Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
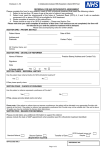
MoreLife Adult Referral Form (South Essex) Previously Carnegie Weight Management Patient Details Title: Date of birth: First name: Gender: Surname: Patient preferred contact number: Patient Address Email address (this will be the main method for contacting the patient) Postcode: Does the patient speak English? ☐ Yes ☐ No NHS Number: Is the patient registered disabled? ☐ Yes ☐ No ☐ Male ☐ Female If yes, please state: Does the patient have any mobility issues or are they housebound? ☐ Yes ☐ No Current Medical Information Height (m): Weight (kg): Blood Pressure: Resting Heart Rate: BMI: Exclusion Criteria* Can you confirm that your patient does NOT meet the following exclusion criteria: Active Bulimia Currently Pregnant Active Psychosis Diagnosed Personality Disorder Active Substance Use Disorder (SUD) including Alcohol Dementia Had Bariatric Surgery in the last 12 months Does the patient meet the EoE clinical criteria for Bariatric Surgery? (BMI>40kg/m2 PLUS severe sleep apnoea and/or Type 2 Diabetes) Confirm ☐ No ☐ No ☐ No ☐ No ☐ No ☐ No ☐ No ☐ Yes ☐ Yes ☐ Yes ☐ Yes ☐ Yes ☐ Yes ☐ Yes ☐ No ☐ Yes Referrer CCG use only * Patients found to have a score of severe anxiety/depression will be assessed on an individual basis Referral Criteria For South Essex One of the following three criteria must be met A BMI of 40 kg/m2 or more A BMI of ≥ 35 kg/m2 and obesity-related comorbidity eg Type 2 Diabetes, metabolic syndrome, hypertension, obstructive sleep apnoea (OSA), functional disability, infertility and depression if specialist advice is needed regarding overall patient management A BMI of ≥ 32.5 kg/m2, type 2 diabetes and of Asian descent (CP&R and Southend) Confirm ☐ OR ☐ ☐ OR ☐ ☐ OR ☐ CCG use only All of the criteria below must be met Referrer Aged 17 years or over Registered with a Practice within South Essex, or if unregistered, residing in South Essex Morbid or severe obesity has been present for at least four years A commitment to change behaviours Discussions covering understanding of the likely resulting health problems, assessment of the individual health risks and engagement in a partnership, preferably using motivational interviewing, to modify the risks as part of a holistic approach that includes emotional wellbeing. Previous attempts at weight loss including participation in a community or commercial Tier II weight management plan In exceptional circumstances patient with BMI < 35 kg/m2 is referred, waist circumference and reasons for referral should be given as prior approval is required from the CCG ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ (CP&R and Southend) Use this area to supply further information evidencing how the patient meets the above criteria if necessary: CCG use only (Castle Point and Rochford and Southend CCGs only) Intervention authorised by: Name Signature Date Pathology (Where available please ensure these are from the last three months) Hb1AC Date: Reading: Total Cholesterol Date: Reading: Haemoglobin Date: Reading: HDL Date: Reading: Creatinine Date: Reading: Triglycerides Date: Reading: TSH Date: Reading: LDL Date: Reading: FT4 Date: Reading: ALT Date: Reading: Current Medical History (within the last 6 months) Metabolic (Select all that apply) Cancer ☐ Mechanical (Select all that apply) Osteoarthritis (OA) Ischaemic Heart Disease (IHD) Other arthritis (eg Rheumatoid etc) Cardiomyopathy Heart Failure Peripheral Vascular Disease (PVD) Myocardial Infarction (MI) Stroke Transient Ischaemic Attack Hypertension Diabetes Type 1 Diabetes Type 2 Hypothyroidism Polycystic Ovary Syndrome (PCOS) Hyperlipidaemia Fatty Liver Other ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ Asthma Obstructive Sleep Apnoea (OSA) Mental Health (Select all that apply) Anorexia Nervosa Binge Eating Disorder Bulimia Nervosa Anxiety Depression Schizophrenia/other psychotic disorder Alcoholism Drug Abuse Other Other Other Or return to MoreLife (UK) Ltd. Churchwood Hall, Leeds Metropolitan University, Headingley Campus, Leeds, LS6 3QJ. Email: [email protected] Please note, incomplete referral forms will be returned. ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ ☐ Medication (please list current medications) Obesity Stages: Please choose ONE of the following stages of obesity that best describes your patient Stage 0: No Apparent Risk Factors ☐ Patient has no apparent obesity-related risk factors (e.g. blood pressure, serum lipids, fasting glucose etc. within normal range) no physical symptoms, no psychopathology, no functional limitations and/or impairment of well-being Stage 1: Preclinical Risk Factors ☐ Patient has obesity-related subclinical risk factors (e.g. borderline hypertension, impaired fasting glucose, elevated liver enzymes etc.) mild physical symptoms, mild psychopathology, mild functional limitations and/or mild impairment of well-being Stage 2: Established Co-Morbidity ☐ Patient has established obesity-related chronic disease (e.g. hypertension, type 2 diabetes, sleep apnoea, osteoarthritis, PSOS, anxiety disorder etc.) moderate limitations in activities of daily living and/or well-being Stage 3: End-Organ Damage ☐ Patient has established end-organ damage such as myocardial infarction, heart failure, diabetic complications, significant psychopathology, significant functional limitations and/or impairment of well-being ☐ Stage 4: End-Stage Patient has severe (potentially end-stage) disabilities from obesity-related chronic diseases, severe disabling psychopathology, severe functional limitations and/or severe impairment of well-being Referral Source details Patient’s Surgery Name: Surgery Address: Surgery Postcode: Surgery contact number: Referrer’s name: Referrer’s profession: Referrer’s signature: Date of referral: (not necessary if emailed) Please e m a i l t o m o r e l i f e @ n h s . n e t fax to 01245 396 934 o r with any supplementary patient pathology records which need to accompany the referral form. Or return to MoreLife (UK) Ltd. Churchwood Hall, Leeds Metropolitan University, Headingley Campus, Leeds, LS6 3QJ. Email: [email protected] Please note, incomplete referral forms will be returned.