Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
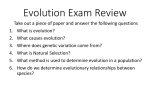
Downloaded from http://jnnp.bmj.com/ on May 5, 2017 - Published by group.bmj.com EDITORIAL 686 Parkinson’s disease ................................................................................... ”Nature versus nurture” and incompletely penetrant mutations DK Simon, MT Lin, A Pascual-Leone ................................................................................... Lessons from twin studies of Parkinson’s disease T he debate over the relative roles of “nature versus nurture” remains unresolved in many fields of study, from childhood education to animal behaviour or neurodegenerative disorders. Points of view frequently are polarised, either nature or nurture, rather then exploring the ways in which both sides play critical and complementary roles. Proponents of “nature” argue that human attributes are uniquely and primarily conditioned by genetics, opposing the view of those who think that environmental influences and experience determine individual differences. Arguments similar to those brought to bear regarding acquisition of skills, language, or cognitive styles also apply to human pathology. Often, in the discussion of disease the terms used are “genetic” versus “environmental”, but the implication is the same as in the “nature” versus “nurture” debate. Disorders considered to be primarily genetic are ones in which the presence or absence of genetic mutations is the primary determinant of disease, independent of environmental circumstances. A disease considered to be primarily environmental is one in which people of virtually any genetic background can develop the disease provided that they are exposed to the necessary environmental factor or factors. However, for many disorders, the risk is strongly influenced by both genetic and environmental factors.1 2 For example, a susceptibility gene may strongly influence the risk of developing a disease only in response to a specific environmental exposure. If the environmental exposure occurs infrequently, the gene will be of low penetrance, and it may seem that the environmental exposure is the primary determinant of the disease, even though the gene is required for developing the disease. Therefore, even when environmental agents are suspected to be a major cause of a particular disease, this does not exclude the possibility that genetic factors also play a major part, particularly genetic mutations with low penetrance. Similarly, a critical mix of nature and nurture is likely to determine personal characteristics. Genetic factors may be thought of as laying the foundation on which environmental agents www.jnnp.com exert their influence. If so, then although certain environmental factors alone (regardless of genetic factors) and certain genetic factors alone (regardless of environmental influences) may explain some behaviours and disease states, most of the time the interaction of both genetic and environment factors will be required. Deafness due to aminoglycoside toxicity is a particularly clear illustration of this interdependence. Prolonged exposure to aminoglycosides is toxic to cochlear cells. However, a mutation at nucleotide position 1555 in the mitochondrial 12S ribosomal RNA gene is associated with an extremely high susceptibility to aminoglycoside induced deafness, even at exposure levels that would not be toxic to most people.3–5 In most cases, the mutation does not cause deafness without aminoglycoside exposure. The “penetrance” of this mutation is therefore dependent on the frequency with which people are exposed to an aminoglycoside antibiotic. If exposure to aminoglycoside antibiotics were rare, then the mutation would have low penetrance, and the critical role of this mutation in determining susceptibility to non-syndromic deafness might be difficult to recognise. To illustrate these points further, in this discussion, we will focus primarily on the potential role of incompletely penetrant mutations in late onset Parkinson’s disease (PD), although similar arguments apply to many late onset neurodegenerative diseases and normal cognitive abilities. GENETIC AND ENVIRONMENTAL FACTORS IN PD It is currently recognised that most late onset neurodegenerative disorders have both genetic and environmental influences. In the case of PD, the relative roles of genetic and environmental factors remain controversial. A recent epidemiological study of the Icelandic population suggested a significant genetic component to late onset PD.6 By contrast, another study comparing concordance rates in monozygotic (MZ) and dizygotic (DZ) twins failed to show evidence for a genetic component for late onset PD.7 For PD with onset after the age of 50, which accounts for most cases of PD, no significant differences were found in the concordance rates between 71 MZ and 90 DZ twin pairs in which at least one twin had PD, though there was a non-significant trend towards increased concordance rates in the MZ twins. This twin study has been interpreted by some as showing that there is no significant genetic component in late onset PD.8 The data from this important study does argue against a major role for high penetrant mutations such as α-synuclein9 or parkin10 in sporadic late onset PD. However, other potentially major genetic contributions are not excluded. The inability of this type of study to address the potential role of mitochondrial genetic factors has been addressed previously.11 12 Additionally, we show below that even large twin studies such as this are insufficiently powered to detect many incompletely penetrant nuclear genetic mutations, even though such mutations could still greatly increase the risk for PD and play a major epidemiological part. Illustrative hypothetical examples are discussed in detail below. PREDICTIONS BASED ON A PD SUSCEPTIBILITY GENE IN A THEORETICAL POPULATION Consider a theoretical population of persons over the age of 65 with a prevalence of PD of 1%, which corresponds with actual estimates of the prevalence of PD in this age group.13 14 We examine three different theoretical mutations, with various frequencies and penetrances and assume for each mutation that it is the only genetic factor that influences risk of PD. However, similar conclusions apply to a wide range of other theoretical incompletely penetrant mutations. Suppose, firstly, that an autosomal dominant mutation “z” present in 50% of persons is associated with a 2% risk of PD. Such a mutation would result in PD in 2% of the 50% of those who have the mutation, representing 1% of the total population. That is, this mutation accounts for all cases of PD, as the prevalence of PD in this theoretical population is 1%. It is an absolutely necessary “permissive” mutation. The risk of disease without the mutation is zero, and the increase in relative risk conferred by the mutation is infinite. Such a mutation would clearly be of enormous epidemiological significance. However, it is extremely unlikely that such a mutation would be detected by a study comparing MZ and DZ twin concordance rates. The concordance rate is defined as the number of twin pairs in which both twins have PD (+PD,+PD) divided by the sum of all twin pairs in which at least one twin has PD (the number of twin pairs that are (+PD,+PD) plus the number that are (+PD,-PD) plus the number that are (-PD,+PD)). With this Downloaded from http://jnnp.bmj.com/ on May 5, 2017 - Published by group.bmj.com EDITORIAL 687 A Mutation in 50% of population D Power to detect mutation "z" 1 0.01 0.9 0.7 Power Concordance rate 0.8 0.008 0.006 Mutation "z" 0.004 0.6 0.5 0.4 0.3 0.2 0.002 0.1 0 0.008 0.012 0 0.02 0.016 0 10 000 Penetrance 20 000 30 000 Number of twins B Mutation in 5% of population E Power to detect mutation "x" 0.15 1 0.9 0.7 0.1 Power Concordance rate 0.8 Mutation "x" 0.05 0.6 0.5 0.4 0.3 0.2 0.1 0 0 0.05 0.1 0.15 0 0.2 0 1000 Penetrance C Mutation in 1% of population 3000 4000 5000 F Power to detect mutation "a" 0.25 1 Mutation "a" 0.9 0.2 0.8 0.7 0.15 Power Concordance rate 2000 Number of twins 0.1 0.6 0.5 0.4 0.3 0.05 0.2 0.1 0 0 0.1 0.2 0.3 0.4 0.5 0.6 0 0 100 Penetrance 200 300 400 Number of twins Figure 1 (A-C) Graphs of the MZ (open symbols) and DZ (closed symbols) concordance rates as a function of the penetrance of the disease associated allele. Graphs are shown for situations in which at least one copy of the disease associated allele is present in (A) 50%, (B) 5%, or (C) 1% of the population. The prevalence of the disease in this hypothetical population is 1%. Note that the range of possible penetrances is inversely proportional to the fraction of the population carrying a disease associated allele, because the product of the penetrance and the fraction of the population carrying the allele cannot exceed the prevalence of the disease. Arrows indicate the points representing concordance rates associated with the theoretical mutations “z” (A), ”x” (B), and ”a” (C) discussed in the text. (D-F) Graphs showing the number of affected twin pairs in each group (MZ and DZ) required in order to have the indicated power to detect a difference in the MZ and DZ concordance rates associated with the mutations “z”, “x”, and “a”. The sample size required to detect the difference between two proportions was calculated using the standard formula15: N=(p1(1-p1)+p2(1-p2))*(zα+zβ)2/ (p1–p2)2 Sample sizes appropriate for a one tailed (α=0.05) z test are shown. definition, the concordance rates predicted to result from mutation “z” are 1.01% for MZ twins and 0.73% for DZ twins (fig 1 A; details of the calculations are available on request). The number of twins required to detect a difference between these concordance rates is exceedingly high. It would require over 14 000 affected twin pairs in each group to have 80% power to detect a difference (fig 1 D; see figure legend for method of calculating power15). This is far beyond even the most exhaustive twin study, by Tanner et al,7 in which only 71 affected MZ twin pairs and 90 affected DZ twin pairs were identified after reviewing a registry of nearly 20 000 twin pairs. www.jnnp.com Downloaded from http://jnnp.bmj.com/ on May 5, 2017 - Published by group.bmj.com EDITORIAL 688 Consider now a less prevalent but more penetrant mutation “x”, present in 5% of the population and associated with a 10% risk of PD. Such a mutation would account for PD in 10% of the 5% of those who have the mutation, or 0.5% of the population. In this case, this would represent half of the cases of PD. Furthermore, the risk of PD without “x” is 0.526%, so the increase in relative risk conferred by the mutation is 19-fold (10% v 0.526%). Like mutation “z”, mutation “x” would clearly have great epidemiological significance. However, again, it is very unlikely that such a mutation would be detected by a study of MZ and DZ twin concordance rates. If “x” were the only genetic risk for PD, the concordance rates predicted to result from “x” are 2.70% for MZ twins and 1.58% for DZ twins (fig 1 B). Again, the number of twin pairs required to detect a difference between these concordance rates is extremely large. It would require about 2100 affected twin pairs in each group to have an 80% chance of detecting a difference between these concordance rates (fig 1 E). Finally, consider a relatively highly penetrant mutation “a”, present in 1% of the population and associated with a 55% risk of PD. Mutation “a” would account for 55% of cases of PD and confer a 121-fold increase in relative risk. Therefore, like mutations “z” or “x”, mutation “a” would be of great epidemiological significance. Furthermore, because of its higher penetrance, the twin concordance rates predicted from mutation “a” are higher than those of “z” or “x”: 17.96% for MZ twins and 8.52% for DZ twins (fig 1 C). Yet, the difference between these rates still is not reliably detectable with the number of twin pairs available. To achieve 80% power to detect this difference, a study would require about twice as many affected twin pairs compared with the numbers available in the study by Tanner et al (fig 1 F).7 Thus, over a very wide range of gene frequencies and penetrances, it is clear that even extremely large and well designed twin studies such as that by Tanner et al7 are still insufficiently powered to detect incompletely penetrant mutations. The literature contains widely varying estimates of sibling concordance rates, depending on the methodology and populations studied. Estimates range from 2% risk of PD among first degree siblings of patients with PD in a community based study,16 to MZ and DZ twin concordance rates of 16% and 11%.7 The risks of PD among siblings associated with hypothetical mutations “z”, “x”, and “a” span this entire range of estimates. Even at the relatively high concordance rates found by Tanner et al, incompletely penetrant mutations that may play a major part in risk of PD are not reliably detected (fig 1 F). www.jnnp.com Clearly, low penetrant mutations do not act alone. Low penetrance implies that other factors, environmental by hypothesis for mutations “x”, “z”, and ‘”a”, must be present for clinical expression of the mutations as PD. Thus, these mutations cause enhanced susceptibility to environmental agents. Already, many genetic variants have been reported in association with PD.17–19 Although many of these associations have not been replicated, it is likely that susceptibility genes play a significant part in the risk of PD and other late onset neurodegenerative disorders. Two well documented examples of low penetrant genetic variants that seem to influence susceptibility to a late onset neurodegenerative disease are the association of the A0 tau gene allele with progressive supranuclear palsy,20–22 and the apoE4 allele with Alzheimer’s disease.23 Technological advances, such as genetic microarrays, may allow rapid screening of many polymorphisms for associations with complex disorders, allowing for further expansion of our knowledge of susceptibility genes as well as clinical application of this knowledge for determining susceptibility to specific disorders. CONCLUSIONS Studies of rare high penetrant mutations such as the α-synuclein gene hold the prospect of disclosing a great deal about the pathophysiology of late onset idiopathic PD. However, α-synuclein mutations are absent in sporadic late onset PD, and twin studies suggest that high penetrant nuclear genetic mutations are unlikely to play a major part. None the less, it remains possible that susceptibility gene variations play a major part in the pathophysiology of a large proportion of late onset cases. Genetic mutations may induce susceptibility to environmental toxins, and both the presence of specific genetic mutations and exposure to particular environmental agents may be required for the development of late onset PD. Therefore, whereas a focus on the role of environmental factors in PD and other neurodegenerative diseases is of critical importance, this should not be done at the expense of further genetic studies, particularly with respect to low penetrant susceptibility genetic mutations. Studies addressing both genetic and environmental factors, as well as their interactions, will be necessary for a complete understanding of PD. The example of PD serves as a pointed illustration of the complex interactions of nature (genetic factors) and nurture (environmental factors) in human diseases and abilities. Studies to address the relative contribution of each are possible, but complex and expensive. Nevertheless, this line of inquiry addresses a fundamental organising principle of brain function that goes well beyond the pathophysiology of diseases. For example, exposed to certain traumatic experiences, some people develop post-traumatic stress syndrome and can be extremely debilitated by it for the rest of their lives. Other people exposed to the similar experiences seem unfazed. Some people seem to thrive in a competitive and result oriented environment whereas others prosper more in a supportive, relaxed atmosphere. Are these interindividual differences grounded on genetic factors that condition the way the brain is changed by certain experiences and hence develops cognitive attributes and illnesses? Identifying such susceptibility genes may allow us to individualise and guide behaviour to maximise educational goals and minimise environmentally induced diseases. The data presented here illustrate that one should not be dissuaded from the potential importance of incompletely penetrant genetic mutations to a human disease or attribute simply due to the lack of significantly different concordance rates detected in studies of MZ and DZ twins. J Neurol Neurosurg Psychiatry 2002;72:686–689 ..................... Authors’ affiliations D K Simon, Department of Neurology, Beth Israel Deaconess Medical Center, Boston, MA, USA M T Lin, Department of Neurology, Weill Medical College of Cornell University, New York, NY, USA A Pascual-Leone, Department of Neurology, Beth Israel Deaconess Medical Center, Boston, MA, USA DKS and MTL contributed equally to the manuscript Correspondence to: Dr M T Lin, Department of Neurology and Neuroscience, Weill Medical College of Cornell University, New York, NY 10021, USA; [email protected] REFERENCES 1 Cooper B. Nature, nurture and mental disorder: old concepts in the new millennium. Br J Psychiatry 2001;178(suppl 40):S91–101. 2 Hulla JE, Miller MS, Taylor JA, et al. Symposium overview: the role of genetic polymorphism and repair deficiencies in environmental disease. Toxicol Sci 1999;47:135–43. 3 Inoue K, Takai D, Soejima A, et al. Mutant mtDNA at 1555 A to G in 12S rRNA gene and hypersusceptibility of mitochondrial translation to streptomycin can be co-transferred to rho 0 HeLa cells. Biochem Biophys Res Commun 1996;223:496–501. 4 Hutchin T, Haworth I, Higashi K, et al. A molecular basis for human hypersensitivity to aminoglycoside antibiotics. Nucleic Acids Res 1993;21:4174–9. 5 Prezant TR, Agapian JV, Bohlman MC, et al. Mitochondrial ribosomal RNA mutation associated with both antibiotic-induced and non-syndromic deafness. Nat Genet 1993;4:289–94. 6 Sveinbjornsdottir S, Hicks AA, Jonsson T, et al. Familial aggregation of Parkinson’s disease in Iceland. N Engl J Med 2000;343:1765–70. Downloaded from http://jnnp.bmj.com/ on May 5, 2017 - Published by group.bmj.com EDITORIAL COMMENTARIES 7 Tanner CM, Ottman R, Goldman SM, et al. Parkinson disease in twins: an etiologic study. JAMA 1999;281:341–6. 8 Cummings JL. Understanding Parkinson disease [editorial; comment]. JAMA 1999;281:376–8. 9 Polymeropoulos MH, Lavedan C, Leroy E, et al. Mutation in the α-synuclein gene identified in families with Parkinson’s disease. Science 1997;276:2045–7. 10 Kitada T, Asakawa S, Hattori N, et al. Mutations in the parkin gene cause autosomal recessive juvenile parkinsonism. Nature 1998;392:605–8. 11 Simon DK. Parkinson disease in twins. JAMA 1999;282:1328, 1328–9. 12 Parker WD Jr, Swerdlow RH, Parks JK, et al. Parkinson disease in twins. JAMA 1999;282:1328. 13 Mayeux R, Marder K, Cote LJ, et al. The frequency of idiopathic Parkinson’s disease by 689 14 15 16 17 18 age, ethnic group, and sex in northern Manhattan, 1988–93. Am J Epidemiol 1995;142:820–7. de Rijk MC, Breteler MM, Graveland GA, et al. Prevalence of Parkinson’s disease in the elderly: the Rotterdam study. Neurology 1995;45:2143–6. Motulsky H. Intuitive biostatistics. New York: Oxford University Press, 1995:199. Marder K, Tang MX, Mejia H, et al. Risk of Parkinson’s disease among first-degree relatives: a community-based study. Neurology 1996;47:155–60. Bajaj NP, Shaw C, Warner T, et al. The genetics of Parkinson’s disease and parkinsonian syndromes. J Neurol 1998;245:625–33. Checkoway H, Farin FM, Costa-Mallen P, et al. Genetic polymorphisms in Parkinson’s disease. Neurotoxicology 1998;19:635–43. EDITORIAL COMMENTARIES Behavioural disorders ................................................................................... Behavioural disorders, Parkinson’s disease, and subthalamic stimulation R G Brown ................................................................................... Stimulation of the bilateral subthalamic nucleus can have adverse consequences T he paper by Houeto et al1 in this issue (pp 701–707) offers new evidence to suggest that bilateral subthalamic nucleus (STN) stimulation can have adverse and potentially serious consequences for patients and their families, despite the benefits obtained in motor function. The study has important implications for those running surgical programmes in terms of patient selection, preoperative counselling, and postoperative care. The management of the motor symptoms of Parkinson’s disease has been greatly enhanced in recent years by new approaches to functional neurosurgery, both stereotactic lesions to the globus pallidus or subthalamic nucleus and stimulation of the same structures via chronically implanted electrodes. These treatments can achieve remarkable clinical outcomes in some patients and significant improvement in many, particularly in the control of levodopa induced dyskinesia. Although research has also investigated the impact of surgery on cognition,2 the psychiatric and the broader social consequences have been largely ignored. The paper reports data on a series of 24 patients, all of who were judged clinically to have benefited from surgery. As in most surgical programmes, patients with dementia or with significant psychiatric problems were excluded as part of normal preoperative clinical screening. Social adjustment was assessed using a standardised instrument 3–38 weeks after surgery and revealed that, although just over a third showed evidence of good to excellent adjustment, moderate or severe impairment was found in the remainder affecting broad aspects of social and interpersonal functioning. Psychiatric problems were also common postoperatively, particularly anxiety disorders. Five patients became depressed after surgery and one patient committing suicide despite having shown dramatic improvement in motor function. Such results offer some important lessons. One key finding was the high level of prior psychopathology in the sample. Such problems were either not reported by patients during screening (possibly for fear that it would lead to exclusion) or were not given sufficient priority in the clinical decision making process. The postoperative exacerbation of these problems and their impact on social adjustment suggest that great care needs to be taken in identifying prior psychiatric disorder, and not just current problems. Although a psychiatric history need not be a cause of exclusion, it 19 Tan EK, Khajavi M, Thornby JI, et al. Variability and validity of polymorphism association studies in Parkinson’s disease. Neurology 2000;55:533–8. 20 Conrad C, Andreadis A, Trojanowski JQ, et al. Genetic evidence for the involvement of tau in progressive supranuclear palsy. Ann Neurol 1997;41:277–81. 21 Morris HR, Janssen JC, Bandmann O, et al. The tau gene A0 polymorphism in progressive supranuclear palsy and related neurodegenerative diseases. J Neurol Neurosurg Psychiatry 1999;66:665–7. 22 Bennett P, Bonifati V, Bonuccelli U, et al. Direct genetic evidence for involvement of tau in progressive supranuclear palsy. European Study Group on Atypical Parkinsonism Consortium. Neurology 1998;51:982–5. 23 Mayeux R, Stern Y, Ottman R, et al. The apolipoprotein epsilon 4 allele in patients with Alzheimer’s disease. Ann Neurol 1993;34:752–4. should indicate the clear need for enhanced postoperative follow up and care in at risk patients. The paper also offers some important anecdotal reports on the cases of social maladjustment. The deterioration of marital and family relations points to the importance of psychosocial factors in the postoperative period. For example, the sudden breakdown in patterns of dependency and caregiving built up over years can have a marked impact on interpersonal relationships. Similar adverse responses, including suicide, have been reported after other dramatically life enhancing surgical procedures such as sight restoration,3 and have long been recognised in the field of organ transplantation.4 Such responses point to the need for careful counselling of patients with Parkinson’s disease and their families before surgery to help prepare them for the possible impact on their lives, both positive and negative. J Neurol Neurosurg Psychiatry 2002;72:689 ..................... Author’s affiliation R G Brown, Department of Psychology, Institute of Psychiatry, King’s College London, De Crespigny Park, London SE5 8AF, UK; [email protected] REFERENCES 1 Houeto JL, Mesnage V, Mallet L et al Behavioural disorders, Parkinson’s disease and subthalamic stimulation. J Neurol Neurosurg Psychiatry 2002;72:701–707. 2 Trepanier LL, Kumar R, Lozano AM, et al. Neuropsychological outcome of GPi pallidotomy and GPi or STN deep brain stimulation in Parkinson’s disease. Brain Cogn 2000;42:324–47. 3 Lester D. Suicide after restoration of sight. JAMA 1971;216:678–9. 4 Dew MA, Switzer GE, DiMartini AF, et al. Psychosocial assessments and outcomes in organ transplantation. ProgTransplant 2000;10:239–59. www.jnnp.com Downloaded from http://jnnp.bmj.com/ on May 5, 2017 - Published by group.bmj.com EDITORIAL COMMENTARIES 690 Impaired cognition ................................................................................... Hypertension+MRI changes=impaired cognition S Tuhrim, S R Levine ................................................................................... A quantifiable formula? A s both the average age of the population and rates of vascular dementia increase, there has been keen interest in measuring and quantifying determinants of cognitive impairment. Koga et al (this issue pp 737–741)1 quantify brain MRI abnormalities and relate them to loss of a normal mental state in a single rural, independent, elderly community. Cognitive impairment was defined as a mini mental state examination (MMSE) score <24 with a mean study score of 26 points.1 The work exemplifies the expanding body of investigations utilising increasingly complex MRI techniques and data analyses to provide insights into brain function beyond those obtainable by mere visual inspection of images. Emerging new structural imaging techniques such as diffusion tensor imaging, can provide information regarding white matter characteristics associated with disease states and brain response to injury (neuroplasticity) and take us beyond more conventional MRI images. The work of Koga et al not only provides confirmation of the importance of white matter lesions and generalised atrophy as markers of cognitive decline but also provides a potentially useful tool for quantifying these changes. It is important not to lose sight, amid this march of technical development, of their confirmation of an important epidemiological finding: the association of www.jnnp.com systolic blood pressure with decreased cognition. Although this factor did not appear in the multivariate logistic model, most likely because of its colinearity with the MRI measurements of white matter lucencies and decreased brain volume, factors with which it is known to be associated, its link to cognitive decline and decreased cerebral perfusion has long been appreciated.2 Recently, analysis of the national Health and Nutrition Examination Survey (NHANES) in the United States indicated that 27% of the United States population had hypertension but only 23% of these with hypertension were taking medication that controlled their blood pressure. Among those with untreated or uncontrolled hypertension, isolated increased systolic blood pressure was the most common pattern found.3 Indeed isolated mild systolic hypertension is the most prevalent form of uncontrolled hypertension in the United States. The work of Koga et al provides further evidence of the importance of addressing this silent epidemic. We also know from the Cardiovascular Health Study (CHS)4 that focal lesions >3 mm on brain MRI (“silent strokes”) were present in 28% of 3324 participants in this study. The presence of these MRI lesions doubled the risk of subsequent stroke, as did increased diastolic and systolic blood pressure, internal carotid artery wall thickness, and the presence of atrial fibrillation. Silent strokes as seen on MRI were an independent predictor of symptomatic stroke, at a rate of 18.7/1000 person-years, over the 4 years of follow up in older people without a clinical history of stroke. Based on the recent results of the PROGRESS trial,5 we should be considering more aggressive blood pressure management in patients with cerebrovascular disease, even in patients with borderline or normal blood pressures (in high risk patients) as data strongly suggest a causal link between blood pressure, MRI lesions, and silent and symptomatic cerebrovascular disease. We are making progress on solving the equation that has blood pressure, MRI changes, and cognition as the variables. J Neurol Neurosurg Psychiatry 2002;72:690 ..................... Authors’ affiliations S Tuhrim, S R Levine, The Stroke Program, Department of Neurology, The Mount Sinai School of Medicine, New York, USA Correspondence to: Dr S R Levine, Stroke Program, Department of Neurology, Box 1137, The Mount Sinai School of Medicine, One Gustave L Levy Place, New York 10029–6574, USA; [email protected] REFERENCES 1 Koga H, Yuzuriha T, Yao H, et al. Quantitative MRI findings and cognitive impairment among community-dwelling elderly subjects. J Neurol Neurosurg Psychiatry 2002;72:737–741. 2 Meyer JS, Rogers RL, Mortel KF. Prospective analysis of long term control of mild hypertension on cerebral blood flow. Stroke 1985;16:985–90. 3 Hyman DJ, Pavlik VN. Characteristics of patients with uncontrolled hypertension in the United States. N Engl J Med 2001;345:479–86. 4 Bernick C, Kuller L, Dulberg C Jr, et al. Silent MRI infarcts and the risk of future stroke: the cardiovascular health study. Neurology 2001;57:1222–9. 5 PROGRESS Collaborative Group. Randomized trial of a perindopril-based blood pressure-lowering regimen among 6105 individuals with previous stroke or tranient ischaemic attack. Lancet 2001;358:1033–41. Downloaded from http://jnnp.bmj.com/ on May 5, 2017 - Published by group.bmj.com ''Nature versus nurture'' and incompletely penetrant mutations DK Simon, MT Lin and A Pascual-Leone J Neurol Neurosurg Psychiatry 2002 72: 686-689 doi: 10.1136/jnnp.72.6.686 Updated information and services can be found at: http://jnnp.bmj.com/content/72/6/686 These include: References Email alerting service This article cites 20 articles, 9 of which you can access for free at: http://jnnp.bmj.com/content/72/6/686#BIBL Receive free email alerts when new articles cite this article. Sign up in the box at the top right corner of the online article. Notes To request permissions go to: http://group.bmj.com/group/rights-licensing/permissions To order reprints go to: http://journals.bmj.com/cgi/reprintform To subscribe to BMJ go to: http://group.bmj.com/subscribe/