Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Schizoaffective disorder wikipedia , lookup
Antisocial personality disorder wikipedia , lookup
Critical Psychiatry Network wikipedia , lookup
Selective mutism wikipedia , lookup
Panic disorder wikipedia , lookup
Asperger syndrome wikipedia , lookup
Classification of mental disorders wikipedia , lookup
Antipsychotic wikipedia , lookup
Autism therapies wikipedia , lookup
History of psychiatric institutions wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Abnormal psychology wikipedia , lookup
Narcissistic personality disorder wikipedia , lookup
Conduct disorder wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
Pyotr Gannushkin wikipedia , lookup
Separation anxiety disorder wikipedia , lookup
Conversion disorder wikipedia , lookup
Factitious disorder imposed on another wikipedia , lookup
History of mental disorders wikipedia , lookup
Moral treatment wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Emergency psychiatry wikipedia , lookup
History of psychiatry wikipedia , lookup
Sluggish cognitive tempo wikipedia , lookup
Child psychopathology wikipedia , lookup
Attention deficit hyperactivity disorder wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Attention deficit hyperactivity disorder controversies wikipedia , lookup
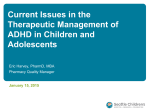
Advances in the Treatment of Attention-Deficit/Hyperactivity Disorder: A Guide for Pediatric Neurologists Sharon B. Wigal, PhD, Stephanie Chae, Avni Patel, and Robin Steinberg-Epstein, MD The purpose of this article is to assist pediatric neurologists in practice and in training to better understand and distinguish between several of the most commonly prescribed treatments for attention-deficit/hyperactivity disorder (ADHD) in school-aged children. Among the various pharmacotherapies available for ADHD, 4 specific medications will be reviewed: oral release osmotic system methylphenidate hydrochloride (CON; Concerta, McNeil Pharmaceuticals), lisdexamfetamine dimesylate (LDX; Vyvanse, Shire Pharmaceuticals), atomoxetine (ATX; Strattera, Eli Lilly), and guanfacine extended-release (GXR; Intuniv, Shire Pharmaceuticals). This article contains information including medication-release pattern, administration including available dosing, adverse reactions, and case studies to serve as a guide to help determine when a particular treatment might be more appropriate than another. Although ADHD is apparent across the lifespan, this article will focus on children with ADHD from ages 6 to 12 years old. Importantly, although a number of stimulant and nonstimulant treatment options are available for school-aged children diagnosed with ADHD, choosing the best treatment options is highly dependent on obtaining thorough family and medical histories. Semin Pediatr Neurol 17:230-236 © 2010 Elsevier Inc. All rights reserved. A ttention-deficit/hyperactivity disorder (ADHD) is the most common child psychiatric disorder of hyperactivity, impulsivity and/or inattention. It is a chronic condition that affects people of all ages from young children through adulthood. Symptoms of ADHD are noticeable and diagnosed at various stages of life although more commonly in children before age 7 years. In children with ADHD, symptoms may be apparent socially, emotionally, and academically. ADHD may lead to low self-esteem, poor peer relationships, delinquencies, and substance abuse. Approximately From the Department of Pediatrics, Child Development Center, University of California, Irvine, CA. Dr Sharon B. Wigal is a consultant for Abbott, McNeil, NuTec, Shire, Taisho, and the NIMH; has received grant/research support from Addrenex, Eli Lilly, McNeil, Next Wave Pharmaceuticals, Otsuka, Psychogenics, Quintiles, Shionogi Pharm, Shionogi Pharm, Shire, and the NIMH; and is on the speaker or advisory boards for McNeil, the NIMH, Shire, and UCB. Dr Robin Steinberg-Epstein is a consultant for McNeil and Shire; has received grant/research support from Addrenex, Eli Lilly, McNeil, Next Wave Pharmaceuticals, Otsuka, Psychogenics, Quintiles, Shionogi Pharm, Shire, and the NIMH; and is on the speaker or advisory boards for Eli Lilly, McNeil, and Shire. Address reprint requests to Sharon B. Wigal, PhD, Department of Pediatrics, Child Development Center, University of California, Irvine, CA 92612. E-mail: [email protected] 230 1071-9091/10/$-see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.spen.2010.10.005 65% of children identified with ADHD since childhood will continue to exhibit symptoms as adults.1 To diagnose ADHD, the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) is used.1 Approximately 3% to 7% of children from ages 8 to 15 years old meet criteria for ADHD. The diagnosis of ADHD can be divided into 3 categories: predominantly inattentive, predominantly hyperactive-impulsive, and combined type, which is both inattentive and hyperactive. The DSM-IV-TR lists 9 different symptoms for both categories of inattentiveness and hyperactivity-impulsivity (Table 1). To be diagnosed with one of the categories of ADHD, a child must present with 6 of the 9 symptoms of impairment in at least 2 different settings, such as classroom and home. These symptoms must be present for at least 6 months and must not be explained by other psychiatric diagnoses. Based on current research, including the Multimodality Treatment Study of Children with ADHD (MTA), there is overwhelming consensus that the primary treatment of ADHD is medication and that accessory symptoms are benefited by multimodal treatment (a combination of medication and alternative treatments).2 This is further supported by the guidelines set forth by 3 major academies (the American Academy of Neurology, the American Academy of Child & Adolescent Psychiatry, and the American Academy of Pedi- ADHD treatment update Table 1 DSM-IV-TR Criteria of Symptomatology in AttentionDeficit Disorder Inattention: must include at least 6 of the following symptoms of inattention that must have persisted for at least 6 months to a degree that is maladaptive and inconsistent with developmental level: Often fails to give close attention to details or makes careless mistakes in schoolwork, work, or other activities Often has difficulty sustaining attention in tasks or play activities Often does not seem to listen to what is being said Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (not due to oppositional behavior or failure to understand instructions) Often has difficulties organizing tasks and activities Often avoids or strongly dislikes tasks (such as schoolwork or homework) that require sustained mental effort Often loses things necessary for tasks or activities (school assignments, pencils, books, tools, or toys) Often is easily distracted by extraneous stimuli Often forgetful in daily activities Hyperactivity/impulsivity: must include at least 6 of the following symptoms of hyperactivity-impulsivity that must have persisted for at least 6 months to a degree that is maladaptive and inconsistent with developmental level: Hyperactivity evidenced by fidgeting with hands or feet, squirming in seat Hyperactivity evidenced by leaving seat in classroom or in other situations in which remaining seated is expected Hyperactivity evidenced by running about or climbing excessively in situations where this behavior is inappropriate (in adolescents or adults, this may be limited to subjective feelings of restlessness) Hyperactivity evidenced by difficulty playing or engaging in leisure activities quietly Hyperactivity evidenced by often on the go or acting as if driven by a motor Hyperactivity evidenced by talking excessively Impulsivity evidenced by blurting out answers to questions before the questions have been completed Impulsivity evidenced by showing difficulty waiting in lines or awaiting turn in games or group situations Impulsivity evidenced by interrupting or intruding on others Data from DSM-IV-TR. Copyright 2000 American Psychiatric Association. atrics) as well as by international consensus.3 Although some alternative treatments (eg, nutrition and exercise) have been shown to improve psychiatric comorbidities, there is limited evidence to suggest their direct benefit for ADHD.4 Treatment Algorithm The Texas Children’s Medication Algorithm Project5 was designed to be used in community mental health centers, pro- 231 viding suggestions for drug choice as it applies to ADHD treatment. As a guide that serves as the basis for the American Academy of Child & Adolescent Psychiatry practice parameter on the treatment of children and adolescents with ADHD,6 it offers opportunities to determine pharmacotherapy with maximal benefits while taking into consideration the unique attributes of any given case. Overall, this consensus-driven algorithm establishes the use of a stimulant for the first stage of treatment followed by a second stage of stimulant, progressing to nonstimulant use. Although some aspects of this algorithm are no longer relevant, such as the use of pemoline (mostly because of concerns regarding fatal hepatotoxicity), the general rationale still can be used and applied to presently available agents. Stimulants Stimulants have been used to treat symptoms of ADHD for more than 50 years. As mentioned earlier, the Texas Consensus Conference Panel on Pharmacotherapy of Childhood ADHD developed the use of stimulant medications as firstline options for the medical management of children and adolescents with classic ADHD without other complicating features.5,6 The expectation is that 70% of patients will respond to the first stimulant that is tried with the recommendation that a second be tried to yield up to an 80% benefit.7 Case Study 1 This child has been diagnosed with ADHD, inattentive subtype and comorbid oppositional defiant disorder (ODD; see Figure 1 below for Case Study 1). Following the treatment algorithm,5 this would suggest starting with a stimulant medication. One must first consider whether there are contraindications to a stimulant. We know that there is no known cardiac history in this patient to suggest a need for a pretreatment echocardiogram. No laboratory studies are necessary. Given that her weight is greater than the 95th percentile, there is no concern that weight loss will be a problem for her, and, in fact, stimulants may at first be helpful. Although there may be some initial weight loss, we would not expect ongoing weight loss. In general, over two thirds of the Multimodality Treatment Study of Children with ADHD sample exhibited concurrent psychiatric disorders.2 As for ODD, the literature supports the use of stimulants in patients with ODD and ADHD.8 Controlling ADHD with a stimulant may offer benefits for ODD symptoms. There is certainly evidence that in the face of ODD, stimulants still work to improve ADHD symptoms and do not worsen the ODD.3 How does one know which stimulant to choose? Stimulants generally belong to either the methylphenidate family or the amphetamine family. The first consideration is one of duration. Given that this is a 9 year old with homework that is taking an inordinate amount of time to complete and her problems exist throughout the school day, a long-acting medication would be the most appropriate. Table 2 provides S.B. Wigal et al 232 Case Study #1 Identification and Presenting Complaints: A 9-year-old girl was brought into the clinic for diagnosis and treatment of possible ADHD. Her mother was concerned because for the last 3 years teachers had mentioned that her daughter was seated up front due to problems staying on task during schoolwork. Her grades are mostly “C’s” with a sprinkling of “B’s” and “D’s”. She has difficulty finishing books and likes to skip to the end to see what happens. Mom often finds her completed, ungraded homework at the bottom of her backpack. Her mom also mentions that she does not listen when spoken to and is quite a daydreamer. She misplaces or loses things that are not important to her; always forgetting things at school. She can takes hours to complete a simple homework assignment. In addition, her mother reports that the teachers also mentioned that she has a hard time making friends. She also has a lot of trouble getting along with her mom; she picks fights and demands things her way. She gets along with her dad and is a tomboy when it comes to her relationship with her brother. She initiates fights with her brother. Physical Exam: She is moderately obese (weight 47 kg (>95th percentile)) but otherwise has a normal general and neurologic exam. Family History: There is a maternal history of ADHD, including the patient’s mother and grandmother having ADHD diagnoses. The girl’s father does not have any history of behavior or mental health problems. No family history exists for sudden, unexpected death or structural cardiac defects. Supporting Data: ADHD rating scales submitted by both parent and teacher showed significant elevations in inattentive and oppositional symptoms. Diagnosis: ADHD, predominantly inattentive subtype with a comorbid problem of ODD Treatment considerations and diagnostic formulation: - Child’s weight is > 95th percentile - Oppositional Defiant Disorder (ODD) diagnosed. - No other psychiatric condition identified (i.e., anxiety or autism spectrum disorders) Key questions for differential treatment: - Is the child’s weight within the normal range, high or low? - Is ODD or some other comorbid disorder present with ADHD symptoms? - Are there any contraindications to treatment? Figure 1 A case study of a child treated with stimulant pharmacotherapy. key details of a few research studies regarding the development of 2 of these products. For the purpose of our discussion, we have chosen to compare 2 long-acting medications: lisdexamfetamine (LDX; Shire Pharmaceutical, Wayne, PA) and Concerta (CON; McNeil Pharmaceuticals, Fort Washington, PA) (See Table 3 for summary information about these 2 stimulants). Although they have similar duration of action and side effect profiles, there are subtle differences that may lead to a choice of one over the other. For example, studies suggest that the severity of appetite suppression may be more significant for LDX and other amphetamines than for other methylphenidate products with the same average duration of action. Such an “adverse effect” might actually be of benefit for this particular patient. By contrast, if this child could not be taught to swallow a pill, LDX can be combined with a liquid to make a solution. Overall, either of these medications serves as an excellent option for her. However, should she respond with significant sleep-onset problems, one might choose a shorteracting (ie, not a sustained- or extended-release) stimulant medication. Nonstimulants Although stimulant drug treatments have proved to be highly effective and safe in treating symptoms of ADHD, approximately 20% of children with ADHD fail to respond or have significant side effects to one of the first 2 stimulants that are tried. Following the treatment algorithm,5 practitioners are encouraged to consider nonstimulant drugs as second-line treatments, with the exception of individuals with ADHD having an active substance abuse problem, comorbid anxiety, or tics, for which nonstimulants would be the first-line treatment.9 Thus, nonstimulants are used when ADHD patients fail to respond to stimulants or have increased side effects. Furthermore, there are subgroups of children whose comorbid conditions (eg, anxiety, tics) may be exacerbated by stimulant treatment. Thus, alternate pharmacotherapy may yield beneficial effects on accessory symptoms while also treating primary ADHD symptoms. Table 4 summarizes several key studies regarding development of 2 specific nonstimulant medications. ADHD treatment update 233 Table 2 Representative Studies of 2 Stimulant Treatments for ADHD OROS Methylphenidate Hydrochloride Citation 200211 Swanson et al, Swanson et al, 200412 Wolraich et al, 200113 Emphasis Conclusion Laboratory school study comparing objective activity levels during structured classroom activities and outside recess activities Comparative trial of 2 long-acting MPH products in the laboratory school setting Randomized study comparing placebo, immediate release MPH tid and CON CON treatment improved attention and behavior during classroom seatwork but generally showed no difference from placebo in the playground The specific time-course profiles are demonstrated, which show differences in onset and duration Demonstrated significance of both MPH treatments over placebo with equivalent efficacy to each other Lisdexamfetamine Citation Emphasis Biederman, et al, 200714 Pennick, 2010 Conclusion Laboratory school study of LDX demonstrating its long acting effects 15 Absorption and metabolic conversion of LDX to d-amphetamine Wigal, et al, 200916 Laboratory school study evaluating the onset and offset effects of LDX Significant improvements were noted from the first time point measured until 12 h. However, no predose baseline was measured Blood vs liver tissue as responsible for the conversion of the inactive prodrug to active amphetamine treatment Placebo controlled study of LDX with efficacy extended in both directions from Biederman et al, 200714 OROS, Oral release osmotic system; CON, Concerta (OROS methylphenidate hydrochloride); MPH, Methylphenidate; tid, 3 times per day. Table 3 Summary Information for 2 Commonly Prescribed Stimulants to Treat ADHD Stimulants Product Delivery System Approval by FDA Doses Initial dose Onset of activity Duration of activity Administration Common side effects OROS Methylphenidate Hydrochloride (Concerta) LDX Dimesylate (Vyvanse) Methylphenidate Oral Release Osmotic System August 2000 18, 27, 36, 54, and 72 mg; (2 ⴛ 36 mg) 18 mg 1h Up to 12 h postdose, extended Once daily in the morning with or without food; Swallow whole; do not crush or chew Decreased appetite, dry mouth, trouble sleeping, dizziness, stomach ache, increased sweating, headache, nausea, anxiety, weight loss, irritability d-amphetamine prodrug February 2007 Twenty, 30, 40, 50, 60, and 70 mg 30 mg 1.5 h Up to 13 h postdose, extended Daily in the morning with or without food; May dissolve it in water. Upper abdominal pain, decreased appetite, dry mouth, dizziness, irritability, insomnia, weight loss Table 4 Representative Studies of 2 Nonstimulant Treatments for ADHD Atomoxetine Citation Faraone et al, Study Description 200717 Statistical extension of Wigal, et al, laboratory school study (see below) Wigal et al, 200518 Laboratory school study measuring time course effects of ATX and MAS-XR Michelson et al, 200219 Clinic study of ATX with quality of life measurements Comparison of two different methods for initiating ATX to reduce incidence of adverse events Greenhill et al, 200720 Conclusion Forecasting to 8-wk treatment period showed continued greater efficacy for mixed amphetamine salts, extended-release MAS-XR compared with ATX Short-term study replicating significant ATX within 1-wk of initial dosing and time course effects in comparison with amphetamine treatment Demonstrated treatment effects within 1 wk of usage Lower risk of adverse events if over the first few weeks of treatment, patients receive doses divided into 2 per day and titrated to full dose (1.2 mg/kg/d) more slowly Guanfacine Extended Release Citation Biederman et al, Study Description 200821 Connor & Rubin, 201022 Spencer et al, 200923 Forced dose escalation study of GXR vs placebo for 8 wks Review paper on GXR Coadministration of GXR and stimulant medication Conclusion Improvements with GXR similar to other nonstimulants Mild slowing of heart rate and some lowering of systolic blood pressure and diastolic blood pressure occurs and requires vital sign monitoring during treatment Increased ADHD symptom improvement with no new adverse events S.B. Wigal et al 234 Case Study #2 Identification and Presenting Complaints: This 10 ½-year-old boy presents with concerns regarding inconsistent grades and several behavioral complaints. His mother reports that he will get “A’s” on tests but will not turn in projects and will end up with “C’s” as final grades. At a parent-teacher conference, his teacher mentioned that he disrupts other students when they are speaking, blurts out answers, and is very talkative. He has trouble listening and following directions, and often daydreams in class. He feels as if his teacher “hates” him and favors other students in the class. He says he does not understand why others don’t see things the way he does including his older brother, with whom he is continually arguing. The only thing he will sit still for is video games. His mother also notices that his backpack and his room are extremely messy and disorganized. Mom is also concerned because he is still so afraid of the dark that he sleeps with the light on. He will not spend the night at a friend's house and is extremely afraid of dogs, even the neighbor's puppy. th Physical Exam: The patient weighs 26.4 kg (just below 5 percentile) and otherwise has normal general and neurologic exams, with the exception of blood pressure being 130/85. Family History: There is no maternal or paternal history of mental health disorders; however the father had an alcohol problem prior to marriage. In addition, the patient’s older brother is diagnosed and in treatment for a chronic tic disorder. No family history exists for sudden, unexpected death or structural cardiac defects. Diagnosis: ADHD, combined subtype Treatment considerations: - Sibling with chronic tic disorder - Blood pressure - Co-morbid symptoms of anxiety Key questions for differential treatment: - Is there a family history of tics or Tourette’s Disorder? - Is the child’s blood pressure within normal limits, high or low? Figure 2 A case study of a child treated with nonstimulant pharmacotherapy. Case Study 2 This child was diagnosed with ADHD, combined subtype (see Figure 2). However, there are some distinct concerns that may alter the choice of medication. Although it would not be incorrect to choose a stimulant as the treatment of choice, one must consider how this child presents (eg, high blood pressure, a family history of a tic disorder, low weight, and a potential comorbid anxiety issue). Each of these issues are explored more closely later. Although studies of stimulant medication typically show a statistically significant increase in blood pressure, they do not show a clinically relevant increase. However, one of the medication options, guanfacine extended-release (GXR) (a recently available extended-release form of guanfacine), is a known antihypertensive agent and thus can cause decreases in blood pressure. Therefore, one might opt to consider this nonstimulant as a strong possibility because, in this case, such blood pressure effects are an advantage. It is important to become familiar with the side effect profile of each medication because they can sometimes be used to the patient’s advantage (Table 5). In addition, instructions to families should be clear about discontinuation practices. For instance, GXR should be tapered off with decreases in incre- ments of 1 mg every 3 to 7 days as directed on the product label. This would even be important for a child with hypertension because it would be very important for this child’s family to be aware of potential rebound hypertension if the medication were to be suddenly withdrawn. Of course, any child with elevated blood pressure also requires further medical investigation to determine the etiology. In a child with known hypertension being managed by a cardiologist, nephrologist, or pediatrician, that physician should be consulted regarding possible medication choices. As for the history of a tic disorder, there is evidence that stimulant treatment, at least temporarily, may increase tics in some individuals.10 Longer-term studies show, however, that there is no overall increase in tics in most individuals.10 As for ATX, there is no evidence of an effect on tics in either direction. GXR, in contrast, may decrease tics because guanfacine has commonly been prescribed as a primary treatment for motor tics in the non– extended-release form. Stimulants and ATX may lead to decreased appetite and weight loss, but GXR does not appear to have an effect in that regard. Finally, anxiety seems to be a presenting problem for this child. The stimulants may worsen anxiety. GXR generally has no effect on anxiety, whereas ATX has mild anxiolytic ADHD treatment update 235 Table 5 Summary Information for 2 Commonly Prescribed Nonstimulants to Treat ADHD Nonstimulants Product Guanfacine Extended-Release (Intuniv) FDA approval Doses September 2009 1, 2, 3, and 4 mg Initial dose Onset of activity Duration of activity Administration 1 mg Some effects in 1 wk 6-8 h extended Atomoxetine (Strattera) November 2002 10,18,25,40, 60, 80, and 100 mg 0.5 mg/kg Some effects in 1 wk 7-9 h and up to 24 h Once or twice daily Once daily in the by mouth with or morning. Swallow without food whole; do not crush or chew Common Side Sleepiness, dry mouth Abdominal pain, decreased effects drowsiness, appetite, nausea dizziness low blood or vomiting, pressure, irritability, dizziness, mood headache, swings, constipation, nausea, somnolence not hungry (decreased appetite), stomach pain benefits. Therefore, if one had the sense that anxiety were an overriding issue, ATX might be the medication of choice. Of course, one might alternatively consider medical therapies specifically focused on anxiety, but these options will not be further considered in this review. As mentioned earlier, stimulants produce an overall more robust response, with over 70% of subjects responding to the first stimulant tried and up to 80% to the second one. The response to the nonstimulant medications (both GXR and ATX) is closer to 50%. Prolonged sedation may be seen with GXR in the first several weeks of use and with ATX in the first few days of use. For this patient, it seems likely that starting either GXR or ATX may provide some unique benefits or protections. See Table 5 for summary information for each of these 2 nonstimulant medications. Conclusions Each of the reviewed stimulant and nonstimulant medications has its own set of benefits and drawbacks. Thus, it is imperative for individual practitioners to gain familiarity with the nuances of treatment options. By reviewing research findings and medication properties of each, following the suggested practical algorithm, and carefully choosing the best option for a particular patient profile, neurologists can gain clinical experience in the optimal treatment of ADHD in children while helping them reach their true potential. References 1. American Psychiatric Association, DSM: IV TR: Diagnostic and Statistical Manual of Mental Disorders (ed 4). Washington, DC, American Psychiatric Publishing, Inc, 2000, pp 78-85 2. MTA Cooperative Group: A 14-month Randomized Clinical Trial of Treatment strategies for attention deficit hyperactivity disorder. Arch Gen Psychiatry 56:1073-1086, 1999 3. Kutcher S, Aman M, Brooks SJ, et al: International consensus statement on attention-deficit/hyperactivity disorder (ADHD) and disruptive behavior disorders (DBDs): clinical implications and treatment practice suggestions. Eur Neuropsychopharmacol 14:11-28, 2004 4. Larzelere MM, Campbell JS, Robertson M: Complementary and alternative medicine usage for behavioral health indications. Prim Care 37:213-236, 2010 5. Pliszka SR, Crismon ML, Hughes CW, et al: Texas Consensus Conference Panel on pharmacotherapy of childhood attention deficit hyperactivity disorder. Revision of the algorithm for pharmacotherapy of attentiondeficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 45:642657, 2006 6. Pliszka S: Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 7:894-921, 2007 7. Elia J, Ambrosini PJ, Rapoport JL: Treatment of attention-deficit-hyperactivity disorder. N Engl J Med 340:780-788, 1999 8. Connor DF, Doerflor LA: Attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder or conduct disorder. Curr Attention Dis Rep 1:5-11, 2009 9. American Academy of Child and Adolescent Psychiatry (AACAP): Official action: Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 46:894-921, 2007 10. Poncin Y, Sukhodolsky DG, McGuire J, et al: Drug and non-drug treatments of children with ADHD and tic disorders. Eur Child Adolesc Psychiatry 7 16:78-88, 2007 (suppl 1) 11. Swanson J, Gupta S, Williams L, et al: Efficacy of a new pattern of delivery of methylphenidate for the treatment of ADHD: Effects on activity level in the classroom and on the playground. J Am Acad Child Adolesc Psychiatry 41:1306-1314, 2002 12. Swanson JM, Wigal SB, Wigal T, et al: A comparison of once-daily extended release methylphenidate formulations in children with attention-deficit/hyperactivity disorder in the laboratory school (The Comacs Study). Pediatrics 113:206-216, 2004 13. Wolraich ML, Greenhill LL, Pelham W, et al: Randomized, controlled trial of OROS methylphenidate once a day in children with attentiondeficit/hyperactivity disorder. Pediatrics 108:883-892, 2000 14. Biederman J, Boellner SW, Childress AC, et al: Lisdexamfetamine dimesylate and mixed amphetamine salts extended-release in children with ADHD: A double-blind, placebo-controlled, crossover analog classroom study. Biol Psychiatry 62:970-976, 2007 15. Pennick M: Absorption of lisdexamfetamine dimesylate and its enzymatic conversion to d-amphetamine. Neuropsychiatr Dis Treat 6:317327, 2010 16. Wigal SB, Kollins SH, Childress AC, et al: A 13-hour laboratory school study of lisdexamfetamine dimesylate in school-aged children with attention-deficit/hyperactivity disorder. Child Adolesc Psychiatry Ment Health 3:17, 2009 17. Faraone SV, Wigal SB, Hodgkins P: Forecasting three-month outcomes in a laboratory school comparison of mixed amphetamine salts extended release (Adderall XR) and atomoxetine (Strattera) in schoolaged children with ADHD. J Atten Disord 11:74-82, 2007 18. Wigal SB, McGough JJ, McCracken JT, et al: A laboratory school comparison of mixed amphetamine salts extended release (Adderall XR) and atomoxetine (Strattera) in school-aged children with attention deficit/hyperactivity disorder. J Atten Disord 9:275-289, 2005 19. Michelson D, Allen AJ, Busner J, et al: Once-daily atomoxetine treatment for children and adolescents with attention deficit hyperactivity disorder: A randomized, placebo-controlled study. Am J Psychiatry 159:1896-1901, 2002 236 20. Greenhill LL, Newcorn JH, Gao H, et al: Effect of two different methods of initiating atomoxetine on the adverse event profile of atomoxetine. J Am Acad Child Adolesc Psychiatry 46:566-572, 2007 21. Biederman J, Melmed RD, Patel A, et al: A randomized, double-blind, placebo-controlled study of guanfacine extended release in children and adolescents with attention-deficit/hyperactivity disorder. Pediatrics 121: e73-e84, 2008 S.B. Wigal et al 22. Connor DF, Rubin J: Guanfacine extended release in the treatment of attention deficit hyperactivity disorder in children and adolescents. Drugs Today 46:299-314, 2010 23. Spencer TJ, Greenbaum M, Ginsberg LD, et al: Safety and effectiveness of coadministration of guanfacine extended release and psychostimulants in children and adolescents with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol 19:501-510, 2009