Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
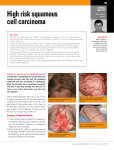
PATIENT INFORMATION Squamous cell carcinoma Bald scalp in men excision lines Method of excision of BCC the spot if it appears to be an obvious SCC. What is squamous cell carcinoma (SCC)? Squamous cell carcinoma is the second-most common form of skin cancer It is a serious form of skin cancer in which cells in the epithelial layer (skin surface) of the skin develop into a malignant tumour. What is the cause of SCC? The two main factors in causation are sun exposure and skin type (fair skin that tans poorly and burns easily). As with other types of skin cancer, years of exposure to the UV rays of the sun is the main cause. Long-term damage to these surface cells triggers the growth of abnormal cells. The causes can be summarised as follows: l Excessive exposure to sunlight (most cases). l Skin damage by radiation. l Exposure to coal tar and various industrial tar products (uncommon). l Exposure to chemicals such as arsenic and polycyclic hydrocarbons. Queensland has the highest rate of skin cancer in the world. Who gets SCCs? Any person can get an SCC but it is more common with increasing age and in men, which may reflect more exposure to sunlight. The risk increases with: l Age older than 60. l Fair complexion. * Common sites of squamous cell carcinoma Outdoor occupation. Development of sunspots (solar keratoses). The problem is rare in people with dark skin. Sunspots (solar keratoses) are dry, rough, persisting spots on the skin which can change into an SCC and need to be watched and treated if they alter appearance. l l Where do SCCs usually occur? They usually develop in skin exposed to the sun, particularly the face (especially the lower lip), ears, neck, forearms, back of the hands and lower legs. In older men they can occur on the scalp. A whitish thick patch on the lip (especially lower lip) may be the forerunner of an SCC. What are the symptoms and signs? The first sign is a thick fleshy lump with crusting that appears on the skin and grows steadily. It may look like a wart or small ulcer at first. It becomes crusty and may bleed. The lump is not usually painful or itchy, although it may be tender to gentle squeezing. What are the risks? This cancer has to be treated with considerable respect. If it is allowed to grow unchecked, it may spread to other parts of the body by “seeding” through blood vessels or lymphatic channels. If this metastatic effect occurs, the outlook is very poor. However, if the problem is detected early, treatment is simple and effective and the outlook is excellent. What should be done? It is important to visit your local doctor without delay if you develop a suspicious skin spot for no apparent reason. If considered suspicious, the doctor may want to remove a small sample for laboratory microscopic analysis (a biopsy) or may completely excise How can SCCs be prevented? Protect yourself from the sun: l Try to avoid direct sunlight when the sun is strongest (eg, 10am to 2pm standard time). l Wear a broadbrimmed hat, T-shirt and baggy shorts in the sun. l Use a factor 15+ or more sunscreen on exposed skin. l Wear a shirt or dress with sleeves. l Be wary of reflected sun on cloudy days. l Don’t be fooled by a cooling breeze — you may still be exposed to UV rays. What is the treatment? Most SCCs are easily removed by a minor surgical operation in which the total spot is removed along with a small margin of about 3-5mm of skin to ensure all the malignant cells are removed. When the tumour is large, a skin graft will be needed to cover the remaining defect. Other treatments are radiotherapy, laser therapy and cryosurgery (freezing of the tumour). More than 99% of patients are completely cured by this treatment. Regular check-ups are recommended during the next few years to detect if any of the cancer remains. If this is the case, the treatment is repeated. Acknowledgment to Professor Robin Marks. AUTHOR: PROFESSOR JOHN MURTAGH Copyright of Professor John Murtagh and Australian Doctor. This patient handout may be photocopied or printed out by a doctor free of charge for patient information purposes.