Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
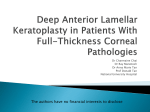
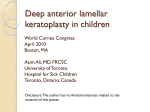
with Prof Charles McGhee & A/Prof Dipika Patel Series Editors Lamellar corneal surgery in 2016 MOHAMMED ZIAEI*, DIPIKA PATEL, CHARLES MCGHEE Introduction Full-thickness corneal transplantation is an operation that deals with a wide variety of corneal pathologies, but the procedure has not changed significantly since Eduard Zirm successfully performed the first penetrating keratoplasty (PK) over a century ago. Lamellar keratoplasty revolves around the concept of targeted replacement of diseased corneal tissue and techniques have evolved at an astonishing speed over the past 15 years. This article reviews some of the most recent developments in this field. Overview of lamellar surgery Lamellar surgery includes anterior lamellar keratoplasty (ALK) in which stromal tissue is selectively replaced, and endothelial keratoplasty (EK) which aims to replace damaged endothelial tissue (Fig 1.). Anterior lamellar keratoplasty ALK has undergone a renaissance with the dissemination of several new techniques since Arthur von Hippel performed the first successful anterior lamellar graft in 1886. This operation is the procedure of choice for a variety of corneal stromal disorders where the endothelium is healthy such as ectasia, stromal dystrophies and anterior stromal opacities. The modern version of this surgery, deep anterior lamellar keratoplasty (DALK), involves complete or near complete removal of diseased stromal tissue and perhaps the two most widely adopted techniques are Anwar’s “Big Bubble” technique (Descemetic DALK), and Melles’s “Closed manual dissection” technique (pre-Descemetic DALK). The major advantage of DALK surgery results from the retention of healthy native endothelium thereby eliminating endothelial allograft rejection, although epithelial and stromal rejection are still possible. Other advantages include a reduced need for topical steroids (15% vs 75% still on topical steroids after 12 months) and potential for earlier suture removal. Several studies have also shown that the visual quality with this form of keratoplasty is comparable to that of PK. The DALK procedure is also thought to be more cost effective when compared to full thickness corneal transplantation and reported to result in lower endothelial cell loss 1-3. In a recent meta-analysis whilst the proportion of patients achieving best corrected visual acuity ≥ 6/12 did not differ statistically between DALK and PK, the uncorrected and best corrected visual acuity levels were significantly better for PK. The DALK group however had a significantly lower frequency of graft rejection than the PK group 3. It is worthwhile noting that refractive error is a significant barrier to functional vision with one long term study reporting a mean refractive error of -6.5 ± 1.7 D after pre-Descemetic DALK and -6.1 ± 1.8 D after Descemetic DALK4. DALK does however have a steep learning curve and is technically more challenging to perform than PK. It is associated with unique potential complications such as Descemet’s membrane perforation, double anterior chamber (separation of the donor stroma tissue from the host Descemet’s membrane) and interface related issues. There are also some challenges associated with performing lamellar surgery in patients with a history of acute corneal hydrops, in individuals with a pre-existing split in Descemet’s membrane and patients with advanced ectasia. DALK makes up only 7% of corneal transplants performed in New Zealand in 2015 (unpublished data). This may reflect local population factors such as advanced ectasia or late presentation of patients. The low uptake of DALK could also be due to the fact that whilst DALK has a number of theoretical advantages over PK, long-term survival of DALK performed for keratoconus has been shown to be inferior to that of penetrating grafts in the recent Australian graft registry study. There have been some recent innovations in the field of anterior lamellar keratoplasty. One novel technique is that of femtosecond laser-assisted anterior lamellar keratoplasty (FALK) in which the depth of the recipient corneal pathology is measured using anterior segment OCT (AS-OCT). Subsequently the femtosecond laser is used to create the lamellar cut in the recipient and donor corneas and this depth can be adjusted based on the extent of the corneal pathology. The recipient’s scarred corneal tissue is then removed and replaced with the healthy donor lenticule. The lenticule can then be sutured into place or even retained by applying a contact lens in a “sutureless” procedure. Endothelial keratoplasty (EK) Charles Tillet performed the first known successful EK case in 1956 to treat corneal oedema. EK has since transformed beyond recognition and is now the procedure of choice for a variety of corneal endothelial disorders such as Fuchs’ endothelial corneal dystrophy and pseudophakic bullous keratopathy. The two most widely adopted techniques are Descemet stripping automated endothelial keratoplasty (DSAEK) in which the Descemet’s membrane endothelial complex is transplanted Fig 1. Different types of keratoplasties (9). (A) Penetrating keratoplasty. (B) Anterior lamellar keratoplasty. (C) Endothelial keratoplasty 22 NEW ZEALAND OPTICS October 2016 Fig 2. Anterior segment Optical Coherence Tomography (OCT) images of two patients who have undergone DSAEK. Note that the graft is fully attached in the top image and partially detached (arrow) in the bottom image. Fig 3. Anterior segment Optical Coherence Tomography (OCT) image of a patient following DMEK. Note the focal area of donor detachment nasally (arrow). with a sheet of stroma and Descemet’s membrane (Fig 2.), and Descemet’s membrane endothelial keratoplasty (DMEK) in which the Descemet’s membrane endothelial complex is transplanted in isolation and attached in a sutureless method through air tamponade (Fig 3.). Endothelial keratoplasty has replaced penetrating keratoplasty as the preferred technique for treating endothelial disease in the developed world, as it offers numerous advantages compared to PK. The most striking advantages of EK include the predictability and rapidity of visual rehabilitation associated with lower surgically-induced astigmatism. These advantages have driven the uptake of this technique. EK has also been shown to be more cost effective than PK as it is associated with fewer rejection episodes and requires less intensive patient follow-up. Other advantages of EK include the reduced need for topical corticosteroids and a tectonically stronger eye. In one large single centre study 50% of patients reached a best corrected visual acuity of Snellen 6/12 or better, by four months following DMEK, 18 months following DSAEK, and more than 24 months following PK. A best-corrected visual acuity of Snellen 6/7.5 or better at 24 months postoperatively was reached in 53% after DMEK, 15% after DSAEK, and 10% after PK 6. However, in another large study, 6/12 was achieved in 60.7% of patients following DSAEK at three months, 71.0% at six months, and 85.4% at 12 months7. Disadvantages of EK include the technically challenging nature of surgery, the need for special instrumentation and its association with unique potential complications such as graft dislocations requiring re-bubbling (re-injection of air into the anterior chamber), and interface related issues. There are also some challenges with performing EK in patients with a history of prolonged endothelial dysfunction in which the stroma has become scarred and in the presence of other ocular co-pathology such as iris defects, aphakia and in patients with a glaucoma drainage device. EK is now the gold standard procedure for endothelial disease comprising 31% of corneal transplants performed in New Zealand in 2015 (unpublished data). However, whilst there are a number of theoretical advantages over PK, long term survival of EK performed for Fuchs’ endothelial dystrophy has been shown to be inferior to that of penetrating grafts in the recent Australian graft registry study5. This has fuelled the interest in minimally invasive procedures such as cultured human corneal endothelial cell transplantation either as a monolayer or by injection of cells into the anterior chamber. Indeed we may soon see the widespread use of medical therapy in patients where topical treatment with Rho-associated kinase (ROCK) inhibitors, a molecule that enhances corneal endothelial survival, promotes cellular proliferation, and has the potential to inhibit and even reverse endothelial cell dysfunction8. Conclusion Penetrating keratoplasty has long been the standard of care for treating eyes with corneal disease with up to 95% long term success in keratoconus but nonetheless, significant shortcomings. Noteworthy barriers towards functional success include prolonged refractive instability and high irregular astigmatism. Advances in surgical instrumentation and technique are improving keratoplasty outcomes and it is widely believed that selective lamellar keratoplasty is the future of corneal transplantation. Advantages of lamellar surgery include a safer surgical procedure, quicker visual recovery, less need for topical steroids and a tectonically stronger eye. However, there needs to be further innovation and refining of current surgical techniques to improve survival rates and long-term outcomes of lamellar grafts. Until such time there will likely remain a place for penetrating keratoplasty. ▀ References 1. Koo TS, Finkelstein E, Tan D, Mehta JS. Incremental costutility analysis of deep anterior lamellar keratoplasty compared with penetrating keratoplasty for the treatment of keratoconus. Am J Ophthalmol. 2011;152(1):40-7 e2. 2. Keane M, Coster D, Ziaei M, Williams K. Deep anterior lamellar keratoplasty versus penetrating keratoplasty for treating keratoconus. Cochrane Database Syst Rev. 2014;7:CD009700. 3. Chen G, Tzekov R, Li W, Jiang F, Mao S, Tong Y. Deep Anterior Lamellar Keratoplasty Versus Penetrating Keratoplasty: A Meta-Analysis of Randomized Controlled Trials. Cornea. 2016;35(2):169-74. 4. Huang T, Hu Y, Gui M, Hou C, Zhang H. Comparison of refractive outcomes in three corneal transplantation techniques for keratoconus. Graefes Arch Clin Exp Ophthalmol. 2015;253(11):1947-53. 5. Coster DJ, Lowe MT, Keane MC, Williams KA, Australian Corneal Graft Registry C. A comparison of lamellar and penetrating keratoplasty outcomes: a registry study. Ophthalmology. 2014;121(5):979-87. 6. Heinzelmann S, Bohringer D, Eberwein P, Reinhard T, Maier P. Outcomes of Descemet membrane endothelial keratoplasty, Descemet stripping automated endothelial keratoplasty and penetrating keratoplasty from a single centre study. Graefes Arch Clin Exp Ophthalmol. 2016;254(3):515-22. 7. Khor WB, Han SB, Mehta JS, Tan DT. Descemet stripping automated endothelial keratoplasty with a donor insertion device: clinical results and complications in 100 eyes. Am J Ophthalmol. 2013;156(4):773-9. 8. Nakagawa H, Koizumi N, Okumura N, Suganami H, Kinoshita S. Morphological Changes of Human Corneal Endothelial Cells after Rho-Associated Kinase Inhibitor Eye Drop (Ripasudil) Administration: A Prospective Open-Label Clinical Study. PLoS One. 2015;10(9):e0136802. 9. Tan DT, Dart JK, Holland EJ, Kinoshita S. Corneal transplantation. Lancet. 2012;379(9827):1749-61. About the author * Dr Mohammed Ziaei completed his ophthalmic training at Moorfields Eye Hospital in London and is currently in his second year as a cornea & anterior segment fellow at the University of Auckland.