Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
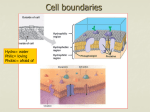
DRUG DISTRIBUTION Distribution Blood Brain Barrier Protein Binding DRUG DISTRIBUTION • Drug distribution is a reversible transport of drug through the body by the systemic circulation • The drug molecules are carried by the blood to: - target site/receptor - non receptor tissues - eliminating organs (liver, kidney) - noneliminating tissues (brain, skin, muscle) - placenta, milk - bound to protein plasma and/or tissue - deposit at bone, fat (slowly released) Circulatory system consists of a series of blood vessels: • Arteries: carry blood to tissues • Veins: return the blood back to the heart Drugs molecules rapidly diffuse through a network of fine capillaries to the tissue spaces filled with interstitial fluid, further may diffuse from interstitial fluid across the cell membrane into the cell cytoplasm The interstitial fluid + plasma water = extracellular water Drug distribution is generally rapid, and most small drug molecules permeate capillary membranes easily The passage of drug molecules across a cell membrane depend on: • The physicochemical nature of both drug ( molecule size, lipid soluble/water soluble) and the cell membrane (composed of protein and bilayer phospholipid) • Blood flow to organ/tissue (high or low vascularization) • Permeability of the membrane and the capillary • pH difference between plasma and tissue Diffusion and Hydrostatic Pressure The processes involved in capillary membrane transverses • Passive diffusion : Fick’s law dQ/dt = - DKA (Cp-Ct) / h • The negative sign means net transfer of drug from inside the capillary lumen into the tissue and extracellular sources • Diffusion is spontaneous and temperature dependent • Hydrostatic pressure = pressure gradient between the arterial end of the capillaries entering the tissue and the venous capillaries leaving the tissue and responsible for penetration of water soluble drugs into spaces between endothelial cells and possibly into lymph • In the kidney high arterial pressure creates a filtration pressure that allows small drug molecules to be filtered in the glomerulus of the renal nephron Distribution of drug entering the cell with blood-flow induced mechanism • Blood-flow induced drug distribution is rapid and efficient, but requires pressure • Blood pressure (BP) decreases when arteries branch into small arterioles – flow speed lows – diffusion into interstitial fluid depends on gradient concentration and facilitated by the large surface area of the capillary network • The average pressure of the blood capillary (18 mm Hg) is > mean tissue pressure (-6mm Hg), net total pressure=24 mm Hg higher in the capillary over the tissue • This pressure is offset by osmotic pressure=24 mm Hg, pulling the plasma fluid back into the capillary • On average, pressure in tissue = pressure in capillary ≈ no net flow of water • At the arterial end, the blood enters the capillary, the pressure at the capillary slightly> than tissue – fluid leave the capillary into the tissue – hydrostatic or filtration pressure • The filtrate water later returned to the venous capillary due to lower venous pressure than tissue called absorptive pressure • A small amount of fluid return to the circulation through the lymphatic system Distribution Space • Intracellular space, 75% of BW: - intracellular fluid - solid cell compound • Extracellular space, 22% - plasma water 4% BW (intravascular fl) - interstitial fluid 16-20% BW (easily difusable interstitial fluid and poorly difusable fluid in skin, muscle, cartilage, bone connective tissue) - trancellular fluid, 1.5% BW (cerebrospinal, eye, synovial, perilymph, endolymph, sinuses and small cavity fluid) , Distribution half-life, Blood flow, Drug uptake by Organ • Drug transfer from the capillary into the tissue fluid is mainly diffusion process : h, D, (Cp-Ct) are important factors in determining the rate of drug diffusion. If drug distribution is limited by the slow diffusion, the process is diffusion / permeability limited • If drugs diffuse rapidly across the membrane that blood flow is a rate limiting step in the distribution of drug, the process is perfusion / flow limited. Congestive heart failure - reduced filtration pressure and blood flow In disease condition: • Drug with permeability limited : increased distribution volume that cause inflammation and increased capillary membrane permeability • Renal/hepatic disease : osmotic pressure balance may be altered due to albumin/ blood loss/changes in electrolyte levels, resulting in net flow of plasma water into the interstitial space (edema) • This change in fluid distribution may partially explain the increased extravascular drug distribution during some disease states • Drug Affinity for a tissue/organ = partitioning and accumulation of the drug in tissue • The Distribution half-life or time for 50% distribution= the time for drug distribution • The factors that determine the distribution constant of drug into an organ are related to: - blood flow - volume of the organ - partitioning of the drug into the organ • • • • • • • • • kd = Q / V R kd = first order distribution constant Q = blood flow to the organ V = volume of the organ R = ratio of drug concentration in the organ tissue to drug concentration in the blood (venous) td1/2 = 0.693/ kd R determined experimentally from tissue samples (the data is only from animal tissue) R ≈ Po/w If each tissue has the same ability to store the drug, then kd is only governed by Q and V. If Q is large, decreases the distribution time, whereas if V is large, increases the distribution time because a longer time is needed to fill a Drug Accumulation • The deposition or uptake of the drug into the tissue is controlled by the diffusional barrier of the capillary membrane and other cell membrane • The brain is well perfused with blood, but many drugs with good aqueous solubility which have high kidney, liver and lung concentrations, yet little brain drug concentration. • The brain capillaries are surrounded by a layer of tightly joined glial cells that act as a lipid barrier to impede the diffusion of polar or highly ionized drugs. • A diffusion limited model may be necessary to describe the pharmacokinetics of these drugs that are not adequately described by perfusion models • The accumulation of drug into tissues is dependent on: - the blood flow - the affinity of the drug for the tissue • Drug uptake into a tissue is generally reversible • The drug concentration in a tissue with low capacity equilibrates rapidly with the plasma drug concentration and then declines rapidly as the drug is eliminated • Drugs with high tissue affinity tend to accumulate or concentrate in the tissue • Drugs with a high lipid /water coefficient partition are very fat soluble and tend to accumulate in lipid or adipose tissue Lipid soluble drugs and accumulation • Partition from plasma (aqueous) into the fat tissue with reversible process. • Extraction of drug out of the tissue is very slow, remain 6-7 days in adipose tissue, long after the drug is depleted from the blood • Adipose tissue is poorly perfused with blood – drug accumulation is slow • Once the drug is concentrated in fat tissue, drug removal from fat may also be slow • To achieve the desired pharmacological effect, need a large initial bolus of drug • The distribution of lipophilic drugs will be different in thin versus obese patients • Some drugs are irreversibly bound to tissue protein with covalent bound: purine and pyrimidine drugs used in cancer chemotherapy are incorporated into nucleic acids, causing destruction of the cell • DDT: highly lipid soluble, remain years in fat tissue • Drug accumulate in tissue - binding to protein tissue: Digoxin – highly binding to protein in cardiac tissue – leading in a large volume of distribution ( 440 L / 70 kg) and long t1/2 (40 hrs) • Some drugs complex with melanin in the skin and eye after long term administration of high doses of phenothiazine to chronic schizophrenic patients • Tetracycline – forms an insoluble chelate with calcium on teeth and bones • Amphetamin (phenilethylamine structure) ≈ norepinephrine, is actively transported into and accumulated in adrenergic tissue (a specific uptake system for catecholamin/ norepinephrine) Permeability of Cell and Capillary Membranes • Cell membrane vary in their permeability characteristics, depending on the tissue • Liver and kidney: more permeable to transmembrane movement than capillaries in the brain. The sinusoidal capillaries of the liver are very permeable and allow the passage of large-molecular-weight molecules • In the brain and spinal cord, the capillary endothelial cells are surrounded by a layer of glial cells, which have tight intercellular junctions, acts effectively to slow the rate of drug diffusion into the brain by acting as a thicker lipid barrier • This lipid barrier, which slows the diffusion and penetration of water-soluble and polar drugs into the brain and spinal cord, is called the blood brain barrier • The diameters of the capillaries are very small and the capillary membranes are very thin. The high blood flow within a capillary allows for intimate contact of the drug molecules with the cell membrane, providing for rapid drug diffusion • For capillaries that perfuse the brain and spinal cord, the layer of glial cells functions effectively to increase the thickness of term h in Fick’s equation, there by slowing the the diffusion and penetration of water soluble and polar drugs into the brain and spinal cord • In disease, the permeability of cell membranes, including capillary cell membranes, may be altered by burns (on the skin-large molecules can permeate inward or outward), inflammation (meningitis) – drug uptake into the brain will be enhanced Apparent Volume of Distribution • The concentration of drug in plasma or tissues depends on the amount of drug systematically absorbed and volume in which the drug is distributed • Apparent volume of distribution, VD = the volume in which the extent of drug distributed in the body, represents the result of dynamic drug distribution between the plasma and the tissues and accounts for the mass balance of the drug in the body • The volume of the system may be estimated if the amount of drug added to the system and the drug concentration after equilibrium in the system are known • Volume of distribution, ( VD , L) = amount (mg) of drug in body/drug concentration (C, mg/L) in plasma after equilibrium Apparent Volume of Distribution, Vapp Vapp is different from VDss (compartment model) Vapp = DB / CP DB = VPCP + VtCt DB = amount of drug in the body; VP = plasma fluid volume; Vt = tissue volume; CP = plasma drug concentration; Ct = tissue drug concentration • For many protein bound drugs, the ratio DB/CP is not constant every time, depends on the nature of dissociation of the protein-drug complex and how the drug is distributed; the ratio is best determined at steady state. • Protein binding to tissue – apparent volume of distribution increase. Some models: the drug distributes from the plasma water into extracellular tissue fluid, where the drug binds to extravascular proteins, resulting in a larger VD due to extracellular protein binding • • • • • Drugs with polar compound (penicillin, cephalosporin, valproic acid, furosemide) stay mostly within the plasma and extracellular fluids – VD relatively low • Drugs with lower distribution to the extracellular water are more extensively distributed inside the tissues and tend to have a large VD • An excessively high VD (>body volume of 70 L) is due mostly to special tissue storage, tissue protein binding, carrier, or efflux system which removes drug from the plasma fluid : Digoxin, is bound to myocardial membrane • The high tissue binding is responsible for the large steady state volume of distribution • The greater drug affinity also results in longer distribution α half-life in spite of the heart’s great vascular blood perfusion • Imipramin is highly protein bound and concentrated in plasma, yet its favorable tissue partition and binding accounts for a large volume of distribution. • TCA – large volume of distribution due to tissue (CNS) penetrating and binding Physicochemical Nature of group of drug related to Drug Distribution • Drug distributed only in plasma • Drug distributed in plasma and extracellular fluid • Drug distributed in plasma, extracellular fluid and intracellular fluid Drugs which have VD of 12 L : distributed in extracellular fluid but not penetrated the cell Drugs which have VD of 3 L (the plasma protein binding are high, MW are high) : distributed only in vascular compartment Determinant of Drug Distribution • • • • • • • Organ blood flow Barriers to drug diffusion Adipose tissue – drug accumulation Tissue protein binding Plasma protein binding Drug transport Ion trapping