Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
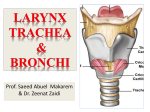
Epiglottis , A Little Cause of Obstructive Sleep Apnea BY AHMAD YOUNES PROFESSOR OF THORACIC MEDICINE Mansoura Faculty of Medicine Obstructive Sleep Apnea • Obstructive Sleep Apnea (OSA) is caused by obstruction or narrowing of the upper airway starting from nose to laryngeal level. Laryngeal Anatomy • The LARYNX is an apparatus made up of cartilage, ligaments, muscles, and mucous membrane, which guards the entrance to the lower respiratory passages (trachea, bronchi, and lungs) and houses the vocal cords. • Note that the hyoid bone is not usually considered as part of the larynx. Three major types of movement are possible: 1. MOVEMENT AFFECTING THE TENSION OF THE VOCAL CORDS. Since the vocal cords are attached to the arytenoid cartilages posteriorly and the thyroid cartilage anteriorly, regulation of vocal cord tension (and therefore pitch of the voice) is accomplished primarily by pivoting the thyroid cartilage forward or backward at the cricothyroid joint . 2. MOVEMENTS WHICH INCREASE OR DECREASE THE SIZE OF THE OPENING BETWEEN THE VOCAL CORDS (ABDUCTION OR ADDUCTION OF THE VOCAL CORDS). This action is best appreciated by imagining the larynx viewed from above. Realize: I. That the vocal cords on each side are covered with a mucous membrane, so that when they are abducted, relatively little air can pass either between them or around them.. The bases of the two arytenoid cartilages are L-shaped. The medial process of each is called the vocal process, and the vocal cords attach to it. The lateral process of each is called the muscular process, and most of the muscles which act to abduct or adduct the vocal cords attach to it. Abduction of the vocal cords may be accomplished either by externally rotating the arytenoid cartilages on a pivot located at the angle of the "L“ or by sliding the 2 arytenoid cartilages apart slightly. Realize that there is only 1 muscle which has an abductor action on the vocal cords, although there are several which act to adduct the cords. 3. MOVEMENTS WHICH CLOSE OFF THE ENTRANCE TO THE LARYNX, AS IN SWALLOWING. • The movements of the epiglottis and arytenoid cartilages which take place during swallowing to block off the entrance to the larynx, to prevent food from entering the larynx. Basically, the epiglottis is pulled down, and the arytenoid cartilages are pulled forward, toward the epiglottis. Realize that two other mechanisms which are independent of laryngeal movements per se also help to keep food from entering the larynx during swallowing. • First, the larynx is raised, along with the pharynx, by the contraction of the longitudinal muscles of the pharynx. • Second, the epiglottis also acts partly as a passive barrier to the movement of food, so that food tends to be funneled to either side of the larynx, into the PIRIFORM RECESSES and from there into the esophagus. Pyriform sinus • On either side of the laryngeal orifice is a recess, termed the piriform sinus (also piriform recess, pyriform sinus, piriform fossa, or smuggler's fossa), which is bounded medially by the aryepiglottic fold, laterally by the thyroid cartilage and thyrohyoid membrane. The fossae are involved in speech. • The term "piriform," which means "pear-shaped," is also sometimes spelled "pyriform" . • Deep to the mucous membrane of the piriform fossa lie the recurrent laryngeal nerve as well as the internal laryngeal nerve, a branch of the superior laryngeal nerve. • The internal laryngeal nerve supplies sensation to the area, and it may become damaged if the mucous membrane is inadvertently punctured. • It is a common place for food to become trapped; if foreign material becomes lodged in the piriform fossa of an infant, it may be retrieved nonsurgically. If the area is injured (e.g., by a fish bone), it can give the sensation of food stuck in the throat. • Local anesthesia can be given here because of the presence of internal laryngeal nerve underneath the mucous membrane. OTHER STRUCTURAL FEATURES OF THE LARYNX 1. Above and parallel to the vocal cord on each side is a second ligament called the VESTIBULAR or VENTRICULAR LIGAMENT. This ligament is not actively moved during vocalization, and is therefore referred to as a "false vocal cord." Nonetheless, this ligament (or the fold of mucous membrane which covers it) is a prominent feature when the larynx is examined with a laryngoscope. 2. The entire larynx is covered with a mucous membrane, which is given different names in its different parts, depending on the structures it covers over or runs between . 3. The membrane running between the epiglottis and the arytenoid cartilages, called the QUADRANGULAR MEMBRANE, is reinforced by a small cartilage which is embedded in it, the CUNEIFORM CARTILAGE. 4. On each side, another small cartilage, called the CORNICULATE CARTHAGE, caps the arytenoid cartilage superiorly. PARTS OF THE LARYNGEAL CAVITY The boundaries formed by the vestibular and vocal folds divide the cavity of the larynx into three parts. 1. The VESTIBULE, which is the area above the vestibular folds. 2. The VENTRICLE, which is a pocketlike recess between the vestibular and vocal folds on both sides. 3. The INFRAGLOTTIC CAVITY, which is the area below the vocal folds. There are two other terms you must know: 1. The GLOTTIS is the aperture formed by the vocal folds (analogous to the iris of the eye). 2. The RIMA GLOTTIDIS is the opening between the vocal folds (analogous to the pupil of the eye). Realize that the size of the rima glottidis is a major factor in determining how much air can enter the trachea and lungs. MUSCLES OF THE LARYNX 1 . MUSCLES WHICH AFFECT THE TENSION OF THE VOCAL CORDS. The CRICOTHYROID MUSCLES : The muscles primarily responsible for regulating the tension of the vocal cords. The small VOCALES muscles, which lie parallel and inferior to the vocal cords (control fine adjustment of vocal cord tension. 2. MUSCLES WHICH OPEN AND CLOSE THE RIMA GLOTTIDIS (ABDUCT AND ADDUCT THE VOCAL CORDS). • Abductor: The posterior cricoarytenoid is the only abductor of the vocal cords. • Adductors: The major abductors of the vocal cords are the LATERAL CRICOARYTENOID, THYROARYTENOID, and ARYTENOIDEUS MUSCLES. NERVE SUPPLY TO THE LARYNX AND PHARYNX 1. MOTOR INNERVATION OF THE MUSCLES OF THE PHARYNX AND LARYNX arises mainly from the CRANIAL DIVISION of the ACCESSORY NERVE (XI). Note, however, that these axons TRAVEL with those of the VAGUS NERVE, and are indistinguishable from it. Exception: The STYLOPHARYNGEUS MUSCLE receives its motor innervation from the GLOSSOPHARYNGEAL NERVE (1X) . Note that this is the ONLY muscle innervated by this nerve. Most of the muscles of the larynx receive their innervation via the RECURRENT LARYNGEAL BRANCH of the vagus nerve . • Exception: The CRICOTHYROID MUSCLE, which receives its innervation via the EXTERNAL LARYNGEAL NERVE. 2. SENSORY INNERVATION OF THE LARYNX AND PHARYNX. • Pharynx: via the GLOSSOPHARYNGEAL NERVE • Larynx: via branches of the VAGUS NERVE • Above the vocal folds the sensory innervation of the larynx is via the INTERNAL LARYNGEAL NERVE. • Below the vocal folds it is by way of branches of the RECURRENT LARYNGEAL NERVE. 3. PARASYMPATHETIC INNERVATION OF THE LARYNX AND PHARYNX is mainly by way of branches of the Epiglottis • About 10% patients with OSA will not improve unless one corrects the epiglottis factor. • Epiglottis prolapse during inspiration is an unusual cause of airway obstruction and a rare cause of OSA. The epiglottis can be seen large and floppy closing like a door over the laryngeal inlet during inspiration. • In laryngomalacia the entire larynx collapses including the epiglottis. These patients cannot tolerate CPAP, their obstruction gets worse and suffocated while wearing CPAP. In fact CPAP therapy is contraindicated in laryngeal OSA. Laryngomalacia • Laryngomalacia, is a congenital abnormality of the laryngeal cartilage. • It is a dynamic lesion resulting in collapse of the supraglottic structures during inspiration, leading to airway obstruction. • It is thought to represent a delay of maturation of the supporting structures of the larynx. • Laryngomalacia is the most common cause of congenital stridor and is the most common congenital lesion of the larynx. Laryngomalacia • The epiglottis is small and curled on itself (omegashaped). Approximation of the posterior edges of the epiglottis contributes to the inspiratory obstruction. • Laryngomalacia may affect the epiglottis, the arytenoid cartilages, or both. When the epiglottis is involved, it is often elongated, and the walls fold in on themselves. The epiglottis in cross section resembles an omega, and the lesion has been referred to as an omega-shaped epiglottis. • If the arytenoid cartilages are involved, they appear enlarged. Laryngomalacia • In either case, the cartilage is floppy and is noted to prolapse over the larynx during inspiration. • This inspiratory obstruction causes an inspiratory noise, which may be high-pitched sounds frequently heard in other causes of stridor, coarse sounds resembling nasal congestion, and low-pitched stertorous noises. • More severe compromise may be associated with a lower ratio of the aryepiglottic fold length to the glottic length. • In type 1 laryngomalacia, the aryepiglottic folds are tightened or foreshortened. Type 2 is marked by redundant soft tissue in any area of the supraglottic region. Type 3 is associated with other disorders, such as neuromuscular disease and gastroesophageal reflux. Types of Laryngomalacia • Type 1 – Anterior prolapse of mucosa overlying arytenoid cartilages (57%) • Type 2 – Short aryepiglottic folds tethering of supraglottic structures in close antero-posterior approximation (15%) • Type 3 - Posterior collapse of epiglottis over glottis (13%) • Combination of above types (15%) Types of Laryngomalacia 1-Infantile Laryngomalacia: • Symptoms occur early in life. • Improve by the age of 2 years 2-Late onset Laryngomalacia: • Children > 2 years. • Present during feeding, exercise or sleep. • Presented by snoring or OSA. 3-State Dependent Laryngomalacia: • Older age group / Adults. • Occurs only during sleep. • Diagnosed by sleep endoscopy. Anatomical Abnormalities 1. Omega shaped epiglottis. 2. Short Ary-Epiglottic fold: Ary-Epiglottic /Glottic length • 0.5 = N • 0.3 = severe LM 3. Redundant mucosa over arytenoids. Pathophysiology of Laryngomalacia • • • • • • • • • Neuromuscular hypotonia (Thompson and Turner, 1900) Poor muscular tone causing laryngeal collapse Association with neurologic disorders Dysfunction in sensorimotor integration of afferent reflexes, brainstem function and motor responses Altered sensorimotor integrative function (Thompson, 2010) Intrinsic muscles of larynx not triggered to stent larynx open Seen by lack of laryngeal adductor reflex May be central/brainstem Possibly related to damage from reflux Associated Pathology • Isolated finding in otherwise healthy infant. • Association with neurologic disorders E.g. cerebral palsy • 15-20% have a synchronous lesion • Mild subglottic stenosis • Tracheomalacia Laryngomalacia • Laryngomalacia is the most common cause of chronic inspiratory noise in infants, no matter which type of noise is heard. • Infants with laryngomalacia have a higher incidence of gastroesophageal reflux, presumably a result of the more negative intrathoracic pressures necessary to overcome the inspiratory obstruction. • Conversely, children with significant reflux may have pathologic changes similar to laryngomalacia, especially enlargement and swelling of the arytenoid cartilages. • Some of the swelling of the arytenoid cartilages and of the epiglottis may be secondary to reflux. Laryngomalacia • Occasional inflammatory changes are observed in the larynx, which is referred to as reflux laryngitis. • When the epiglottis is involved, gravity makes the noise more prominent when the baby is supine. • The exaggerated inspiratory effort increases blood return to the pulmonary vascular bed. This could account for the increased likelihood of pulmonary artery hypertension in infants with hypoxemia. • Rarely, the lesion may cause enough hypoxemia or hypoventilation to interfere with normal growth and development. • In severe cases, when laryngomalacia may be associated with gastroesophageal reflux, feeding problems such as choking or gagging may occur . Laryngomalacia • Although this is a congenital lesion, airway sounds typically begin at age 4-6 weeks. Until that age, inspiratory flow rates may not be high enough to generate the sounds. Symptoms typically peak at age 68 months and remit by age 2 years. • Late-onset laryngomalacia may be a distinct entity, which can present after age 2 years. • Noises are inspiratory and may sound like nasal congestion, with which they are initially confused. • Usually, no feeding intolerance is noted, although occasional choking or coughing with feedings may be noted if the baby has reflux. • Oxygen saturation is usually normal and the noise may be increased if the baby is placed supine. • laryngomalacia may present primarily with snoring and/or sleep-disordered breathing and swallowing dysfunction in a significant proportion of children, the diagnosis must be considered in children, older than 3 months, presenting with these upper airway complaints. • Differential Diagnoses Congenital Stridor ,Croup ,Hypocalcemia, Airway Foreign Body, Gastroesophageal Reflux ,Subglottic Stenosis Surgery ,Respiratory Papillomatosis. • Fluoroscopy of the airway may be performed by a pediatric radiologist .The cartilages may be observed collapsing on inspiration on a lateral view of the airway. • Laryngoscopy :Direct visualization of the airway reveals an omega-shaped epiglottis and Enlarged arytenoid cartilages that prolapse over the larynx during inspiration may also be present. Laryngomalacia • In more than 90% of cases, the only treatment necessary for laryngomalacia is time. The lesion gradually improves, and noises disappear by age 2 years in virtually all infants. • The noise steadily increases over the first 6 months, as inspiratory airflow increases with age. Following this increase, a plateau often occurs with a subsequent gradual disappearance of the noise. • In some cases, the signs and symptoms dissipate, but the pathology may persist into childhood and adulthood. In those cases, symptoms or signs may recur with exercise or sometimes with viral infections. • Children with severe retractions, cyanotic spells, and apneas during sleep may have obstructive sleep apnea associated with laryngomalacia. These children should Laryngomalacia • Children with severe retractions, cyanotic spells, and apneas during sleep may have obstructive sleep apnea associated with laryngomalacia. • These children should be evaluated with a sleep study. Supraglottoplasty may be of benefit in children with severe symptoms of laryngomalacia . Thus, a detailed sleep history should be taken in all infants with symptoms of laryngomalacia. • Recent data suggest infants with laryngomalacia and hypoxemia may more readily develop pulmonary hypertension.[7] Therefore, children with hypoxemia should periodically undergo evaluation for pulmonary hyperte Indications for Surgery • 10-31% of infants need surgery for laryngomalacia • Not following expected course/ responding to medical therapy • Severe laryngomalacia 1-Respiratory compromise 2-Feeding difficulty – reflux/aspiration 3-Weight loss/failure to thrive 4- Obstructive sleep apnea Supraglottoplasty • Procedure tailored to site/mechanism of obstruction • Type 1 :Excise redundant arytenoid tissue • Type 2: Divide shortened aryepiglottic folds • Type 3 : Pexy posteriorly displaced epiglottis to base of tongue Sleep endoscopy • Sleep endoscopy is examining the upper airway using a flexible laryngoscope. • The patient is sedated by giving propofol intravenously. • Awake endoscopy will not give much information in these two areas. • Dynamic MRI can be done first. There are two areas need special attention-one is the tongue base and other the epiglottis. • Tongue base snorers are common and correcting the palatal area and nose will give only partial improvement. • Debulking the tongue base may have to be repeated. Some surgeons perform resection of tongue base. • Before considering radical surgery, the simple RF Coblation of tongue base and lateral borders can be done under local anesthesia or along with multilevel surgery. • The treatment of epiglottic collapse is Partial Epiglottidectomy using Co2 laser but one might have to be prepared for a temporary Percutaneous tracheotomy and get consent before surgery. • Injecting sclerosants in the epiglottis will not work. EPIGLOTTIS SURGERY • The epiglottis can contribute to obstructive sleep apnea in some patients, with improvement after partial removal of the epiglottis (epiglottidectomy). • This procedure is performed in the operating room under general anesthesia and is performed entirely by working through the open mouth, without any skin incisions. • A laser or other method of cutting is used to remove a portion of the epiglottis and control any bleeding. RISKS • Bleeding :As with any procedure, there is a risk of bleeding. Bleeding in this area can be serious if it is substantial, as it would be close to the opening into the windpipe (trachea). • Typically, however, there is only minor oozing from the cut edge of the epiglottis that resolves completely within the first 24 hours after surgery. • A major factor in preventing serious bleeding is to avoid the use of aspirin, NSAIDs (such as ibuprofen, Advil®, Motrin®, naproxen, or Aleve®), vitamin supplements, or herbal medications for at least two weeks before and after surgery. • Infection :Infection is uncommon, but patients typically receive antibiotics at the time of surgery to reduce the chance of infection. RISKS • Tooth injury :Operating in the back of the throat is impossible unless an instrument is placed to keep the mouth open. This is the same instrument used when tonsillectomies are done. Rarely, a tooth may be injured by this instrument, and the risk is much higher if a tooth is loose or decayed prior to surgery. • Difficulty swallowing :The epiglottis is important in swallowing because it closes off the opening into the lungs through the trachea . After epiglottis surgery, it is possible to have foods, especially liquids, entering the trachea, only to be cleared with a gentle cough. It is unusual for this complication to be permanent and significant. RISKS • Changes in speech : Any operation on the throat can cause changes in speech. The epiglottis is next to the larynx (voice box), but no surgery is performed on the larynx itself. Therefore, any changes in voice are usually temporary and are not noticeable. • Continued snoring :Many patients undergoing epiglottis surgery will also have loud snoring. The goal of epiglottis surgery is to eliminate obstructive sleep apnea. Usually snoring will improve dramatically if this goal is accomplished. However, many patients will continue to snore to some extent, even after surgery that resolves obstructive sleep apnea completely. • Need for additional procedures :Epiglottis surgery may not be effective in accomplishing the goals of surgery. Another procedure—either performed on the tongue region or on another area—may be necessary. POSTOPERATIVE INSTRUCTIONS • Hospital stay and discharge :Most patients stay in the hospital 1-2 days. The major concerns while you are in the hospital are making sure you are breathing freely, having no bleeding, controlling your pain with oral medications, and drinking enough fluids to have no risk of dehydration. • You do need someone to stay with you the first night home after discharge, for safety. Beyond that, it is helpful to have someone available and checking on you to provide assistance when needed, although they do not have to stay with you 24 hours a day, every day. • Planning before surgery (for example, buying milk or nutritional supplements) will decrease the amount of help you need at home after surgery. POSTOPERATIVE INSTRUCTIONS • Pain control :Like most surgeries, there is pain in the recovery period. Controlling your pain is important for breathing, healing, and being able to swallow enough to maintain your nutrition. • While in the hospital, we will control your pain with oral medications, starting on the day of surgery. You can also hold ice chips inside your mouth to decrease swelling and reduce pain. • Although we will use intravenous pain medications if necessary, the goal will be to use oral medications alone because this is what you will use when you go home after surgery. POSTOPERATIVE INSTRUCTIONS • When you are at home, take your pain medication as you need it. You can also continue to hold ice chips inside your mouth to decrease pain and swelling. Try not to let the pain increase until it becomes intolerable before you take the medication. • If you prefer to avoid narcotics, you should feel free to use acetaminophen (Tylenol®). Avoid aspirin, NSAIDs (such as ibuprofen, Advil®, Motrin®, naproxen, or Aleve®), vitamin supplements, or herbal medications for at least two weeks because they can increase your risk of bleeding after surgery. • Your pain will be significant for at least the first 7-10 days following surgery, but it should improve markedly by 14 days following surgery. POSTOPERATIVE INSTRUCTIONS • Nutrition and fluids : It is very important to have good nutrition and avoid dehydration after surgery. • Due to the pain and swelling that is expected after surgery, you will most likely only be able to tolerate a liquid diet for the first 4-5 days after surgery. Push yourself to drink fluids, even if it is painful. • The first sign of dehydration is a decrease in urination, so keep track of this. In addition to water, it is It is helpful to drink other liquids, such as juices . • It is also essential that your body receive protein and fat in your diet to help with healing and maintaining your energy level. Every day, you should have 3 glasses of something with fat and protein like milk or chocolate milk, POSTOPERATIVE INSTRUCTIONS • As your recovery continues, you will transition to soft solid foods such as eggs, yogurt, or mashed potatoes. • You should be able to tolerate a fairly normal diet by 2 weeks after surgery. • During the recovery period, you should avoid foods with sharp edges such as chips because these can cause bleeding. • Antibiotics :Most patients receive an antibiotic while in the hospital. You may be prescribed an antibiotic to take when you go home. This can be useful for preventing infection and decreasing swelling. POSTOPERATIVE INSTRUCTIONS • Do not use mouthwashes, lozenges, or throat sprays :Patients should not use mouthwashes, lozenges, or throat sprays following surgery because many of these contain alcohol that can irritate the lining of the mouth or numbing medication that can expose you to a serious complication when used for more than a couple of times. • Activity :Walking after surgery is important. Patients should walk at least 3 times a day starting the day after surgery. Walking helps prevent blood clots from forming in your legs. Spending more time out of bed (walking or in a chair) than in bed is helpful because your lungs fill up with air, lowering the risk of fevers and pneumonia. • Patients should avoid strenuous activity for 4 weeks following surgery because that typically raises heart rate and blood pressure. For this reason, it can increase swelling or cause bleeding to start. POSTOPERATIVE INSTRUCTIONS • Ear problems or jaw discomfort :The swelling in your throat that occurs after surgery can cause jaw pain or ear symptoms such as pain, pressure, or fullness. This is common and should improve within 1-2 weeks following surgery. • It occurs because the soft palate and tonsils are next to the jaw and the small Eustachian tube that connects the space behind the eardrum to the top of the throat. Swelling in the throat can interfere with your ability to clear or pop your ears, and it can also be sensed by your body as pain coming from your ears even though the ears are not affected (a phenomenon called referred pain). POSTOPERATIVE INSTRUCTIONS • Sleep with head elevated (at 45 degrees) and avoiding supine position for at least three days :Elevating your head during sleep decreases blood flow to the head and neck regions. Therefore, it decreases swelling and the associated pain. Elevating the head during sleep may also improve breathing patterns by better movement of diaphrgm . POSTOPERATIVE INSTRUCTIONS • Nausea and constipation :Nausea and constipation are very common after any surgery. The anesthetic medications that you receive during surgery and the narcotic pain medication you receive after surgery can cause these. • You will receive medications after surgery to decrease nausea and constipation, but please notify your doctor . if you feel constipated or have not had a bowel movement in any 3 days after surgery. • Postoperative appointment :Yout doctor likes to see his patients 1-2 weeks after surgery. POSTOPERATIVE INSTRUCTIONS • There is hardly any chance of aspiration after removal of part of the epiglottis as the patient fears. • The vestibular fold acts as good protective valve during swallowing. • Effective and relatively safe treatment can be achieved by partial resection of the epiglottis with a microlaryngoscopic CO2 laser. • Hyoid Suspension – If collapse occurs at the tongue base, a hyoid suspension may be indicated. The procedure secures the hyoid bone to the thyroid cartilage and helps to stabilize this region of the airway. Hyoid Suspension Other upper airway surgery • Genioglossus Advancement – The procedure tightens the front tongue tendon; thereby, reducing the degree of tongue displacement into the throat. This operation is often performed in tandem with at least one other procedure such as the UPPP or hyoid suspension. • Maxillomandibular Advancement is a procedure that surgically moves the upper and lower jaws forward. As the bones are surgically advanced, the soft tissues of the tongue and palate are also moved forward, again opening the upper airway. • For some individuals, the MMA is the only technique that can create the necessary air passageway to resolve their OSA condition. Genioglossus Advancement Maxillomandibular Advancement AIRvance System for Obstructive Sleep Apnea • The AIRvance Bone Screw System enables surgical treatment of tongue- and hyoidbased obstructive sleep apnea. • For treating obstructive sleep apnea, there are two surgical procedures that may be performed with the AIRvance System . The tongue suspension procedure can be done with or without the adjunct hyoid suspension procedure. Advantages of the AIRvance procedures • • • • Quick (about 30 minutes for each procedure) Low technical complexity Effective Reversible AIRvance Tongue Suspension • The AIRvance Tongue Suspension Procedure is indicated for the treatment of obstructive sleep apnea and/or snoring. • The tongue suspension procedure can be performed with or without the adjunct hyoid suspension procedure. • The objective of this procedure is to advance and stabilize the genioglossus muscle to help prevent it from falling back and occluding the airway when the patient is supine and asleep. A small titanium screw with attached sutures is implanted in the lower mandible, then the sutures are looped through the tongue to form a hammock that suspends it. AIRvance Hyoid Suspension • The AIRvance Hyoid Suspension procedure is indicated for the treatment of OSA and/or snoring. • It serves as an adjunct to the AIRvance Tongue Suspension procedure. • The goal of this procedure is to help improve airway patency by providing anterior/posterior and lateral support of the lower airway, as well as lateral support of the base of the tongue. This is accomplished by advancing and suspending the hyoid bone and associated musculature. AIRvance Hyoid Suspension • Two small titanium screws with attached sutures are implanted in the lower mandible, and the sutures are looped around the hyoid bone to suspend it.