Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Fundus photography wikipedia , lookup
Corrective lens wikipedia , lookup
Photoreceptor cell wikipedia , lookup
Keratoconus wikipedia , lookup
Cataract surgery wikipedia , lookup
Dry eye syndrome wikipedia , lookup
Corneal transplantation wikipedia , lookup
Contact lens wikipedia , lookup
Eyeglass prescription wikipedia , lookup
Retinitis pigmentosa wikipedia , lookup
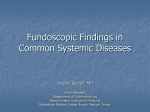
1206 Invest. Ophthahnol. Visual Sci. December 1978 Reports threshold may be a useful indicator of determining when the process of adaption to contact lenses is complete. Two of the subjects returned to baseline sensitivity after discontinuing lens wear overnight, while one subject required 1 week to regain original threshold levels. Although none of these subjects developed corneal edema or any other adverse signs during lens wear, there apparently are some individual factors which may prolong the corneal desensitization process long after lens wear is discontinued. From the School of Optometry, University of California, Berkeley, Calif. This study was supported in part by U.S.P.H.S. Grant R01 EY01755-02. Submitted for publication July 7, 1978. Reprint requests: Dr. Kenneth A. Poise, School of Optometry, University of California, Berkeley, Calif. 94720. Key words: corneal touch threshold, corneal sensitivity, comeal swelling, corneal thickness REFERENCES 1. Byron, H. M., and Wesley, A. C : Clinical investigation of comeal contact lenses, Am. J. Ophthalmol. 51:675, 1961. 2. Dixon, J. M.: Ocular changes due to contact lenses, Am. J. Ophthalmol. 58:424, 1964. 3. Ko, L. S., and Tomiyama, S. K.: The influence of contact lens application on the corneal sensitivity, Trans. Ophthalmol. Soc. 2:1, 1963. 4. Larke, J. A., and Sabell, A. G.: A comparative study of the ocular response to two forms of contact lenses, The Optician 162:10, 1971. 5. Millodot, M.: Effect of hard contact lenses on corneal thickness, The Contact Lens 1:5, 1967. 6. Millodot, M.: Effect of the length of wear of contact lenses on corneal sensitivity, Acta Ophthalmol. 54:721, 1976. 7. Cochet, P., and Bonnet, R.: L'esthesiometrie corneene, Realisation et interet pratique, Bull. Soc. Ophtalmol. Fr. 61(7 - 8):541, 1961. 8. Millodot, M.: Studies on the sensitivity of the cornea, Optician 157(4067):267, 1969. 9. Millodot, M.: Objective measurement of corneal sensitivity, Acta Ophthalmol. 51(3):325, 1973. 10. Mandell, R. B., and Poise, K. A.: Keratoconus: Spatial variation of corneal thickness as a diagnostic test, Arch. Ophthalmol. 82:182, 1969. Vitreous fluorophotometry evaluation of xenon photocoagulation. JAMES M. NOTH, CHARLES VYGANTAS, AND JOSE G. F. CUN- HA-VAZ.* An abnormal increase in the permeability of the outer blood-retinal barrier was induced in the eyes of adult pigmented rabbits after retiiial xenon arc photocoagulation. The alteration of the blood-retinal barrier, which was assessed by vitreous fluorophotometry after systemic administration of sodium fluorescein, followed a welldefined pattern. Higher values, which were recorded during the first three days after photocoagulation, recovered progressively afterward. The permeability of the blood-retinal barrier returned to near-normal levels between 10 and 14 days after photocoagulation. A direct correlation was observed between higher initial values and heavier photocoagulation. A variety of retinal diseases (vascular retinopathies and macular disorders) associated with breakdown of the blood-retinal barrier are, at some time in their evolution, treated by photocoagulation. This appears to be somewhat contradictory, in that photocoagulation has been shown by fluorescein angiography and histologic studies using a variety of tracer materials1 to induce a breakdown of the blood-retinal barrier. Further studies were needed to measure the degree of the alteration of the blood-retinal barrier induced by xenon photocoagulation and its recovery to normal levels. The availability of vitreous fluorophotometry,2 a new quantitative method of fluorescein analysis of the vitreous that permits the detection of very small amounts of fluorescein penetrating into the vitreous through an altered blood-retinal barrier, enabled us to measure at different intervals the alteration of the blood-retinal barrier after xenon arc photocoagulation. Material and methods. Adult pigmented rabbits, principally of the Dutch strain, were used as the experimental animals. Xenon photocoagulation. Xenon photocoagulation was applied to 11 eyes of seven animals. Before treatment all eyes were subjected to ophthalmoscopic examination and fundus photography. Photocoagulation (Zeiss) with the xenon arc lamp (XBO-2007 Osram), using a 4.5° cone size was selected for all burns. General anesthesia was given to all animals in an ultramuscular injection of acepromazine and ketamine. Xenon photocoagulation was applied to the posterior pole of the eye in an area immediately inferior to the region of the myelinated nerve fibers. A total of 20 burns were applied to each eye. Although difficult, an attempt was made to evaluate the intensity of the retinal burns by following the system of grading proposed by Tso et al.3 Five eyes received predominantly grade I photocoagulations, whereas the other six eyes had heavier grade II and III retinal burns inflicted to their retinas. At the time of the sacrifice, the eyes were enucleated and the retinas were laid flat on slides. The photocoagulated area 0146-0404/78/121206+04$00.40/0 © 1978 Assoc. for Res. in Vis. and Ophthal., Inc. Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017 Volume 17 Number 12 was then measured and its size compared with that of the entire retina. Vitreous fluorophotometry. The permeability of the blood-retinal barrier was assessed by vitreous fluorophotometry before photocoagulation and at 1, 3, 7, 10, 14, and 21 days afterward. The apparatus and techniques have been previously described.2 In this study, a fiberoptic probe 450 /am in size was used. The posterior pole of the eye, immediately inferior to the myelinated nerve fiber, was selected for starting the recordings. The recordings from the retina to the lens were divided into three equal parts, which were ascribed to posterior, middle, and anterior vitreous. To calculate the blood-retinal barrier permeability, a method previously reported was followed.4 The geometry of the rabbit's eye, a curved lens surface placed 6 to 7 mm from the spherical retina of 8 mm radius, leads to a difficult computation. For the present purpose two simple approximations were used between which the true condition might be expected to fall. In one, the retina and lens were taken as large plane sheets 6.5 mm apart, and in the other, the retina was assumed to be a complete sphere 6.5 mm in radius. The distributions at any time, corresponding to these approximations, can be interpolated between the examples plotted by Crank,5 which give curves of D(C0-C) (Foa) plotted against r/a for different values of Dt/a2. D is the rate of movement of fluorescein through the vitreous, 6 X 10"6 cnWsec, (Co-C) is the concentration of fluorescein at the retinal surface, Co is background fluorescence, a — 0.65 cm, t, = 3600 sec, and Fo is the rate of fluorescein penetration over unit area of surface. The value of the retinal permeability is then given by the ratio F0/Cp, where Cp is the free concentration of fluorescein in blood (approximately 25% of the total concentration of fluorescein in the blood). Samples of blood, taken from a cut in the marginal ear vein, were placed in a 10 /nl "Microcap" pipette and discharged without centrifugation into a convenient volume of saline. Readings were taken in the supernatant when the cells had sedimented or been centrifuged down. The blood was sampled from the vein on the opposite side 1 hour after the intravenous injection of 1 ml of 10% sodium fluorescein at the time of the vitreous fluorophotometry recordings. Controls. All eyes were examined by vitreous fluorophotometry before application of xenon photocoagulation. Furthermore, three eyes from three different rabbits were not subjected to treatment and were similarly examined by vitre- Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017 Reports 1207 Table I. Blood-retinal barrier permeability after heavy xenon photocoagulation* Days after xenon photocoagulation Rabbit eye No. 2 3 4 6 8 Mean SD 10 28.0 25.0 15.0 28.0 14.0 15.0 20.8 ±6.8 23.0 20.0 22.0 16.0 7.5 22.0 23.0 16.0 19.0 13.6 8.0 15.0 13.5 20.7 ±3.2 ±4.9 14 21 10.0 5.0 Bt 8.5 6.5 6.5 5.5 6.0 7.1 4.5 B B B B B B B B B ±1.8 4 Values are X 10~ cm/hr. * Heavy xenon photocoagulation consisted of 20 retinal bums of predominantly grades II and III intensity. t Background values in the vitreous. Table II. Blood-retinal barrier permeability after minimal xenon photocoagulation* eye No. 5 7 9 10 11 Mean SD Days after xenon photocoagulation 1 7 10 14 8.5 5.0 7.5 9.0 8.0 7.6 Bt B B B B B B B 9.5 8.5 8.3 7.5 6.5 8.1 ±1.2 3 11.0 12.0 19.0 11.0 9.5 14.5 ±5.6 4.0 3.5 ±1.6 Values are x 10"4 cm/hr. •Minimal xenon photocoagulation consisted of 20 retinal burns of predominantly grade I intensity. t Background values in the vitreous. ous fluorophotometry at intervals of 1, 3, 7, 10, 14, and 21 days after photocoagulation of the contralateral eye. Results. In the control eyes, penetration of fluorescein across the retinal surface was not detectable. Our measurements showed that the level of the vitreous body remained well below 10~8 gm/ml, whereas the free fluorescein in the blood reached initial values of about 10"4 gm/ml. These data suggested an inward permeability no greater than 10~5 cm/hr. When a series of 20 xenon photocoagulations were applied over an area of approximately one sixth of the entire retina, fluorescein penetrated into the eye after an intravenous injection of the dye. The entry pattern was similar in every eye. The profile of the concentration within the vitreous body conformed approximately to that which would be expected if the dye were liberated at the retinal surface at a constant rate, diffused through the vitreous humor at the rate of movement found in free solution (6 X 10~6 cm2/ sec), and met a barrier to further progress at the 1208 Invest. Ophthalmol. Visual Sci. December 1978 Reports l/sw 2624- o 22ro 20- o Lighter photocoagulation c 18- • Heavier o </> 16- X <D 1412- tor O u. 108- % 6- Q> E 42-7 77^)7/7/^77/7; 10 14 Days Fig. 1. Permeability of the blood-retinal barrier for fluorescein after xenon photocoagulation. lens surface.4 Values of retinal permeability were obtained at 1, 3, 7, 10, 14, and 21 days after photocoagulation (Tables I and II). The results showed a direct correlation between the breakdown of the blood-retinal barrier and the intensity of the photocoagulation burns. Rabbit eyes that received lighter retinal burns showed much lower values of retinal permeability when compared with the eyes that had heavier photocoagulation burns (Fig. 1). In both groups of eyes, however, the breakdown of the blood-retinal barrier followed a similar course. After an initial increase in the retinal permeability, which remained high during the first three days after photocoagulation, there was a similar progressive decline. The blood-retinal barrier recovered to near normal values 14 days after heavier photocoagulation and only 10 days after grade I lesions were predominantly applied to the retina. Discussion. Our results show that after xenon photocoagulation of the retina there is an abnormal increase in the permeability of the bloodretinal barrier. This alteration of the blood-retinal barrier follows a well-defined pattern. Higher values that were demonstrated during the first 3 days after photocoagulation recovered progressively afterward. The permeability of the blood-retinal barrier returned to near-normal levels in the period between 10 and 14 days after photocoagulation. A direct correlation between higher initial values and heavier photocoagulation was observed. The permeability of the blood-retinal barrier reached, after heavy photocogulation, very high values (approximately 2 X 10~3 cm/hr). These Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017 were much higher than the values registered previously after competitive inhibition of the active transport for fluorescein and other organic anions.4 This finding is even more significant in that only approximately one sixth of the retina was treated by photocoagulation, and the measurements of the retinal permeability were made for the entire retina and vitreous. The abnormal increase in the permeability of the blood-retinal barrier may, under certain circumstances, be considered useful for therapeutic purposes. A few reports in the ophthalmic literature have indicated that a breakdown of the blood-retinal barrier induced either by cryoapplications or photocoagulation can significantly increase the concentration in the vitreous of intravenously administered drugs.6 The fact that the recovery of the barrier becomes almost complete by 10 days favors its use only for short-term periods of treatment. The anatomic substrate of the recovery of the outer blood-retinal barrier after xenon photocoagulation is still, however, a matter for discussion. In the rabbit, the reparative tissue is composed mainly of cells from the retinal pigment epithelium. The degree of reconstitution of the tight junctions in this newly formed epithelial layer, however, remains to be further clarified.7 At present we are undertaking an electron microscopic examination of the eyes used in our study. We expect that the findings will contribute to the understanding of the cellular mechanisms involved in the recovery of the blood-retinal barrier after breakdown. Recovery of the permeability of the blood-retinal barrier to normal values Volume 17 Number 12 Reports after photocoagulation is supported by clinical experience. Photocoagulation in central serous chorioretinopathy, for instance, is considered to have a "sealing" effect upon the characteristic fluorescein leakage. Finally, vitreous fluorophotometry may serve as a clinical tool in evaluating the final effect of a photocoagulation treatment. We thank Ms. Maxine Gere for editorial assistance and Ms. Patricia Watkins for secretarial help. From the Department of Ophthalmology, University of Illinois Eye and Ear Infirmary, Chicago, 111. *Professor of Ophthalmology, Clinica Oftalmologica, Universidade de Coimbra, Coimbra, Portugal. International research scholar of Research to Prevent Blindness, Inc., and Visiting Professor of Ophthalmology, University of Illinois Eye and Ear Infirmary, Chicago. Submitted for publication May 8, 1978. Reprint requests: Dr. Jose Cunha-Vaz, Department of Ophthalmology, University of Illinois Eye and Ear Infirmary, 1855 W. Taylor St., Chicago, 111. 60612. Key words: vitreous fluorophotometry, xenon photocoagulation, blood-retinal barrier, retinal pigment epithelium, permeability REFERENCES 1. Peyman, G. A., and Bok, D.: Peroxidase diffusion in the normal and laser-coagulated primate retina, INVEST. OPHTHALMOL. 11:35, 1972. 2. Cunha-Vaz, J. C , Abreu, J. R. F., Campos, A. J., and Figo, G.: Early breakdown of the blood-retinal barrier in diabetes, Br. J. Ophthalmol. 59:649, 1975. 3. Tso, M. O. M., Wallow, I. H. L., and Elgin, S.: Experimental photocoagulation of the human retina: I. Correlation of physical, clinical and pathologic data, Arch. Ophthalmol.95:1035, 1977. 4. Cunha-Vaz, J. G., and Maurice, D. M.: The active transport of fluorescein by the retinal vessels and retina, J. Physiol. 191:467, 1967. 5. Crank, J.: The Mathematics of Diffusion, Ed. 1, Oxford, 1956, Clarendon Press, pp. 59, 93. 6. Rober, H., Goring, W., Sous, H., and Reim, M.: Concentration of ampicillin in the vitreous after cryocoagulation, Albrech v. Graefes Arch. Klin. Exp. Ophthalmol. 204:275, 1977. 7. Wallow, I. H. L., Tso, M. O. M., and Fine, B. S.: Retinal repair after experimental xenon arc photocoagulation: I. A comparison between rhesus monkey and rabbit, Am. J. Ophthalmol. 75:32, 1973. Cortical responses evoked by laser speckle. WILLIAM W. DAWSON AND MICHAEL C. BARRIS. Human cortical evoked responses elicited by patterns are very size and focus dependent, but those produced by moving laser speckle patterns (LASCERs) remain similar in amplitude and subjective sharpness over a wide (±20 D) variation in added lens power. Moreover, cortical signal amplitudes evoked by speckle displays with high average spatial frequencies are significantly larger than those reported for check stimuli equivalent in spatial frequency. Consistent with animal data on cortical unit responses,1 patterned stimulation of the human retina produces cortical evoked signals consistent in amplitude across normal subjects. Human visual cortical evoked responses produced by patterned stimuli (pattern VERs) are highly dependent upon retinal image quality.2 Furthermore, these pattern VERs are not linearly related to the pattern element visual angular subtense.3 Speckle patterns produced by laser irradiation may be shifted spatially over time to produce visual stimulation. We have found that the amplitudes of laser speckle cortical evoked responses (LASCERs) are largely independent of the refractive condition of the eye and evoke signals which are several times larger in magnitude than those reported for patterns equivalent in mean spatial frequency. These attributes suggest that LASCERs may be developed to evaluate visual resolution in patients where there are opacities. Indeed, Arden and Sheorey4 reported that their opacity patients continued to see speckle when low-frequency gratings produced by a laser interferometer could no longer be seen. The physical understanding of laser speckle has developed largely since I960.5 Speckle is produced readily whenever coherent energy is reflected from a roughened surface. The speckle pattern (Fig. 1) is the consequence of constructive and destructive interference of coherent wavefronts whose phase relations have been altered by reflection from a surface. The granular pattern may be detected in any plane where a sensor (e.g., photographic emulsion, retina, photodiode) is present. An aperture in front of the sensor enhances the speckle by increasing the number of interference fringes.6 The spatial frequency and irradiance of the speckle is a complex interaction between the detector-reflector distance, aperture size, and reflector surface characteristics.7 Lenses between the detector and the reflecting surface produce small changes in the apparent size of the speckle but do not alter the sharpness of speckle borders. The spatial frequency of speckle is approximated by a Gaussian probability distribution.8 Methods. Human subjects viewed laser speckle 0146-0404/78/121209+04$00.40/0 © 1978 Assoc. for Res. in Vis. and Ophthal., Inc. Downloaded From: http://iovs.arvojournals.org/ on 05/05/2017 1209