Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
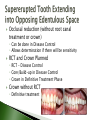
ODRP 726 Patient Diagnosis and Treatment Planning Many times the treatment plan will be fairly uncomplicated ◦ No periodontal disease with poor prognosis for any teeth ◦ No teeth where restorability is in question The finalized treatment plan will contain all treatment procedures The dentist is sure that there will only be minor changes in treatment plan Often a patient’s treatment includes much uncertainty Patients want to know all that will be involved in rehabilitating their oral condition Too much unpredictability is involved to finalize overall treatment plan when extensive problems are involved ◦ ◦ ◦ ◦ Which teeth are restorable? Which teeth will need endodontic treatment? Will periodontal treatment be successful? Will the patient commit to perio surgery if needed? Disease Control Phase Definitive Unknown restorability Phase Unknown endo needs Unknown perio outcomes Disease control only Changes in Tx Plan + Chances for Patient Confusion Disease Control Phase Definitive Unknown restorability Phase Unknown endo needs Unknown perio outcomes All phases can be included Changes in Tx Plan + Chances for Patient Confusion Design a disease-control-only plan ◦ Improves unpredictability by controlling variables such as periodontal disease and rampant caries simplifying the situation by extracting hopeless teeth. ◦ Provisional replacements for missing teeth may be fabricated for interim esthetics and function In some cases design a disease-control treatment plan plus tentative definitive treatment plan. Tentative definitive plan ◦ Discuss the possible treatment outcomes ◦ Important to have a tentative definitive plan to identify key teeth when tooth supported denture is considered ◦ A post-treatment assessment is performed at the end of disease control phase to evaluate: Level of disease resolution (Perio re-eval) Patient compliance Patient desire for further care ◦ Options: Maintain the patient at current state Design definitive phase treatment plan Control active oral disease and infection Stop occlusal and esthetic deterioration Manage risk factors Periodontal therapy, endodontic therapy, extractions, operative treatment to eradicate caries Particularly valuable when the dentist is uncertain about: ◦ Disease severity ◦ Outcome of disease control ◦ Patient commitment to treatment Some teeth may receive only palliative treatment – until perio treatment is complete Patient may enter a holding period and not proceed to definitive disease Consider all reasonable treatment options Discussion with patient to reach a consensus on objectives Dentist helps the patient: ◦ Set achievable treatment goals ◦ Build realistic expectations for treatment outcomes Establish clear, specific, quantifiable standards for success (outcomes measures) ◦ Target plaque score ◦ Target bleeding score Specify the factors to be evaluated at the post treatment assessment ◦ Plaque and bleeding score ◦ Status of periodontal disease and need for surgery ◦ Need for endo/crown Delineate the steps to be implemented when the patient does or does NOT meet the standards for success 68 yr old Caucasian female “Wants a prettier smile No pain All teeth are mobile, maxillary Class II and III Recurrent decay #3 – replace crown Recurrent decay #12 – place crown Patient would like to keep as many teeth as possible Should we prepare a comprehensive treatment plan or just the Disease Control Phase? When would it be helpful to treatment plan only the Disease Control Phase? ◦ Uncertain about disease severity ◦ Uncertain about the outcome of disease control ◦ Uncertain about the patient’s commitment to treatment 68 yr old Caucasian female “Wants a prettier smile” No pain All teeth are mobile, maxillary Class II and III Recurrent decay #3 – replace crown Recurrent decay #12 – place crown Patient would like to keep as many teeth as possible What are all the treatment options? What are realistic expectations for treatment outcomes? What could be quantifiable standards for success post disease control phase? Address the patient’s Chief Complaint as quickly as possible, insuring that this will not conflict with the primary goals of the disease control phase ◦ Example: Patient just had # 8 extracted and has returned for a comprehensive treatment plan. The patient has moderate periodontal disease and multiple Class II cavities. ◦ CC: replace #8 with an implant. What would you treat first? Sequence by Priority ◦ Treat the most severe and urgent needs first ◦ Example: Moderately large asymptomatic cavity on vital tooth Amalgam or composite restoration Large cavity with asymptomatic necrotic pulp Root canal tx and crown Grossly decayed, asymptomatic, non-restorable tooth Extraction ◦ Which would you treat first? Sequence by quadrant or sextant It is most efficient and productive to restore all carious teeth in the same area at the same time Integration of periodontal therapy Should perio therapy always come first in disease control? What takes priority over periodontal treatment? ◦ Treatment of deep caries in vital teeth ◦ Symptomatic pulpal problems ◦ Acute oral infections Keep definitive phase options open with minimalist treatment in the disease control phase. ◦ Key teeth ◦ Other teeth that might be salvageable but uncertainty if it is feasible or desirable for the patient to expend the resources to restore them definitively Minimalist treatment ◦ ◦ ◦ ◦ Provisional restorations rather than crowns Pulp-capping rather than RCT initiation Pulpectomy/pulpotomy rather than definitive RCT Exception: Definitive direct-fill restorations are preferred over temporary fillings Overall management 1. Comprehensive caries diagnosis 2. Assessment of caries risk 3. Basic caries intervention protocol for patients with active lesions or those who are at risk for developing new lesions 4. Supplemental caries intervention protocol to address specific needs of those requiring additional measures or the patient who remains caries active 5. Maintenance and re-evaluation at appropriate intervals to identify new lesions and re-evaluate the risk for future caries activity Individual restoration of cavities Use of sealants or conservative composite restorations to prevent, control new or incipient lesions Dietary and/or behavioral approaches to prevent new caries Use of fluoride and/or MI Paste to strengthen the tooth Elimination of plaque Caries control protocol is for individuals: ◦ With moderate or high rate of caries formation ◦ Who are at significant risk for developing caries in the future Comprehensive, organized plan designed to: ◦ Arrest or remineralize early carious lesions ◦ Eradicate overt carious lesions ◦ Prevent the formation of new lesions Can be stabilized and controlled May be inactivated for a period of time In a predisposed patient, the possibility of reactivation persists The patient with periodontal disease can be expected to require some sort of therapy for as long as they have teeth. The PATIENT has a great deal to do with how long they have teeth Chronic disease Systemic considerations Lessening the force or intensity ◦ Identification and mitigation of diseases, treatments or medication regimens that might Promote periodontal disease Delay healing Interfere with periodontal therapy ◦ Identification of patients who require antibiotic prophylaxis Risk of endocarditis Risk of artificial joint infection ◦ Determination if antibiotics are contraindicated ◦ Obtain physician’s clearance for invasive treatment Oral self-care instructions ◦ Demonstration of brushing and flossing techniques ◦ Provide additional oral health care aids and instruction ◦ Training is imperative ◦ Implementation – can the patient manage the tools correctly? ◦ Support virginiagarberding.authorweblog.com Extraction of hopeless teeth ◦ Severe periodontal disease ◦ Severe decay or fracture ◦ For prosthodontic reasons Tooth will not be functional Tooth is poorly positioned ◦ Extraction may be delayed To preserve appearance To prevent collapse of VDO dental--health.com Of or related to medical examination or treatment Elimination of iatrogenic restorations and open carious lesions contributing to periodontal disease – complete BEFORE scaling and root planing Open margins Open contacts Overhangs Poor contours ◦ S & RP will be more effective ◦ Patient’s oral self-care efforts are more effective ◦ Tissues heal more quickly and completely ◦ The interim evaluation can be complete and definitive ◦ Determine the cause of sensitivity (pulpal or dentinal) Manage other dental problems that contribute to periodontal disease ◦ Acute occlusal trauma from significant occlusal interferences Scaling and Root Planing ◦ Is a technically challenging procedure that takes patience, persistence and skill ◦ IT TAKES TIME ◦ Educate the patient about the challenge of the procedure and it’s value ◦ If in doubt, use anesthesia The patient will be more comfortable and you will be more comfortable. It allows you to do the job more thoroughly than without it. Scaling and Root Planing ◦ It is better to perform a thorough scaling and root planing on a smaller area than to scale a larger area superficially – you will usually have to come back and rescale ◦ When patients are late, do not try to provide the entire procedure scheduled Rewards the patient for being late Very frustrating to do an optimal job in a sub-optimal amount of time ◦ Sometimes you can’t get all the calculus without a surgical flap Pharmacotherapy ◦ Chlorhexidine Reduces plaque, gingival inflammation and bleeding Selected conditions Acute conditions – acute necrotizing ulcerative gingivitis Disabled patients with difficulty with OHC Immunocompromising conditions Severely debilitating systemic disease Overt residual gingival inflammation and bleeding after scaling and root planing ◦ Systemic antibiotic therapy ◦ Site-specific antibiotics When a few isolated deep pockets have been unresponsive to initial S and RP Post-Initial Therapy Evaluation (Perio Re-Eval) ◦ 6-8 weeks after the completion of SRP The patient should have effective hygiene program ◦ ◦ ◦ ◦ ◦ Review the health history Complete re-evaluate of the gingival condition Compare with the pre-treatment evaluation Determine the effectiveness of treatment Develop plan for future periodontal therapy Interval until maintenance visit Perio surgery Should definitive treatment phase begin In the disease control phase there are three options: 1. Irreversibly compromised tooth • Root canal treatment • Provisional restoration of tooth – usually with foundation restoration (core build-up, post and core) 2. Initial restorative treatment for conditions, which may if untreated lead to loss of pulp vitality • Decay, fractured teeth, recurrent decay, missing restorations 3. Opportunity for conservative pulp treatment (direct or indirect pulp capping) with definitive diagnosis following Thorough evaluation of the tooth and periapical areas (endodontic testing) is important before restoring the tooth dentistrytoday.com intelligentdental.com Healthy Pulp or Reversible Pulpitis ◦ Caries, fracture or defect is of moderate depth and the pulp is not exposed Treatments ◦ Direct-fill restoration Base or liner is usually not warrented ◦ Adhesive material (glass-ionomer cement or resin hybrid) can be used as “bandage” When time does not permit permanent restoration Allows confirmation of pulp health Necessitates future visit to for final restoration Healthy Pulp and Periapical Area or Reversible Pulpitis ◦ Caries, fracture or defect is in close proximity to the pulp Two schools of thought 1. Total caries removal and final form preparation. If the pulp is encountered in this process, extraction or root canal treatment are recommended. Compromised pulp = likelihood of necrosis Force the issue – do RCT Better sooner than later – calcified canals less likely and outcome more predictable. Two schools of thought 2. Additional caries removal and preparation should be minimal and should avoid areas where pulpal encroachment is likely, even if affected dentin remains between the indirect pulp capping material and the pulp. The pulp has a reasonable likelihood of survival Indirect pulp cap has generally favorable prognosis If successful, root canal therapy or extraction is avoided If unsuccessful, root canal therapy can still be attempted, although with slightly poorer prognosis dentalindia.com dentaljuce.com Sometimes go for the RCT ◦ Key tooth is involved and the overall prognosis depends on it’s retention ◦ It is imperative to do the root canal, if needed, before restoration of the tooth Sometimes use the pulp-cap ◦ Patient is unwilling or unable to accept root canal treatment if necessary, and the tooth would have to be extracted Sometimes either ◦ Engage the patient in a discussion with benefits and risks involved with each. Reversible Pulpitis or a Healthy Pulp and Healthy Periapical Area ◦ The pulp is exposed. Treatment options ◦ Direct pulp cap is indicated: Small mechanical pulp exposures Tooth with healthy pulp and periapical area Tooth is treatment planned for direct fill intracoronal restoration Larger mechanical or carious pulp exposure Patient cannot decide on a path of treatment Tooth is to be extracted at a future date Establish time frame and emphasize future problems ◦ Informed consent if very important ◦ The tooth should be monitored indefinitely Irreversible Pulpitis or Necrotic Pulp ◦ Definitive treatment is required! Extraction or root canal therapy Pulp capping is contraindicated Pulpotomy or Partial pulpectomy should ONLY be considered if the doctor cannot execute a complete pulpectomy or extraction. The patient must understand that this is NOT definitive treatment. kokkinosmileclinic.com “Baby” root canal contempclindent.org smilewinnipeg.dentistryonline.com “Mini root canal” First step of the root canal procedure saugusdental.com Patient DECLINES treatment for Asymptomatic Apical Periodontitis, Cyst or Granuloma ◦ If the patient is immunocompromised, allowing chronic apical infection to persist is inappropriate and unacceptable ◦ If the patient has normal host response, it is appropriate to re-evaluate the lesion at specified periods to determine if the lesion increases in size. Tooth (no RCT is necessary) Tooth – crown required ◦ Direct fill restoration ◦ Core or crown build-up (direct-fill material) is placed in the Disease Control Phase, the crown in Definitive Phase Substructure for the crown Interim (temporary) restoration Tooth – compelling esthetic concern Tooth having received root canal treatment ◦ Crown may be placed in disease control phase ◦ An effective seal between oral cavity and root canal filling is required ◦ Direct-fill core/build-up is placed ◦ Provisional post and core ◦ Definitive post and core Occlusal reduction (without root canal treatment or crown) ◦ Can be done in Disease Control ◦ Allows determination if there will be sensitivity RCT and Crown Planned ◦ RCT - Disease Control ◦ Core/Build-up in Disease Control ◦ Crown in Definitive Treatment Phase Crown without RCT ◦ Definitive treatment Exposure and forced eruption ◦ Begin as early as possible to determine the outcome by the time definitive treatment begins Extraction ◦ Disease control – so definitive treatment is not delayed search.wn.com periodontist.org