Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cardiovascular disease wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
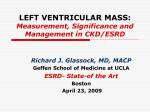
28 Journal of the association of physicians of india • JANUARY 2014 • VOL. 62 Original Article Echocardiographic Assessment of Cardiac Dysfunction in Patients of End Stage Renal Disease on Haemodialysis Mukesh Laddha*, Vishal Sachdeva*, PM Diggikar**, PK Satpathy ***, AL Kakrani **** Abstract Objective: To assess the prevalence of systolic and diastolic dysfunction in patients of end stage renal disease (ESRD) on haemodialysis. Methods: Seventy patients with ESRD were subjected to two-dimensional and M mode echocardiography for determination of systolic and diastolic dysfunction. All patients were evaluated clinically, biochemically and radiologically and were diagnosed as chronic kidney disease (CKD). The left ventricular ejection fraction (LVEF) and fractional shortening (FS) were taken as measures of left ventricular (LV) systolic function. Diastolic function was determined by measuring E/A ratio by spectral doppler LV inflow velocity. Echocardiographic findings of hypertensive and normotensive patients were compared. Results: Out of 70 patients studied, there were 53 males (75.7%) and 17 females (24.3%). Hypertension (37.1%) was leading cause of ESRD. Echocardiography showed that left ventricular hypertrophy (LVH) was present in 74.3%. Systolic dysfunction as measured by reduced fractional shortening (< 25%) and decreased LVEF (< 50%) was present in 8.6% and 24.3% respectively. Diastolic dysfunction as denoted by E/A ratio of less than 0.75 or more than 1.8 was present in 61.4% of patients. Regional wall motion abnormality (RWMA) was present in 12.9%. Pericardial effusion was noted in 14.3% of patients. Valvular calcification was noted in 7.1% of ESRD patients. Mean left ventricular internal diameter in diastole was 45.55 ± 6.03 mm. Mean Interventricular septum diameters in systole was12.2 ± 1.71 mm. Mean left atrium diameter was 33.01 ± 4.11 mm. Normotensive group was compared to hypertensive group. Statistically significant difference was noted in LVH and E/A ratio in hypertensive group as compared to normotensive group. Conclusion: Patients with hypertensive ESRD had higher prevalence of diastolic and systolic dysfunction as compared to normotensive counterparts. Introduction E nd stage renal disease (ESRD) is the irreversible deterioration of renal function which results into impairment of excretory, metabolic and endocrine functions leading to development of the clinical syndrome of uraemia. Chief Resident, **Associate Professor, ***Professor, **** Professor and Head, Department of Medicine, Dr. D.Y. Patil Hospital, Pimpri, Pune-411 018 Received: 24.02.2012; Revised: 09.05.2012; Accepted: 09.05.2012 * 28 Chronic kidney disease (CKD) is not uncommon but fortunately treatable and it is recognised worldwide as a public health problem. Patients with CKD are at significantly increased risk for both morbidity and mortality from cardiovascular disease (CVD). Patients on dialysis have a 10- to 30-fold increased risk for cardiovascular mortality compared with the general population. CVD is the single most important cause of death among patients receiving long-term dialysis; accounting for 44% of overall mortality. 1 The magnitude of the problem has become more apparent as patients now survive longer on maintenance haemodialysis. Coronary artery disease including myocardial infarction, congestive heart failure (CHF) and pericardial disease are the common manifestations of major cardiovascular © JAPI • january 2014 • VOL. 62 29 Journal of the association of physicians of india • JANUARY 2014 • VOL. 62 abnormalities in the ESRD. 30% of patients reaching ESRD already have clinical evidence of ischaemic heart disease or CHF. Furthermore patients with a reduced glomerular filtration rate (GFR) are more likely to die of CVD even before they are to develop ESRD. Heart failure accounts for 15%, myocardial infarction for about 10% and pericarditis for about 3% of dialysis associated mortality. 2 Sudden cardiac death may be related to the high prevalence of left ventricular dysfunction secondary to the LVH in dialysis patients. 3 Both traditional and non-traditional risk factors play a role in the aetiology of these cardiac problems. Many patients with CKD die prematurely before or after beginning dialysis. Reasons for these adverse associations are not well understood. Whether CVD events differ in patients with and without CKD is poorly defined. The relative importance of nontraditional risk factors for CVD in CKD is not well defined. Similarly, whether differences in CVD in CKD patients suggest preventive or therapeutic strategies unique to this population is unclear. Although patients with CKD have a high prevalence of many of traditional risk factors, such as diabetes, hypertension, and LVH, they also are exposed to nontraditional or uraemia related risk factors that increase in prevalence as kidney function declines e.g. a high percentage of haemodialysis patients have higher levels of homocysteine, oxidative stress, lipoproteins, and lipoprotein remnants. The known common cardiac abnormalities in ESRD are increase in LV cavity size, thickened LV posterior wall, thickened interventricular septum, region wall motion abnormality, decrease in LV compliance, pericardial effusion and calcific/sclerotic valves. Material and Methods Seventy patients of CKD irrespective of aetiology having ESRD (stage 5 CKD) were included in the study. A person was considered CKD if his illness was of more than 3 months duration and had abnormal USG findings and reduced creatinine clearance pointing to chronic kidney disease. A person was labelled ESRD if his GFR was below 15 ml/min per 1.73m 2 as per Cockcroft Gault equation and who was on haemodialysis. The following patients were excluded from the study; pre-existing cardiac disease like rheumatic heart disease, congenital heart disease, other pre-existing cardiovascular disease like myocarditis due to infective aetiology, primary heart muscle diseases like cardiomyopathies. All these patients were clinically evaluated for cardiac involvement, the following investigations were done on all the patients; complete haemogram, renal © JAPI • january 2014 • VOL. 62 function test, serum electrolytes, blood glucose level, lipid profile, ECG, chest X-ray and 2-D echo. 2D- Echocardiography machine GE LOGIQ 400 PRO was used with 3.5 MHz transducer probe. Two dimensional echocardiography and M- mode echocardiography performed. The M. mode recording perpendicular to the long axis of and through the centre of the left ventricle at the papillary muscle level were taken as standard measurements of the systolic and diastolic wall thickness and chamber dimensions. The LVEF and fractional shortening (FS) were taken as measure of left ventricular systolic function. Diastolic function was determined by measuring E/A ratio by special Doppler inflow velocity (E is peak early diastole velocity and A is peak atrial filling velocity of left ventricle across mitral valve). E/A ratio less than 0.75 and more than 1.8 was considered as diastolic dysfunction. LVH was diagnosed when interventricular septum thickness or left ventricular posterior wall thickness was ≥ 12 mm. Fractional shortening (s) was calculated as FS (%) = (LVDd-LVDs) (LVDd) × 100 Normal range being 25% to 45% LVDd: Left ventricle internal diameter in diastole LVDs: Left ventricle internal diameter in systole Ejection fraction was calculated as LV EF (%) = LVVd-LVVs × 100 Normal = 59.2 ± 6% (LVVd) LVVd: Left ventricle volume in diastole LVVs: Left ventricle volume in systole Statistical analysis: was done by SPSS software version 18 by using chi square test. A ‘p’ value less than 0.05 was considered significant. Results Out of 70 patients, there were 53 males (75.7%) and 17 females (24.3%). Maximum number of patients belonged to age group of 51-60 years (26). Mean age of ESRD patients was 53.3 ± 12.8. Hypertension (37.1%) was leading cause of ESRD, other causes included diabetes (21.4), diabetes with hypertension (10%), chronic glomerulonephritis (8.6%), polycystic kidney disease (7.1%), obstructive uropathy (5.7%), analgesic nephropathy (2.9%) and aetiology remained unknown in 7.1% cases. Mean haemoglobin percentage was 7.78 ± 1.84 gm%. Mean blood urea level was 151.7 ± 51.37 mg%. Mean serum creatinine level was 10.35 ± 5.56 gm%. Mean serum cholesterol level was 205.8 ± 47.69 mg/ dl. Serum cholesterol level was elevated in 60% of patients. Mean serum triglyceride level was 183.4 ± 36.76 mg/dl; it was elevated in 84.3% of patients. Mean 29 30 Journal of the association of physicians of india • JANUARY 2014 • VOL. 62 serum LDL level was 120 ± 33.7mg/dl; it was elevated in 77.1% of patients. Mean serum HDL level was 35.67 ± 6.11 mg/dl; it was decreased in 67.1% of patients. in 7.1%, QT prolongation and low voltage pattern in 5.7%, ventricular tachycardia in 2.9% and complete heart block in 1.4% was noted. ECG changes in decreasing order of frequency were sinus tachycardia in 48.6%, LVH in 45.7%, ST -T changes in 30%, ventricular ectopics and Tall ‘T’ wave Following parameters of echocardiography were studied and analysed in detail; these were left ventricular internal diameter in systole and diastole, interventricular septum diameter in systole, left ventricular posterior wall diameter, E/A ratio, FS and LVEF (Tables 1 and 2). Table 1 : Mean echocardiographic parameters in ESRD study cases Mean echocardiography parameters in cases of ESRD Left ventricular internal diameter in diastole (LVIDd) (mm) Left ventricular internal diameter in systole (LVIDs) (mm) Interventricular septum diameter in systole (IVS) (mm) Left ventricular posterior wall diameter (LVPWD) (mm) Left atrium diameter (mm) Fractional shortening (%) Ejection fraction (EF) (%) ‘E’ peak early diastole velocity mm/sec ‘A’ peak atrial filling velocity mm/sec E/A ratio Mean values 45.55 ± 6.03 29.8 ± 6.02 12.2 ± 1.71 12.0 ± 1.81 33.01 ± 4.11 34.06 ± 8.41 54.91 ± 9.62 73.47 ± 16.21 83.8 ± 24.5 0.95 ± 0.35 Table 2 : Echocardiographic findings in ESRD study cases Echocardiographic finding in cases of ESRD Left ventricular hypertrophy Fractional shortening (< 25%) Ejection fraction (< 50%) E/A ratio (< 0.75 or >1.8) Regional wall motion abnormality Pericardial effusion (< 10 mm) Valvular calcification Mitral regurgitation No. of cases Percentage 52 6 17 43 9 10 5 5 74.3 8.6 24.3 61.4 12.9 14.3 7.1 7.1 Patients were categorised into two groups; first having serum cholesterol more than 200 mg/dl and second having serum cholesterol less than 200 mg/dl. Correlation of 2D-echo findings and serum cholesterol were analysed (Table 3). Hypertension was considered when blood pressure was more than 140/90 mmHg. All patients were categorised into hypertensive and normotensive group according to blood pressure. Findings of 2D- echo were compared among hypertensive and normotensive ESRD patients (Table 4 and Figure 1). Discussion Premature cardiovascular disease is a significant cause of morbidity and mortality among patients with CKD. Premature atherosclerotic coronary disease is driven by multiple risk factors, including dyslipidaemia and oxidative stress. Four main structural abnormalities of the heart have been described in patients with CKD: LV hypertrophy, expansion of the nonvascular cardiac interstitium leading to inter-myocardiocytic fibrosis, changes in vascular architecture, and myocardial calcification. All these abnormalities promote systolic as well as diastolic LV dysfunction which predisposes to Table 3 : Correlation analysis of total cholesterol with echocardiographic parameters in ESRD study cases Echocardiographic findings LVH Absent Present Decreased EF Absent Present Decreased FS Absent Present Abnormal E / A ratio No Yes RWMA Absent Present Pericardial Effusion No Yes 30 TC < 200 mg/dL Group ( n = 28) n % TC > 200 mg/dL Group (n = 42) n % Chi-square value P value 0.11 10 18 35.7 64.3 8 34 19.0 81.0 2.44 23 5 82.1 17.9 30 12 71.4 28.6 1.04 25 3 89.3 10.7 39 3 92.9 7.1 0.27 17 11 60.7 39.3 9 33 21.4 78.6 11.10 27 1 96.4 3.6 34 8 81.0 19.0 3.59 < 0.05* 26 2 92.9 7.1 34 8 81.0 19.0 1.94 0.16 0.30 0.60 < 0.01* © JAPI • january 2014 • VOL. 62 31 Journal of the association of physicians of india • JANUARY 2014 • VOL. 62 Table 4 : Correlation analysis according to echocardiography finding in hypertensive and normotensive ESRD study cases Echocardiographic findings LVH Absent Present Decreased EF Absent Present Decreased FS Absent Present Abnormal E / A ratio No Yes RWMA Absent Present Pericardial Effusion No Yes Normotensive Group ( n = 22) Hypertensive Group (n = 48) Chi-square value n % n % 12 10 54.5 45.5 6 42 12.5 87.5 13.96 19 3 86.4 13.6 34 14 70.8 29.2 1.97 20 2 90.9 9.1 44 4 91.7 8.3 0.01 13 9 59.1 40.9 13 35 27.1 72.9 6.62 21 1 95.5 4.5 40 8 83.3 16.7 1.97 19 3 86.4 13.6 41 7 85.4 14.6 0.01 P value < 0.01* 0.16 0.91 < 0.05** 0.16 0.91 dysfunction by LVEF measurement in haemodialysis patients.6 S.Agarwal et al (2003) had observed diastolic dysfunction in 60% and systolic dysfunction in 15% of patients. 7 The above findings were consistent with our study. Fig. 1 : Figure showing correlation analyses according to echocardiography finding in hypertensive and normotensive ESRD study cases symptomatic heart failure, which in turn is a risk factor for premature death. In this study LVH was present in 74.3%, systolic dysfunction was present in 24.3% of patients as suggested by reduced LVEF measurement and diastolic dysfunction was observed in 61.4% by abnormal E/A ratio of ESRD patients. Mild pericardial effusion (less than 10 mm thickness) was present in 14.3% patients. Mitral and aortic valve calcification and mitral regurgitation was noted in 7.1% patients. Robert N. Foley et al (1995) had found abnormalities of left ventricular structure and functions were very frequent on baseline echocardiography: 73.9% had left ventricular hypertrophy, 35.5% had left ventricular dilatation and 14.8% had systolic dysfunction in ESRD patients. 4 NP singh et al (2000) had found LVH in 76.92%, diastolic dysfunction in 72% but did not find systolic dysfunction in CKD patients. 5 Zoccali et al.( 2000) had found 77% LVH, 22% systolic © JAPI • january 2014 • VOL. 62 I n t h e p r e s e n t s t u d y t h e r e wa s s t a t i s t i c a l l y significant association between the findings of 2D – Echo and lipid profile. The proportion of patients having abnormal E/A ratio was almost doubled and RWMA was six-times more in raised serum total cholesterol group as compared to normal serum cholesterol group (p value less than 0.01 and less than 0.05 respectively). These findings suggest the hyperlipidaemia increases risk of cardiovascular involvement in ESRD patients. Devasmita choudhary et al (2009) found that hyperlipidaemia is associated with rapid progression of CKD and increases cardiovascular mortality 8 (Table 3). In hypertensive patients with ESRD LVH was present in 87.5%, diastolic dysfunction was present in 72.9% as measured by abnormal E/A ratio, systolic dysfunction as measured by reduced LVEF was present in 29.2% and pericardial effusion observed in 14.6%. In normotensive patient with ESRD LVH was present in 45.5%, diastolic dysfunction was present in 40.9%, and systolic dysfunction was present in 13.6% and pericardial effusion observed in 13.6% patients. There was statistically significant association between the findings of 2D – Echo in patients having hypertension as compared to normotensive group for LVH and abnormal E/A ratio parameters (p value 0.01 and 0.05 respectively) (Table 4 and Figure 1). Levin A et al (1996) found 3% increased risk of LVH, as an increase in systolic blood pressure by 31 32 Journal of the association of physicians of india • JANUARY 2014 • VOL. 62 5 mm Hg in CKD patients. Juan M. et al (1998) had found statistically significant difference in E/A ratio, fractional shortening, and LVEF among hypertensive and normotensive patients. 9 Patrick S et al (1999) 10 had found that rise in mean arterial blood pressure was associated with increase in LVH in ESRD patients. SA Kale et al (2001) 11 had found that hypertension was identified as important risk factor for all three LV disorders LVH, diastolic dysfunction and systolic dysfunction. Systolic, diastolic and mean BP was separately and significantly associated with LV disease. References Conclusion Cardiovascular abnormalities in ESRD were observed in large no of patients and left ventricular dysfunction was the commonest cardiovascular a b n o r m a l i t y . LV H w a s t h e m o s t c o m m o n echocardiographic abnormality in ESRD cases. Diastolic function was deranged in more number of patients as compared to systolic function in patients with ESRD. Major contributing factors for left ventricular hypertrophy and diastolic dysfunction were hypertension and anaemia. Major contributing factor for systolic dysfunction was RWMA due to ischaemic heart disease. Echocardiography was more sensitive for detecting LVH and minimal pericardial effusion prior to clinical detection. 1. US Renal Data System: USRDS 2005 Annual Data Report. The National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2005 2. Wing AJ. Cardiovascular related causes of death and fate of patients with renovascular disease. Contributions to Nephrology 1984; 41:306311. 3. Silverberg JS, Sniderman AD, Barre PE, Prichard SS. Impact of left ventricular hypertrophy on survival in end stage renal disease. Kidney International 1989;36:286- 290. 4. Foley RN, Parfrey PS, Harnett JD, et al. Clinical and echocardiographic disease in patients starting end-stage renal disease therapy. Kidney Int 1995;47:186-92 5. Singh NP, Chandrashekar, M Nair. The cardiovascular and hemodynamic effects of erythropoietin in CRF. JAPI 2000;48:301-306. 6. Manish M.Sood et at. Left ventricular dysfunction in the haemodialysis population. NDT plus 2008;4:199–205 7. S agarwal, P Dangri, OP Kalra, S Rajpal. Echocardiographic assessment of cardiac dysfunction in patients of chronic renal failure. JIACM 2003;4:296-303. 8. Devasmita choudhury et al. Disorders of lipid metabolism and chronic kidney disease in the elderly. Semin Nephrol 2009;29: 610–620. 9. Juan M.et al. Blood pressure, left ventricular hypertrophy and long-term prognosis in hemodialysis patients. Kidney International 1998;54suppl.68:S-92–s-98. 10. Patrick S et al . The clinical epidemiology of cardiac disease in chronic renal failure. J Am Soc Nephrol 1999;10:1606–1615. 11. SA Kale et al. Left ventricular disorders in patients of end stage renal disease entering hemodialysis programme. Indian J Nephrol 2001;11: 12-16. Office Bearers of the Rajasthan Chapter of API 2013-2014 Chairman Elect : Dr. Girish Mathur, Kota; Chairman : Dr. L.A. Gauri, Bikaner; Immediate Past Chairman : Dr. D.C. Kumawat, Udaipur; Hon. Secretary : Dr. Sanjiv Maheshwari, Ajmer; Hon. Treasurer : Dr. R.K. Mehta, Bhilwara 32 © JAPI • january 2014 • VOL. 62 Journal of the association of physicians of india • JANUARY 2014 • VOL. 62 © JAPI • january 2014 • VOL. 62 33 33