Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
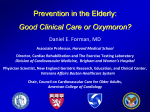
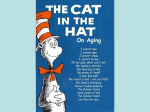
Aging America: Clinical Management of the Elderly Patient Pat Segu, OD FAAO Clinical Associate Professor Definitions Gerontology a branch of knowledge involving the study of aging and problems associated with the aged Geriatrics a specialized part of gerontology; it covers the mental and physical health aspects and problems of elderly individuals Definitions Aging – to show signs of growing old; succession of states of a system along a time line Ageism – bias or prejudice against elderly people based on belief that older people are incapacitated or incompetent simply b/c they are old Senescence – condition of growing old Definition Elderly Population Young Old 65 – 74 Middle Old 75 – 84 Old - Old > 85 yrs Each Age group require different aspects of our attention Definition Older Patient Well Elderly Moderate Impaired Elderly Severely Impaired Elderly Well Elderly Independent Chronic Health Problems NOT Functionally Impaired Susceptible to age-related diseases (i.e. Cataracts) Patient Education Importance of Annual Eye Exam Education Regarding Disease Moderate Impaired Elderly Compared to Well-Elderly-may have same or more chronic health conditions Need help with Daily Living Activities Cooking Personal Care Shopping Assistive Devices – Walkers / Wheelchair Multiple Meds Impt Complete List of Medication Possible SE interfere with Visual System Severely Impaired Elderly Many Disabling Conditions Multiple RX & OTC Meds “Confusion” Homebound or Long-term care facility Nursing Home What is your Aging IQ? The older you get, the less you sleep. True or False FALSE Quality of sleep declines but NOT the total sleep time Elderly take more naps throughout the day Overall get the same amount of sleep except that the sleep is fragmented What is your Aging IQ? Families Don’t Bother with Their Older Relatives. True or False FALSE Most Elderly live close to their children and many live with their spouses Approx. 5 % nationwide live in nursing homes Cultures Differences What is your Aging IQ? Does IQ Change with age? Yes or No NO No serious decline in intelligence with age Wisdom increase with age Rate/Speed of learning decreases with age Absorbing new information at an older age maybe more difficult Calculated IQ test may be lower because of emphasis on speed What is your Aging IQ? Everyone becomes confused or forgetful if they live long enough. True or False FALSE Alzheimer’s can cause confusion and forgetfulness Many Treatable problems may also elicit these symptoms Poor Nutrition Adverse Drug Reaction Depression What is your Aging IQ? Falls and injuries are most common among people over 65 years of age True or False TRUE Important for Regular Hearing and Vision Tests Good Safety Habits to prevent accidents Adverse Drug Reaction can affect balance and coordination Characteristics of Aging Common Physical Changes Decreased Hearing Vision Taste Smell Increase reaction time for complex tasks Decrease ability to multi-task Disease and injury is more difficult to recover from as we age Clinical Impact Elderly Patients Cardiovascular diseases Cancer Cerebrovascular disease DM Rheumatic disorders Smoking Poor nutrition Alcohol abuse Lack of exercise Mental Health Depression Dementia Clinical Impact Elderly Patients Auditory considerations Loss of high frequency pitch Presbycusis Progressive Hearing Loss occurring bilaterally Affects 30% of 65-74 yrs 50% of >75yrs and older Tinnitis affects Vertigo 30% of people over 65 Psychological considerations Retirement Declining health Decreased mobility* Income decline Sensory decline Decreased response time Death of a spouse Children leaving home Reduction in social role Institutionalization Elder abuse Prescribing Considerations Physiological changes metabolism decreased liver and kidney function decreased muscle mass/increased body fat decrease GI absorption & serum protein Toxicity (systemic medications) Poly-pharmacy Side effects Contraindications with other meds Family Support Expressive Instrumental Advice Affection Love Financial Transportation Household Tasks Informal or unpaid care estimated to account for 95% of all care given to older adults Family Support Social Change Relocation Family Size Smaller More women in the workforce Grandparents help with looking after grandkids Increased longevity of older results Demographics of Aging in America “Graying of America” www.aoa.gov (Administration on Aging) Elderly Populations “Graying of America” (65+) Increase in Elderly Population (>65yrs) Decrease infant mortality Preventive health care measures Advanced life saving technology Improved Clinical Medicine In the U.S., approximately 1 person out of every 8 is an older American 2002: 35.6 Million (increase of 10.2% from 1992) “Graying of America” Future Growth 2011-2029 the “coming of age” of baby boomers will yield a sudden sharp increase By the year 2030, the older population will more than double to 71.5 million Age group of >85 is increasing the most quickly 3.1 % of US Labor Force “Graying of America” Future Growth “Graying of America” Future Growth Figure 1: Number of Persons 65+, 1900 - 2030 (numbers in millions) 80 70 60 50 40 30 20 10 0 71.5 54.6 25.7 31.2 35 40.2 16.7 3.1 4.9 9 1900 1920 1940 1960 1980 1990 2000 2010 2020 2030 Year (as of July 1) Life Expectancy Life Expectancy 1900 47.9yrs Life Expectancy 2001 77.2 yrs F (78-79 yrs) vs. M (71-72yrs) Centenarians in the U.S. In the year 1990: 37,306 In the year 2002: 50,364 Represents in increase of 35%. Living Arrangements (2001-02) Majority of Elderly live in the community 5% of adults live in institutional setting 80% Homeowners vs. 20% Renters Older Men More Likely to be Married ½ of the Older Female live alone Less likely to Relocate Living Arrangements Women Men 10% 19% 40% 41% living with spouse living alone Other 18% 72% living with spouse living alone Other Marital Status Men more likely to be married vs. Female ½ of Older Females widows (2002) 10% Older population divorced or Figure 2: Marital Status of Persons 65+ - 2002 separated 80% 73% 70% 60% 50% 41% 46% Women Men 40% 30% 14% 20% 10% 10% 9% 4% 4% 0% Married Widowed Divorced or Single (never Separated/ married) Spouse Absent Geographic Distribution (2002) Top 5 States California Florida New York Texas Pennsylvania 3.7 2.9 2.5 2.2 1.9 million million million million million Most Older American lived in metropolitan areas (77%) Education Among Elderly (2002) Education Level is Increasing Between 1970 and 2002, the percentage completed High school increased from 28% to 70% 74% 68% 51% 35% Caucasians Asians AA Hispanics 17% Bachelor Degree or more Economic Status (2002) Sources Social Security Income from Assets Public & Private Pensions Earnings 91% 58% 40% 22% Poverty rate: 10.4% Elderly group are actually wealthier Net Worth increases until Age 74 Median Net Worth (2000) was $108,000 vs. $55,000 for total population Economic Status (2002) Family Households 65+ Householder 0.0% Under $10,000 5.0% 10.0% 15.0% 20.0% 25.0% 4.5% 7.1% $10,000 - $14,999 20.9% $15,000 - $24,999 19.6% $25,000 - $34,999 18.4% $35,000 - $49,999 $50,000 - $74,999 $75,000 and over 15.3% 14.3% Economic Status (2002) Poverty About 10% of all elders have incomes < the poverty line Older Women > Older Men AA > Hispanics > Caucasians Older Hispanic women living alone HIGHEST Poverty Rates (47%) Health and Health Care Majority of Elderly are Healthy Greater Disability with >80+ Relationship Disability & Health Status Most Older Adults have 1 Chronic Condition Probable Multiple Chronic Disease Chronic Health Conditions Sensory Impairments and Oral Health Use of Time Use of Time Vision Care and the Elderly Vision Care and the Elderly Vision Care Needs will INCREASE Correction of Refractive Error & Presbyopia Problems Dry Eyes Cataracts Floaters Age-related macular degeneration Retinopathy Glaucoma Medicare Billing Increase need for LV services Evaluation Vision Care Setting Private Office Private Residence Hospital Nursing Home Evaluation Visual and Non-visual Needs BVA in Office = Home Environment Familiar with Home Environment Functional Demand Services Available Optometric Evaluation Gross Observations Hearing Impairment “Confusion” Fatigue Asymmetry / Note Lid Margins Mobility Careful Case History CC Ocular Medical Meds / Allergies Social Mental Functional DIFFICULTY IN TAKING A CASE HISTORY Reduced VA Impaired Hearing Cognitive Ability Slower Response Under Report Visual Symptoms Time Consuming Functional Abilities Effect on Everyday Function Ex. Patient w/ Arthritis Unable to Open Bottle Ask Patient Able To Perform Activities Shopping Cooking Self-Medication Reading Mail Writing Bills Visual Acuity Enhanced using LV charts with increase contrast Contrast sensitivity testing good to explain non-specific complaints Multiple Glasses – test with more freq worn Rule out Media Opacity Pinhole VA to ______________ Problems with GLARE Amsler Grid Normal Ocular Aging Changes Decreased vergence ability (speed & amplitude) Diplopia Break down of a high phoria Stereopsis might be reduced after age 50 Impaired smooth pursuits Slower eye movements Refractive error Hyperopic shift vs. myopic shift Astigmatism Shift from WTR to ATR Optical aberrations Increased diffraction (smaller pupil) Age induced miosis R/O Trauma / Inflammation / Surgery Increased light scatter Presbyopia Age norms 45 yrs 50 yrs 55 yrs >55 yrs +1.50 +2.00 +2.50 +2.50 (if working dist is 40cm) Calculated amplitude minimum = 15.0 – 0.25 (age) average = 18.5 – 0.3 (age) maximum = 25.0 – 0.4 (age) Aphakic Correction High plus lenses 25% Magnification Objects appear larger and closer Pin-cushion distortion Ring scotoma “Jack-in-the-box” Increase vergence demand Practice Strategies Concentrate on Geriatric Population 15-20 minutes from Practice Community Service Activities Public education Vision screening Network health care providers Employing staff member >55 yrs Practice Strategies Adjust exam time Do not use reflective or glossy paper for materials Avoid blue, violet, or green colored paper Good Contrast of furniture, walls, carpets etc Proper lightening Handicap accessible Door handle that pulls Reception counter waist level Office should not be cluttered REMEMBER Handle One Complaint @ a time Case History Never Ends Educate Your Patient Refer Mental problems Physical problems Normal Age Related Vision & Ocular Changes Adnexa Orbital Aging Changes Orbital fat shrinks Lids become flaccid Entropion Ectropion Dry Skin Orbital fat prolapses into upper nasal lid Decreased levator function Adnexa Dermatologic Decreased Elasticity Muscular tone Wrinkling Increased chance of infection Dermatochalasis Decreased Cilia Adnexa EOMs Fibrosis/sclerosis leads to relative restriction, especially superiorly Aperture Lateral canthus drifts inward Reduced levator function shortens lateral dimension shortens vertical dimension Sagging Skin shortens vertical dimension Loss of Elasticity “Snap-Back Test” Failure of the lid to snap back into position eyelearn.med.utoronto.ca/. ../04Ectropion.htm Ectropion Horizontal Lid Laxity Snap Back Test Medial Canthus Tendon Laxity Pull LL laterally & evaluate position of puncta Pull center part of LL >10 mm Failure to snap back into position Normal – 1-2 mm displacement of puncta Mild – Position of puncta @ limbus Severe – Position of puncta @ pupil Lateral Canthus Tendon Laxity Ability to pull LL medially > 2mm Uneven Eyelid Margins Normal aging change Check to see that a mass isn’t causing this (Sebaceous carcinoma) Recurrent chalazia need to be biopsied Adnexa Tear Film Important in Maintaining Corneal Integrity Decreased Stability and Production Aqueous deficiency most common problem with the elderly Reduction in Blink Rate (blinks/minutes) Lubrication Disinfection Removal of Debris 3-4 vs. 15-20 Complaints of Dry Eye Symptoms Sjogren’s syndrome, post-menopausal females, medications Management Tear Supplementation & Ectropion Repair Conjunctiva Saggy, loose, “redundant” Vasculature Increase in size and number Subconjunctival hemorrhage Increased incidence Caution w/patients taking blood thinners Coumadin Plavix Clarity Decreased; yellowing due to hyaline changes and fat deposits Sclera Clarity More transparent and yellow Due to dehydration and lipid deposits Increase in Rigidity Senile Scleral Plaque Senile Scleral Plaque Senile Scleral Plaque Local area of excessive scleral thinning Occurs at the area of the insertions of the rectus muscles (MR & LR) Thin clear area, may be dark if it is very thin and you are seeing the choroid through it Benign