Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
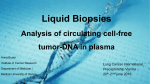
172 Salvage MET amplification detection and therapy through cell-free DNA NGS in a progressing lung cancer patient 1 Peled , 1 Belilovski , 2 Soussan-Gutman , 3 Lanman , 3 Talasaz Nir Anna Lior Richard B. AmirAli 1 2 3 Affiliation: Tel Aviv University, Tel Aviv, Israel; Oncotest Teva, Teva Pharmaceuticals, Shoham, Israel; Guardant Health, Inc., Redwood City, CA Background • Genotyping of metastatic non-small cell lung cancer (NSCLC) has become standard of care, targeting the canonical driver mutations in seven genes: EGFR, BRAF, ERBB2 (HER2), MET and fusions in ALK, RET, and ROS1. • NCCN guidelines also recommend repeat tissue biopsy in patients progressing on EGFR inhibitors to identify targetable resistance mutations such as EGFR T790M, MET amplification, etc.1 • Targeted next generation sequencing (NGS) of cell-free circulating tumor DNA (ctDNA) may identify druggable resistance mechanisms without an invasive tissue biopsy, or when tissue is obtained but DNA quantity is not sufficient (QNS) for analysis. Results Figure 1. B • CtDNA NGS testing identified a high-level MET amplification (copy number of 53.6 in circulation) (Figure 1A). • The test was repeated on a second tube of blood submitted at the same time point, with the second test showing a similar MET gene copy number (60.0). • Crizotinib was prescribed to target the MET amplification with immediate clinical improvement and a significant imaging response on CT/PET scans (Figure 1B). • Three months after start of treatment the patient is fully active, able to carry on all pre-disease performance without restriction (ECOG Performance Status = 0) and is symptom-free. Crizotinib Case • A 70-year-old former light smoker (15 packs/year) with pulmonary fibrosis and moderate pulmonary hypertension was diagnosed with a 30 mm right middle lobe stage IIIA lung adenocarcinoma and treated with definitive chemoradiotherapy. After five months, mediastinal, liver, and multiple bone metastases were diagnosed. After two months of treatment with a targeted therapeutic regimen (afatinib) for a rare EGFR mutation (I744F), a significant progression occurred. The patient was not a candidate for chemotherapy and there was no tissue available for molecular testing. Methods • CtDNA testing was performed with a 70Table 1. gene ctDNA NGS panel (Guardant360™, Table 1) that includes all NCCNrecommended somatic genomic variants for solid tumors and completely sequences the critical exons in 70 genes to identify all four major types of genomic alterations: single nucleotide variants (SNVs), selected indels and fusions, and copy number amplifications (CNA) in 16 genes with high sensitivity (85% in stage III/IV solid tumors) and ultra-high specificity (>99.9999%).2 • CNA for MET and other genes have been validated against cell lines with known amplifications and are reported as 1+, 2+ or 3+ with the latter representing the absolute copy number of the gene in blood at the 90th percentile and higher. Conclusions 1. Analysis of ctDNA in this metastatic NSCLC cancer patient identified MET gene amplification and the patient had a dramatic response to crizotinib. 2. Liquid biopsy methods such as ddPCR may identify EGFR T790M, but NGS methods may be required to detect the other 50% of the secondary resistance mechanisms (Figure 2), such as MET amplification - which occurs in 5% of patients on EGFR inhibitors.3 3. CtDNA detection of MET amplification as a key resistance mechanism after EGFR TKI therapy is feasible with a targeted NGS method when tissue is not accessible or biopsy performed but was QNS for genotyping. References 1 Ettinger DS. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) NonSmall Cell Lung Cancer Version 4.2016. January 2016. www.nccn.org. 2 Lanman RB, Mortimer SA, Zill OA, et al. Analytical and Clinical Validation of a Digital Sequencing Panel for Quantitative, Highly Accurate Evaluation of Cell-Free Circulating Tumor DNA. PloS One. 2015;10(10):e0140712. 3 Camidge DR, Pao W, Sequist LV. Acquired resistance to TKIs in solid tumours: learning from lung cancer. Nat Rev Clin Oncol. 2014;11(8):473-481. Figure 2. PIK3CA mutation 5.0% MEK1 (MAP2K1) mutation 5.0% KRAS mutation 1.0% EML4-ALK and other fusions 1.0% Other 3.3% EMT to SCLC RB1 loss or inactivating mutation6.0% NF1 loss or inactivating mutation 1.0% PTEN loss or inactivating mutation 4.0% EGFR T790M 50.0% BRAF mutation 1.0% FGFR3 fusions 0.6% ERBB3 (HER3) amp or mutation 2.0% ERBB2 (HER2) amp 12.0% MET amp 4.0% EGFR exon 20 EGFR L747S, insertion D761Y, T854A, 0.1% 4.0%