well have been in Baby P's best interests, the handling of this case was lacking in key elements of informed consent, disclosure, and voluntarism. Although the parent's role as Baby P's surrogate decision-makers was never subverted, neither was it exercised in any real sense: the parents had assented rather than consented. According to the fairly stringent legal and ethical standards for autonomy and informed consent, the management of this case was therefore lacking. The perinatologists involved argued that because no Australian insurance scheme covered overseas surgery and the parents clearly could not afford it, advising them of this option would only increase the parents' feelings of guilt. However, in cultures in which individual autonomy has primacy above beneficence, medical indications, or the professional role, this well-meaning paternalism, or even nationally based parochialism, is no longer appropriate. Futility and Best Interests If a treatment is considered futile, doctors may legally and ethically withhold or withdraw the treatment, even contrary to the patient's wishes.17 ± 19 Furthermore, doctors are under no obligation to even inform their patients of the existence of therapies they consider 536 Ethics and Law in a Case of HLHS futile.20,21 This view has been a longstanding and well-established principle. Even Hippocrates advised physicians to ``refuse to treat those who are overmastered by their diseases, realizing that in such cases medicine is powerless.''14 Although applying the concept of futility encounters difficulties, it is by no means an uncommon practice, particularly in neonatal settings. In fact, the most common mode of death in neonatal intensive care units is the limitation or withdrawal of treatment.20,22 ± 25 Unlike many areas, the courts have in most cases left the decision regarding a treatment's futility to the treating doctors. But although it seems clear that a doctor should be released from a duty of care where no good can be offered to the patient, arriving at formulae for what futility must entail is no easy matter.18 One well-known quantitative definition was proposed by Schneidermann26 which asserts that if the intervention does not work in more than 1% of attempts, it should be futile. Schneidermann uses physiological outcome: that treatment will fail ``to reverse a physiological disturbance that will lead to the child's proximate cause of death.''27 However, we do not judge worth by physiology alone. When faced with an imminently and irrevocably dying infant, one can well agree that aggressive treatment such as artificial ventilation should be considered futile, although such a treatment would certainly be physiologically successful, in that it would maintain breathing, if nothing else. This objection has yielded a second major approach to defining futility, namely that a treatment is futile if its intent or effect is to prolong dying without much benefit to the patient. However, the moment one deviates from strict physiological or mortality criteria, futility becomes an intrinsically value-laden idea that merely designates the far end of the burdens versus benefits continuum.18 Nonetheless, this broader yet more difficult conception of futility is in line with the reasoning of many ethicists and appears to better match patients' actual use and understanding of the word. Yet while strict (physiological) futility is poorly applicable to most ethical and medical decisions, by expanding one's definition to include ``benefit,'' two further problems are immediately encountered. The first problem is that one is forced to ask whether any considerations might outweigh the goal of preserving or extending life, even if this means achieving little else save a prolonged death. Although the principle of sanctity of life has its roots in diverse religious traditions, can be derived from the United States Constitution's guarantee of the ``right to life'' or from Kantian ethics, and comes perilously close to formal expression in recent United States case law,27 it is clear to many that relentless treatment to preserve life at all costs is not consistent with any but the most extreme doctrines of religion or ethics. Acknowledging this, Catholic theologians have traditionally distinguished ordinary treatments from extraordinary treatments (i.e., those that cannot be obtained or used without excessive expense, pain, or other inconvenience, or which, if used, would not Journal of Perinatology 2000; 20:535 ± 539 Ethics and Law in a Case of HLHS offer a reasonable hope of benefit). Doctors are not obligated to provide, nor patients to accept, extraordinary treatments.28 Instead of focusing on the nature of the treatment, one could focus on the subject being treated, and ask to what extent severely and permanently disabled patients ``can be regarded as being humanly alive in the sense in which we usually understand those words.''14 In a controversial argument rejecting the blanket sanctity of life, Singer29 has developed a system of ethics based on the idea of personhood, emphasizing that human rights and the importance of human life reside in those qualities that make us human beings, rather than merely human bodies. Tooley30 enumerated these as the capacity to have a concept of self; the actuality of being a conscious subject of experiences: a capacity for self-consciousness; and the actuality of being a continuing subject of experiences and other mental states. McCormick31 has added the capacity for relational potential to these criteria. This viewpoint is extremely contentious, but many would agree that ethical considerations depend both on the nature of the treatment and on the individual case at hand. Within Catholic theology, the concept of proportionality between the proposed treatment and the individual situation is replacing the ordinary versus extraordinary dichotomy. What remains, then, are difficult and case-dependent questions of burdens and benefits, best interests, and quality of life, ideas which are difficult to define or cleanly distinguish from one another. It may be difficult to admit that the severity of illness and burden of existence for some infants makes death preferable to continued life, but many would recoil from imposing painful treatment on an infant that at best will yield a few years' survival in constant and severe pain, unable to participate, even minimally, in human existence.32,33 As even Plato said, if a treatment would at best leave a patient with a ``useless life,'' then ``medicine was not intended for them and they should not be treated even if they were richer than Midas.''14 The English court's position on futility was best expressed by Lord Goff in the 1993 case of Airedale National Health Service Trust v Bland (AC789): ``I cannot see that medical treatment is appropriate or requisite simply to prolong a patient's life, when such treatment has no therapeutic purpose of any kind, as where it is futile because the patient is unconscious and there is no prospect of any improvement in his condition.''34 Likewise, the American Academy of Pediatrics recognizes that life-sustaining treatment, including artificial nutrition and hydration, may be withdrawn ``if treatment only preserves biologic existence.''35 The second problem involved with considerations beyond strictly physiological futility is one of decision-making. Futility, although imperfect, is in essence a matter for professional judgment. Questions of burdens, quality of life, and best interests are more explicitly value judgments. The courts do not easily recognize quality of life as a legal concept,34 and in the United States have seriously criticized the concept.35 Furthermore, in the case of never-competent individuals, decision-making is extremely difficult, and research has shown that doctors (and often surrogate decision-makers) consistently Journal of Perinatology 2000; 20:535 ± 539 Pager underestimate patients' subjective assessments of their own quality of life.34 It is for this reason that most recent publications on this subject have focused not on what futile or burdensome treatments are, but rather the process by which such decisions are made or conflicts resolved, through clear communication and consensus-building between the patients (or guardians) and doctors.17,35,36 However, there is a growing ethical and legal disquiet with any decisions, based on the value judgments of others, that result in an infant's death. The difficulties in adjudicating an infant's ``best interests'' have already been discussed. Other critics raise the symbolic value (to family, community and the medical profession) of providing treatment, even where the actuarial value of the intervention may be negligible. Some highlight the curious foundations of any ``universal'' ethical principle (such as futility) whose application varies with culture, technology, and geography. Certainly, in the case of Baby P, the ``futility'' of the Norwood and Fontan procedures depends entirely on whether she was born in America, Australia, or Africa, and under Schneidermann's definition, is further dependent on precisely what physiological goal one hopes to achieve. The differences in treatment, referral, information, and outcome Baby P and her parents might have received in the United States, be it due to organ availability, surgical skill, cost, ignorance, or other factors, raises problematic issues concerning the management and development of regional expertise, recently brought to the public eye, in part, by the Bristol case in the United Kingdom. In 1998, a group of pediatric cardiac surgeons at a peripheral hospital in Bristol attracted widespread notoriety for continuing to perform complex and high-risk surgery despite achieving outcomes significantly below the national standard.37 This situation, like the Baby P case, highlights the perennial problem imposed by an ever-increasing medical armament without concomitant advances in guidelines concerning their use and distribution.38 Responding to these ambiguities in both best interests and futility, it is one advocate's opinion that the courts ``leave vast discretion to the medical profession while both courts and doctors pay lip service to the sanctity of life.''35 In the United States, however, as science pushes at the bounds of the meaning of ``medical futility,'' the sanctity of life position has gained strength and is relied on more frequently by the judiciary.39,40 This position is best exemplified by aspects of the Baby Doe legislation, the Emergency Medical Treatment and Active Labor Act, the Americans with Disabilities Act, and the most recent Baby K Case.38 In this last case, ``treatment'' and futility as defined in the Emergency Medical Treatment and Active Labor Act were construed in their most narrow physiological sense, leading to a court-mandated ventilation of an anencephalic baby. An anencephalic baby lacks a functioning cerebral cortex, is permanently unconscious, has no cognitive ability, and cannot see, hear, talk, or feel pain. But it has an intact brainstem, and can emit reflex breathing, sucking, swallowing, and pain avoidance.38 Therefore, by the current ``brainstem'' legislative definition of death, 537 Pager anencephalic babies are alive and subject to the full protection of the Emergency Medical Treatment and Active Labor Act, the Americans with Disabilities Act, and other laws. Although American cases like Baby K have little bearing on and would not be expected from most other jurisdictions, they do highlight a general international trend for medical bodies, such as the American Medical Association, to increasingly focus on questions of quality of life, while the courts are called on to increasingly address sanctity of life. As the medical armament grows, this divergence will produce increasing tensions between medical practice and the law. CONCLUSIONS It is a peculiarity of philosophy that the conclusions reached are often less significant than the arguments used along the way, and this study has covered a large amount of territory. However, likely consensus positions regarding the issues raised through this case would include: (1) Baby P's parents will make all decisions so long as the parents are competent and the decisions appropriate and in Baby P's best interests. (2) Futile or extraordinary treatment need not be provided, even when parents request it. Burdensome treatment may be withdrawn or withheld, although court intervention may be required when agreement cannot be reached between parents and physicians. Within Australia, in the case of Baby P, surgical treatment of HLHS could reasonably be considered as futile. However, in specialist centers outside of Australia, surgical treatment of Baby P would by no means be futile, calling into question the adequacy of the informed consent for nontreatment in this case. The increasing complexity and fragmentation of medical competency further calls into question the universality of ethical principles when applied to medical decisions that are becoming increasingly dependent on geography, culture, technology, and individual circumstances. As medicine advances, along with geographical inequalities, concepts of futility and autonomy will become less applicable, and tensions between the sanctity and quality of life will increase. To reduce further divergence between medical practice and law, greater emphasis on the collaborative decision-making processes and conflict resolution are required. References 1. Cohen DM. Surgical management of congenital heart disease in the 1990s. Am J Dis Child 1992;146:1447 ± 1451. 2. Taeusch H, Ballard R. Avery's Diseases of the Newborn. 7th ed. Sydney: WB Saunders; 1998. 3. Tchervenkov CI, Tahta SA, Jutras LC, Beland MJ. Biventricular repair in neonates with hypoplastic left heart complex. Ann Thorac Surg 1998;66:1350 ± 1357. 4. Bove EL. Surgical treatment for hypoplastic left heart syndrome. Jpn J Thorac Cardiovasc Surg 1999;47:47 ± 56. 538 Ethics and Law in a Case of HLHS 5. Bove EL. Current status of staged reconstruction for hypoplastic left heart syndrome. Pediatr Cardiol 1998;19:308 ± 315. 6. Hoshino K, Ogawa K, Hishitani T, Kitazawa R, Uehara R. Hypoplastic left heart syndrome: duration of survival without surgical intervention. Am Heart J 1999;137:535 ± 542. 7. Hehrlein FW, Yamamoto T, Orime Y, Bauer J. Hypoplastic left heart syndrome: which is the best operative strategy? Ann Thorac Cardiovasc Surg 1998;4:125 ± 132. 8. Kern JH, Hayes CJ, Michler RE, Gersony WM, Quaegebeur JM. Survival and risk factor analysis for the Norwood procedure for hypoplastic left heart syndrome. Am J Cardiol 1997;80:170 ± 174. 9. Cohen DM, Allen HD. New developments in the treatment of hypoplastic left heart syndrome. Curr Opin Cardiol 1997;12:44 ± 50. 10. Bove EL, Lloyd TR. Staged reconstruction for hypoplastic left heart syndrome: contemporary results. Ann Surg 1996;224:387 ± 395. 11. Razzouk AJ, Chinnock RE, Gundry SR, et al. Transplantation as a primary treatment for hypoplastic left heart syndrome: intermediate - term results. Ann Thorac Surg 1996;62:1 ± 8. 12. Morrow WR, Naftel D, Chinnock R, et al. Outcome of listing for heart transplantation in infants younger than six months: predictors of death and interval to transplantation. The Pediatric Heart Transplantation Study Group. J Heart Lung Transplant 1997;16:1255 ± 1266. 13. Storch T. Passive euthanasia for HLHS. Am J Dis Child 1992;146:1426. 14. Mitchell K, Kerridge I, Lovatt T. Bioethics, Clinical Ethics for Health Care Professionals. 3rd ed. Sydney: Social Science Press; 1996. 15. Hamblin J. Blood transfusions and the limits of autonomy. Aust Health Law Bull 1999;7:49 ± 51. 16. Stow M, Croft P. Sterilization of intellectually disabled minors. Aust Health Law Bull 1994;3:28 ± 31. 17. Charatan F. AMA - issued guidelines on end - of - life care. BMJ 1999;318:690. 18. Council on Ethical and Judicial Affairs, American Medical Association. Medical futility in end - of - life care. JAMA 1999;281:937. 19. Goldsmith JP, Ginsberg HG, McGettigan MC. Ethical decisions in the delivery room. Clin Perinatol 1996;23:529 ± 550. 20. Balfour - Lynn LM, Tasker RC. Futility and death in paediatric medical intensive care. J Med Ethics 1996;22:279 ± 281. 21. Luce JM. Physicians do not have a responsibility to provide futile or unreasonable care if a patient or family insists. Crit Care Med 1995;23: 760 ± 766. 22. Goh AYT, Lum LCS, Chan PWK, Bakar F, Chong BO. Withdrawal and limitation of life support in paediatric intensive care. Arch Dis Child 1999;80:424 ± 428. 23. Kelly NP, Rowley SR, Harding JE. Death in neonatal intensive care. J Paediatr Child Health 1994;30:419 ± 422. 24. Hazebroek FW, Tibboel D, Mourik M, Bos AP, Molenaar JC. Withholding and withdrawal of life support from surgical neonates with life - threatening congenital anomalies. J Pediatr Surg 1993;28:1093 ± 1097. 25. Ryan CA, Byrne P, Kuhn S, Tyebkhan J. No resuscitation and withdrawal of therapy in a neonatal and a pediatric intensive care unit in Canada. J Pediatr 1993;123:534 ± 538. 26. Schneiderman LJ. The futility debate: effective versus beneficial intervention. J Am Geriatr Soc 1994;43:883 ± 886. 27. Best interests, sanctity of life. J Med Law 1995;14:331 ± 353. 28. Beauchamp T, Childress J. Principles of Biomedical Ethics. 4th ed. New York: Oxford University Press; 1994. 29. Singer P. Practical Ethics. Cambridge: Cambridge University Press; 1979. Journal of Perinatology 2000; 20:535 ± 539 Ethics and Law in a Case of HLHS 30. 31. 32. 33. 34. 35. Tooley M. Abortion and Infanticide. Oxford: Clarendon Press; 1983. McCormick RA. To save or let die: the dilemma of modern medicine. JAMA 1974;229:172 ± 176. Solbach G. Legal limits in the treatment of severely handicapped newborn infants? Klin Paediatr 1993;205:389 ± 393. Wainer S, Khuzwayo H. Attitudes of mothers, doctors, and nurses toward neonatal intensive care in a developing society. Pediatrics 1993;91:1171 ± 1175. Kerridge I, Low M, McPhee J. Ethics and Law for the Health Professions. Sydney: Social Science Press; 1998. Campbell AG, McHaffie HE. Prolonging life and allowing death: infants. J Med Ethics 1995;21:339 ± 344. Journal of Perinatology 2000; 20:535 ± 539 Pager 36. 37. 38. 39. 40. Dyer C. Mother loses bid to clarify rights of parents in treatment decisions. BMJ 1999;318:1167. Smith R. All changed, changed utterly: British medicine will be transformed by the Bristol case. BMJ 1998;316:1917 ± 1918. Flannery E. Conflicts and tensions in the Baby K case. J Law Med Ethics 1995;23:7 ± 12. Sewchuk TR. The uncertain ``best interests'' of neonates: decision - making in the neonatal intensive care unit. Med Law 1995;14:331 ± 358. Kapp W. Legal aspects. Schweiz Rundsch Med / Prax 1994;83:550 ± 555. 539