Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
THE RELATIONSHIP BETWEEN REGIONAL INTEGRATED BACKSCATTER LEVELS
AND REGIONAL STRAIN.
J. D’hooge, F. Jamal, B. Bijnens, J. Thoen, F. Van de Werf, P. Suetens and G.R. Sutherland
Katholieke Universiteit Leuven
Medical Image Computing, Dept. of Cardiology and Dept. of Physics
U.Z. Gasthuisberg, Herestraat 49, B-3000 Leuven, Belgium
Abstract— Integrated backscatter (IB) and its cyclic
variation (CV) are echographic parameters often used
for tissue characterization. To study the origin of CV, we
correlated changes in IB with regional strain in healthy
volunteers.
Both radiofrequency (RF) and Color Doppler Myocardial Imaging (CDMI) data were acquired from 10
volunteers (parasternal long axis view, posterior wall),
using a clinical scanner at high frame rate. IB was extracted from the RF data. Regional radial strain was
calculated by integrating the strain rate (SR) curve, extracted from the velocity data. For each volunteer, 3
consecutive heart cycles were averaged. The individual
phases of the cardiac cycle (ejection, fast filling, diastasis and atrial contraction) of all datasets, were averaged.
The negative radial strain (NRS) curve was plotted on
top of the IB curve.
During all phases of the cardiac cycle, NRS paralleled IB apart from early systole, where IB increased
while NRS decreased. These results can be explained
by correlating IB to regional three-dimensional strain
(rather than just the radial component, e.g. wall thickening). Indeed, NRS results in an increase in mean scatterer spacing and hence a decrease in IB level. Moreover,
it has been shown that longitudinal contraction preceeds
the radial one. This could explain the increase in IB level
during early systole since this early longitudinal strain
could initially decrease scatterer spacing.
Changes in myocardial reflectivity as measured by
regional IB levels seem to be directly related to regional
three-dimensional strain.
I NTRODUCTION
Myocardial tissue characterization based on processing
the raw backscattered data has been investigated by many
groups in recent years [1]. The parameter extracted from the
radiofrequency (RF) data that has been studied most thoroughly is the integrated backscatter (IB). IB is calculated by
integrating the power spectrum of the received signal over
the meaningful bandwidth of the transducer, which implies
that it is a measure for the mean reflected ultrasonic energy
from a particular region of tissue.
Extensive evaluation of the properties of IB has demonstrated that its magnitude correlates with the state of the myocardial tissue and can be used to differentiate normal from
pathological myocardium. It has been shown that during
acute ischemia, the mean IB level raises. Moreover, IB exhibits a cardiac-cycle dependent variation (CV) in normal
myocardium. Typically, a variation of 3 to 5 dB is found
with a maximum at end-diastole and a minimum at endsystole [1]. Extensive clinical evaluation of CV has demonstrated that the magnitude and the timing of peak and trough
IB levels are all influenced by a wide range of disease processes. The magnitude of the CV has been shown to be
an index of contractile performance and to decrease during
acute myocardial ischemia.
However, no consensus has been reached on the origin
of this cyclic variation. Some investigators would hold that
regional anisotropy produced by local changes in both scatterer density and angle of insonation can account wholly
for the CV and its changes during ischemia and that CV is
thus simply a measure of regional changes in wall thickness
during the cardiac cycle [4]. Others would argue that CV
represents more than wall thickness changes and point to
the evidence for the return in CV in a myocardial segment
following reperfusion which precedes the return of changes
in wall thickness [5].
The original studies on IB were performed using single
crystal M-mode data acquisition at high temporal resolution. However, in order to reduce variability, several measurements had to be averaged, resulting in a loss of temporal resolution. Most subsequent studies have obtained
two-dimensional sector data, determining IB values by either off-line processing of the acquired RF signal or by online processing using dedicated hardware incorporated in
standard clinical equipment. However, all these systems acquired IB data at frame rates around 20-30 Hz at a resolution
of 6-8 bit.
Recent developments in echocardiographic equipment
enable image acquisition at high frame rates (> 100 Hz). It
has been demonstrated that IB traces extracted from these
high frame rate datasets [3] show changes corresponding
to the timing of short-lived myocardial contraction and relaxation events. Therefore, in order to understand the relationship between IB and mechanical events, we have investigated the relationship between high frame rate IB and
geometrical changes (strain) within the myocardium.
M ETHODS
Cardiac ultrasound data were acquired from 10 healthy,
male volunteers (age 28 4 years) using a clinical scanner
(GE Vingmed, System V) (parasternal long axis view, tissue
harmonics mode, 2.2 MHz transmit frequency) which enabled the continuous acquisition of the digital IQ data (the
in-phase quadrature sampled RF signal) (19 bit, 20 MHz)
within a sector angle of 20-30 at a frame rate above 170 Hz.
In order to obtain information on the precise timing of the
different phases of the cardiac cycle and in order to be able
to estimate local radial strain, corresponding Color Doppler
Myocardial Imaging (CDMI) velocity data sets were acquired at the same temporal resolution and from the same
myocardial segments immediately after acquisition of the
RF data. The ECG was digitized simultaneously.
A region of interest (' 100 mm2 ) was positioned within
the posterior mid-wall myocardial segment avoiding epicardial and endocardial reflections and a mean IB curve (obtained by averaging over 3 R-R intervals) was extracted for
each volunteer.
A mean velocity profile over one R-R interval was extracted from the CDMI data sets, for each individual, from
the same location as the position of the region of interest
used to define the IB curve. Regional radial strain was calculated by time-integrating the strain rate curve, extracted
from the velocity data as the spatial gradient in myocardial
velocities [2].
The timing of the onset and duration of ejection, fast
filling, and atrial contraction were determined based on the
velocity data sets. These were used to average the interindividual IB and strain curves: each part of the IB and
strain curve corresponding to a specific phase of the cardiac
cycle was interpolated to have the same number of samples
for all volunteers and was normalized and averaged over the
number of volunteers. The mean IB level and the average
CV and strain values were calculated from all volunteers
and used to rescale the average (normalized) IB and strain
curve. In this way, the mean behavior of the IB and strain
curve during each phase of the cardiac cycle was obtained.
Finally, these partial curves were merged in order to obtain
one representative average heart cycle.
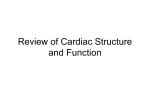
(a)
(b)
Figure 1: IB curve of one volunteer averaged over 3 R-R
intervals (a) and its corresponding velocity profile (b). Specific phases are defined on the velocity curves (Isovolumetric Contraction (IVC), Ejection (E), Isovolumetric Relaxation (IVR), Fast Filling (FF), Diastasis (D), Atrial Contraction (AC)) and also indicated on the IB curves.
R ESULTS
Figure 1 (a) shows a typical example of a single R-R interval, high frame rate IB curve taken from a left ventricular
posterior mid-wall segment obtained from one of the normal volunteers together with the corresponding CDMI velocity data set (b). The different phases of the cardiac cycle
(Isovolumetric contraction (IVC), ejection (E), isovolumetric relaxation (IVR), fast filling (FF), diastasis (D) and atrial
contraction (AC)) can clearly be identified on the velocity
curve. However, because the onset and duration of the isovolumetric phases is not always clearly identifiable on the
velocity curves, only the beginning of E, FF and AC and the
end of FF and AC were indicated and used for the analysis
of the corresponding IB curves (indicated as vertical lines).
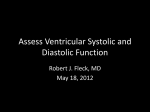
(a)
(b)
Figure 2: Overall mean IB curve standard deviation acquired at high frame rate (a) and the overall average radial
strain profile standard deviation (b) for a posterior midwall segment in a parasternal long axis view.
Figure 2 shows the overall mean IB curve (a) and the
corresponding average strain curve extracted from the CDMI
velocity data (b) for all normal volunteers, together with
their standard deviation. Dashed vertical lines are again delineating the onset of the specific cardiac mechanical events.
The IB value decreases rapidly during mid to late systole
after a short marked increase in early systole. The minimum
IB level was found shortly after end systole (just before the
onset of FF). IB levels then increased rapidly during fast fill-
ing to reach their end-diastolic value around mid-diastasis
after a small over- and undershoot. They then increased
further during ventricular filling due to atrial contraction.
During the isovolumetric contraction and relaxation periods, some curves showed a variable increase and some a
transient short-lived decrease in IB level. The mean IB level
was 49.2 dB and the mean CV 8.9 dB.
The average radial strain curve increased continuously
during systole to reach its maximal value of 44 % at endsystole. Strain values then returned to zero during fast filling of the ventricle and remained constant during diastasis.
Finally, a marked decrease was observed during atrial contraction.
Figure 3: Mean integrated backscatter levels (solid) and
mean negative strain curve (dashed) for one human cardiac
cycle.
In order to make comparison between IB and strain behavior easier, the same average IB curve and the average
negative radial strain curve were plotted on top of each other
in Figure 3. During all phases of the cardiac cycle, negative
radial strain paralleled IB apart from early systole, where IB
increased while negative radial strain decreased.
D ISCUSSION
The IB curves obtained using high frame rate acquisition show a maximum level in the beginning of systole followed by a pronounced decrease with a minimum near endsystole. This is more or less in keeping with the prior findings of other investigators who acquired data at a relatively
low temporal resolution. However, the increase in the rate
of acquisition of the IB samples to 195 Hz resulted in the
delineation of a more complex IB curve with multiple, reproducible peaks and troughs occurring during the cardiac
cycle. Since these peaks and troughs were highly reproducible over a range of different heart cycles in all volunteers, these high frequency changes could not be explained
by measurement noise or by the positioning of the regions
of interest and appeared to be temporally related to specific
mechanical events during the heart cycle.
The average CV was 8.9 dB. This was higher than the
values reported in other studies. This was most likely caused
by the fact that CV was calculated as the difference between
maximal and minimal value occurring during the cardiac
cycle, which were better resolved due to the high temporal
resolution. Although other methods have been described to
calculate CV, they seemed not relevant for the interpretation
of the results found in this study.
Relating the regional IB changes to the concomitant regional velocity profiles enabled the definition of the temporal relationship between local changes in IB levels and the
different phases of the cardiac cycle. The rapid onset of motion induced by myocardial contraction was associated with
an initial increase in reflectivity. This was immediately followed by a progressive decrease in reflectivity during mid to
late systole which reached a minimum around end-systole.
The onset of fast filling was associated with a rapid progressive increase in reflectivity which returned to base-line (enddiastolic) value at mid-diastasis after a small over- and undershoot. Then there was a further clear increase occurring
during passive ventricular filling due to atrial contraction.
Although this increase was less pronounced in the overall
average of the volunteers traces, it could clearly be observed
in some of the individual traces (cf. Figure 1). This variability in young normals is likely to be explained by the fact
that this increase is relatively small and thus will only be
observed in very echogenic individuals.
Extracting the local radial strain from the regional Myocardial Doppler velocity profiles showed a continuous increase in radial strain during the whole of systole, reflecting
the thickening of the myocardial wall during contraction.
The onset of relaxation was associated with a return of the
radial strain to zero, i.e. wall thickness returned to its initial
value. Finally, during atrial contraction the wall thinned due
to the increasing pressure in the left ventricle, showing as a
decrease in radial strain.
Relating the changes in IB to the changes in radial strain
suggests that IB changes during the cardiac cycle are directly related to re-positioning of the scatterers due to local myocardial strain associated with the regional pattern of
myocardial contraction.
This hypothesis is based on the fact that IB changed not
only during active contraction but also during passive compression (during atrial contraction) of the posterior wall.
Such passive changes in reflectivity are probably not associated with changes in acoustic properties of the scatterers
and thus are probably related to changes in scatterer concentration. This would strongly support the hypothesis that IB
is directly related to wall thickness as suggested by other investigators [4]. Indeed, the amount of scatterers within one
resolution cell of the imaging system could decrease with
increasing wall thickness as the same amount of scatterers
is distributed over a larger volume (i.e. a thicker wall). As
a result, less energy is scattered within the resolution cell,
which implies that IB levels decrease with increasing wall
thickness. This hypothesis also fits with the behavior of
the IB curve during fast filling and during atrial contraction,
where wall thinning is related to an increase in IB level.
However, the results in the volunteers showed a marked
increase in reflectivity in early systole which was, according
to the concomitant radial strain curve, not associated with
myocardial thinning. Thus, perhaps a better explanation
for the behavior of the IB curves is obtained by relating IB
changes to local, three-dimensional strain rather than to wall
thickening. Since wall thickening represents one component of the strain vector (the radial component), the behavior of the IB levels during contraction, fast filling and atrial
contraction can be explained as described above. However,
the initial increase in IB is perhaps explained by the fact
that the contraction of a volume of myocardium is a threedimensional process. As a consequence, local scatterer density could be increased during early systole due to the normal, early longitudinal contraction of the myocardium (resulting in longitudinal strain), which would decrease the
longitudinal distance between scatterers, thus increasing the
IB level. Subsequently, the delayed radial contraction (i.e.
radial strain) would increase mean scatterer spacing and thus
decrease the IB level. This contraction process and how it
could relate to scatterer distribution (and hence IB levels)
is schematically illustrated in Figure 4. Similarly, the elastic recoil observed in the IB curve but absent in the radial
strain curve could be explained by the fact that this recoil is
predominantly in the longitudinal direction.
ers, oriented approximately longitudinally, contract before
the mid-myocardial layers (oriented approximately circumferentially) because of their earlier depolarization.
If IB levels are indeed related to mean scatterer spacing, this could imply that the predominant scatterers within
the myocardium are the extra-cellular collagen fibers (as
suggested by other investigators). Indeed, during systole,
mass within the myocardium will re-distribute according to
the stress within the wall. At the beginning of contraction,
capillaries and arterioles are pushed closed since the blood
contained within them can relatively easily be pushed away.
This implies that during early systole myocardial cells move
closer together and thus the surrounding collagen fibers as
well. Then, as no more space is available and contraction
continues, the wall thickens and collagen fibers are pulled
along, resulting in an increase in the mean distance between
fibers.
C ONCLUSION
This study shows that increasing the rate of real time
RF data acquisition results in a more complex, reproducible
IB curve. The resolved maxima and minima in IB levels
are related to specific phases of the myocardial contraction.
The high frame rate curves suggest that changes in IB levels are directly related to local, three-dimensional strain and
as a consequence, only indirectly related to wall thickening. If this hypothesis holds true than the role of IB in myocardial tissue characterization becomes questionable since
modern techniques enable to estimate (three-dimensional)
strain more directly.
ACKNOWLEDGEMENTS
This work was supported by the Flemish Institute for
the Improvement of the Scientific-Technological Research
in the Industry (IWT).
R EFERENCES
[1] Perez JE, Dávila-Román VG, Miller JG, “Assessment of myocardial viability by ultrasonic tissue characterization”, Coronary Artery
Disease, 6(8):613–618, 1995.
Figure 4: Contraction of the posterior wall. The scatterers
just before systole (left) will be re-organized. In early systole, longitudinal strain is dominant resulting in increase in
scatterer density (middle). In mid-late systole radial strain
is more important (right), having the opposite effect.
Since the total radial strain is larger than the total longitudinal strain (approximately 30% vs. 15%), the combined effect of longitudinal and radial strain will result in
an overall increased mean scatterer spacing and hence a decreased IB level. Moreover, the delayed radial strain in the
posterior wall has been described and might in part be explained by the fact that the sub-endocardial myocardial lay-
[2] Heimdal A, Stylen A, Torp H, Skjaerpe T, “Real-time strain rate
imaging of the left ventricle by ultrasound”, The Journal of the American Society of Echocardiography, 11(11):1013–1019, 1999.
[3] Bijnens B, D’hooge J, Pislaru C, Pislaru S, Kirkhorn J, Herregods
MC, Angermann C, Suetens P, Van de Werf F, Sutherland G, “High
frame rate Integrated Backscatter in normal canine myocardium”,
Circulation,98(Supplement):I642, 1998
[4] Rijsterborgh H, Mastik F, Lancee CT, Van der Steen AFW, Sassen
LMA, Verdouw PD, Roelandt J, Bom N, “Ultrasonic Myocardial
Integrated Backscatter and Myocardial Wall Thickness in Animal
Experiments”, Ultrasound in Medecine and Biology, 16(1):29–36,
1990.
[5] Milunski M, Mohr GA, Wear KA, Sobel BE, Miller JG, Wickline
SA, “Early Identification With Ultrasonic Integrated Backscatter of
Viable But Stunned Myocardium in Dogs”, Journal of the American
College of Cardiology, 14(2):462–471, 1989.