Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
5-HT3 antagonist wikipedia , lookup
Pharmacognosy wikipedia , lookup
NMDA receptor wikipedia , lookup
Toxicodynamics wikipedia , lookup
5-HT2C receptor agonist wikipedia , lookup
Discovery and development of angiotensin receptor blockers wikipedia , lookup
Drug interaction wikipedia , lookup
Cannabinoid receptor antagonist wikipedia , lookup
NK1 receptor antagonist wikipedia , lookup
Neuropharmacology wikipedia , lookup
Nicotinic agonist wikipedia , lookup
PHL 313 & 315
Pharmacology I
Parasympathetic drugs
Dr. Naglaa F. El-Orabi,
Department of Pharmacology &Toxicology
College of Pharmacy,
King Saud University,
Riyadh, KSA
Lecture 1
10/17/2015
Dr. Naglaa F. El-Orabi
Reference Textbook
• “ Rang & Dale’s Pharmacology”. By
Rang HP, Dale MM, Ritter JM, Moore
PK, eds. 7th ed., Elsevier Science,
2012.
• “ Basic & Clinical Pharmacology”. By
Katzung BG ed. 12th ed., The
McGraw-Hill Companies, Inc., 2012.
• “Pharmacology
(Lippincott
Illustrated Review) ” . 5th ed., 2011
10/17/2015
Dr. Naglaa F. El-Orabi
Cholinergic
transmission
10/17/2015
Dr. Naglaa F. El-Orabi
Introduction
Regulation of Body Functions
There are two major systems that control body functions; the nervous
system(NS) and the endocrine system
These two systems have several common properties, which include:
high-level integration in the brain
the ability to influence processes in distant regions of the body
extensive use of negative feedback
both systems use chemicals for the transmission of information
In the nervous system, chemical transmission occurs between nerve
cells and between nerve cells and their effector cells
Chemical transmission takes place through the release of small
amounts of transmitter substances from the nerve terminals into the
synaptic cleft
The transmitter crosses the cleft by diffusion and activates or inhibits
the postsynaptic cell by binding
to F.aEl-Orabi
specialized receptor molecule
10/17/2015
Dr. Naglaa
Introduction (Cont’d)
• The nervous system is a network of specialized
cell that communicate information about an
animal's surroundings and itself.
• It processes this information and causes reactions
in other parts of the body.
• The nervous system is divided broadly into two
categories: the central nervous system (CNS) and
the peripheral nervous system (PNS) .
• Neurons generate and conduct impulses between
and within the two systems.
10/17/2015
Dr. Naglaa F. El-Orabi
Introduction (Cont’d)
• Autonomic Nervous System (ANS) is
functionally defined as a part of PNS.
10/17/2015
Dr. Naglaa F. El-Orabi
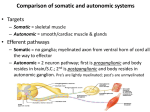
Introduction (Cont’d)
• Somatic nervous system control the motor
function of the body. Neurons innervate skeletal
muscles . Its actions voluntary.
• ANS innervates visceral smooth muscles, cardiac
muscles and glands. It regulates spontaneous
activity of many systems like heart, blood vessels,
respiratory system, digestive organs, urinary sys.,
most glands (endo- & exo-), parts of reproductive
systems (both male & female), etc.
• Mostly automatic action is involuntary.
10/17/2015
Dr. Naglaa F. El-Orabi
Efferent division of the peripheral nervous
system
10/17/2015
Dr. Naglaa F. El-Orabi
Autonomic nervous system
(A) Divisions of the ANS
I-Sympathetic Division
• Mobilize body systems during activity (exertion,
stress, or emergency conditions); (fight and flight
response ). For example:
– Increased pulse & respiratory rate
– Vasoconstriction to skin & viscera
– Sweating (cold sweat)
– Release of adrenalin (epinephrine) from adrenal
medulla
– Inhibition of digestive activity and loss of appetite
10/17/2015
Dr. Naglaa F. El-Orabi
Autonomic nervous system (cont’d)
II- Parasympathetic Division
• Promots body functions during resting or relaxation conditions and
conserve energy (rest and digest response). For example:
– Slower pulse & respiratory rate
– Increased blood flow to skin & viscera
– Increased digestive activity
– Increased reproductive interest, receptiveness
• Penile erection, engorgement of vulva
– SLUDD3D
• Salivation, Lacrimation, Urination, Digestion/Defecation and
3 “decreases”--- decreased HR, diameter of airways and
diameter of pupil .
- Paradoxical fear when there is no escape route or no way to
win causes massive activation of parasympathetic division
10/17/2015
Naglaa F. El-Orabi
and loss of control over Dr.urination
and defecation
10/17/2015
Dr. Naglaa F. El-Orabi
Autonomic nervous system (cont’d)
• Most vital organs receive dual innervation which
means they receive instructions from both the
sympathetic and parasympathetic divisions. The two
divisions often have opposing or antagonistic effects;
one division increases activity of organ, other
division decreases activity of organ (e.g GI smooth
muscles, bladder smooth muscle and heart).
• There are some places ( like salivary glands) where
the two divisions of ANS produce similar rather than
opposing effects (stimulate secretion)
10/17/2015
Dr. Naglaa F. El-Orabi
Autonomic nervous system (cont’d)
• Some organs are supplied with sympathetic only:
– Adrenal medulla, sweat glands, arrector pili
(pilomotor), some kidney’s tissues, some liver
areas(by epinephrine)
– Smooth muscles of most of blood vessels;
arteries, veins and arterioles; (constriction of
most, dilation in skeletal muscles)
10/17/2015
Dr. Naglaa F. El-Orabi
Autonomic nervous system (cont’d)
• Other organs are supplied with
parasympathetic only:
– Ciliary muscle of eye contracts for
accommodation for near vision
– Broncheal smooth muscles
– Erectile smooth muscles of Penis
and clitoris.
– Vaginal lubrication glands
10/17/2015
Dr. Naglaa F. El-Orabi
10/17/2015
Dr. Naglaa F. El-Orabi
Autonomic nervous system (cont’d)
(B) Anatomy
• Two kinds of efferent neurons
– Preganglionic neuron/axon
• Cell body in CNS, axon to autonomic ganglion
(usually. myelinated)
– Postganglionic neuron
• Cell body in ganglion, postganglionic axon to
effector (unmyelinated)
• Ganglia
• Are relay plexi that trnasmit CNS information
via preganglionic to postganglionic nerve fibers.
10/17/2015
Dr. Naglaa F. El-Orabi
Anatomy of ANS (cont.)
Ganglia
Post-ganglionic
neurons
Pre-ganglionic
neurons
Effector organs
10/17/2015
Dr. Naglaa F. El-Orabi
Anatomy of ANS (cont.)
Comparison between sympathetic and parasympathetic divisions of
ANS
10/17/2015
Dr. Naglaa F. El-Orabi
10/17/2015
Dr. Naglaa F. El-Orabi
Autonomic nervous system (cont’d)
(C) Drugs affect the ANS (Types)
• Drugs may mimic or block the effects of the two primary
neurotransmitters, Acetylcholine and Norepinephrine/Epinephrine
• Drugs that mimic the effects of neurotransmitters are referred to as
“Receptor agonists”
- These drugs directly activate receptors
• Drugs that block the effects of neurotransmitters are referred to as
“Receptor antagonists”
- These drugs block the endogenous neurotransmitters from
activating receptors
10/17/2015
Dr. Naglaa F. El-Orabi
Autonomic nervous system (cont’d)
(C) Drugs affect the ANS (Classification)
• Drugs affect Parasympathetic nervous system:
Mimic acetylcholine = cholinergic = muscarinic agonists = Parasympathomimetic
Block acetylcholine = anticholinergic = muscarinic antagonist = Parasympatholytic
• Drugs affect Sympathetic nervous system:
Mimic norepinephrine = adrenergic = adrenergic agonist = Sympathomimetic
Block norepinephrine = antiadrenergic = adrenergic antagonist = Sympatholytic
10/17/2015
Dr. Naglaa F. El-Orabi
Cholinergic transmission
• An important traditional classification of autonomic nerves
is based on the primary neurotransmitter molecules
released from their terminals.
• A large number of peripheral ANS fibers synthesize and
release Ach; they are cholinergic fibers.
• These include all preganglionic efferent autonomic fibers
(both Sympathetic and Parasympathetic) and the somatic
(non-autonomic) motor fibers (NMJs) to skeletal muscle as
well. Thus, almost all efferent fibers leaving the CNS are
cholinergic.
• In addition, most Parasympathetic and some sympathetic
(to sweat glands) postganglionic fibers are cholinergic.
• Ach is also very important neurotransmitter in variuous
10/17/2015
Dr. Naglaa F. El-Orabi
areas in CNS.
I- Parasympathetic Effects
10/17/2015
Dr. Naglaa F. El-Orabi
II-Parasympathetic
anatomy
•
PSNS originates from cranio-sacral
parts of spinal cord.
• Cranial outflow originate from cranial
nerve nuclei in the brain stem.
Preganglionic fibers run via:
– Oculomotor nerve (III)
– Facial nerve (VII)
– Glossopharyngeal nerve (IX)
– Vagus nerve (X)
• These nerve fibers innervate organs of
the head & neck (eye, nasal mucosa,
salivary glands,…), thorax & upper
abdomen ( heart, respiratory system,
esophagus, stomach, pancreas, liver,
small intestine and upper half of the
10/17/2015
Dr. Naglaa F. El-Orabi
large intestine).
II-Parasympathetic
anatomy (Cont’d)
• Sacral outflow originate
from visceral motor region
of spinal cord (S2-S4).
Preganglionic fibers run via
pelvic nerves.
• These
nerve
fibers
innervate organs of the
pelvis and lower abdomen
(lower
half
of
large
intestine,
the
rectum,
urinary and reproductive
systems)
10/17/2015
Dr. Naglaa F. El-Orabi
II- Parasympathetic anatomy (Cont’d)
• Parasympathetic pathway
– Brain areas (hypothalamus & brain stem)
– Cranial or sacral outflow
– Relatively long pre-ganglionic neurons to terminal or intramural
ganglia (in walls of viscera,or close to effector organs)
– Short post-ganglionic neurons.
– All Parasympathetic nerve fiber (both preganglionic postganglionic)
are cholinergic, that is, they work by releasing ACh neurotransmitter.
10/17/2015
Dr. Naglaa F. El-Orabi
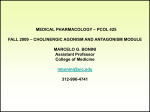
III- Cholinergic transmission
•
•
•
•
•
All
Parasympathetic
nerve
fiber
(both
preganglionic postganglionic) are cholinergic, that
is, they work by releasing ACh neurotransmitter.
Acetylcholine is synthesized in the cytoplasm of
neuronal cells from acetyl-CoA and choline
through the catalytic action of the enzyme choline
acetyltransferase (ChAT).
Acetyl-CoA is synthesized in mitochondria, which
are present in large numbers in the nerve ending.
Choline is transported from the extracellular fluid
into the neuron terminal by a sodium-dependent
membrane carrier (carrier A). The action of the
choline transporter is the rate-limiting step in ACh
synthesis
Carrier A can be blocked by a group of drugs called
hemicholiniums (e.g. HC-3) that are classified
as indirect acetylcholine antagonist)
10/17/2015
Dr. Naglaa F. El-Orabi
III- Cholinergic transmission (Cont’d)
• Acetylcholine is then transported into the storage
vesicle by an antiporter that removes protons
(carrier B). This transporter can be blocked by
Vesamicol wich is classified as cholinergic
physiological antagonist
• Release of transmitter occurs when voltagesensitive calcium channels in the nerve terminal
membrane are opened when an action potential
reaches the terminal and triggers sufficient influx
of Ca2+ ions
• The resulting increase in intracellular Ca2+
destabilizes" the storage vesicles by interacting
with special proteins associated with the vesicular
membrane (VAMPs) causes fusion of vesicles with
the surface membrane and exocytotic expulsion of
acetylcholine into the junctional cleft and interact
with postsynaptic receptors.
• The ACh vesicle release process is blocked by
botulinum
10/17/2015 toxin (neurotoxic protein). Dr. Naglaa F. El-Orabi
III- Cholinergic transmission (Cont’d)
• Acetylcholine's action is terminated by metabolic
degradation by the enzyme acetylcholinesterase
(AChE). AChE splits ACh into choline and acetate,
neither of which has significant transmitter effect,
and thereby terminates the action of the transmitter .
Most cholinergic synapses are richly supplied with
AChEs; the half-life of ACh in the synapse is very brief
(approx. 2min).
• AChE is also found in other tissues, eg, RBCs. Another
cholinesterase with a lower specificity for ACh,
butyrylcholinesterase (pseudocholinesterase) , is
found in blood plasma, liver, glia, and many other
tissues.
• Little or no acetylcholine escapes into the circulation.
Any acetylcholine that reaches the circulation is
immediately inactivated by plasma esterases.
• Many drugs work by inhibiting acetylcholinesterase
(Anticholinesterases) e.g. Neostigmine, thus leading
to excess acetylcholine and indirect cholinoreceptors
stimulation.
10/17/2015
Dr. Naglaa F. El-Orabi
ChAT
ACETYLCHOLINE
B
A
10/17/2015
Dr. Naglaa F. El-Orabi
PHL 313 & 315
Pharmacology I
Parasympathetic drugs
Dr. Naglaa F. El-Orabi,
Department of Pharmacology &Toxicology
College of Pharmacy,
King Saud University,
Riyadh, KSA
10/17/2015
Dr. Naglaa F. El-Orabi
Lecture 2
Types of Cholinergic
receptors
10/17/2015
Dr. Naglaa F. El-Orabi
IV-Cholinergic receptors
• Main subdivisions of cholinergic receptors are nicotinic (nAChR)
and muscarinic (mAChR) subtypes.
• Ach acts as specific agonist for both receptor subclass
• In contrast, because of their unique configurations,Nicotine and
Muscarine are selective for the cholinergic receptor subtypes
whose structure complements their own.
10/17/2015
Dr. Naglaa F. El-Orabi
IV-Cholinergic receptors (Cont’d)
(a) Muscarinic receptors (MACHRs)
•
•
•
•
mAChRs are G-protein-coupled receptors causing:
– activation of PLC (hence ↑IP3, DAG as 2nd
messengers) odd-numbered members (M1, M3,
M5)
– inhibition of adenylyl cyclase (↓cAMP)
even-numbered receptors (M2, M4)
– mAChR also may activate or inhibit of ion (K+ &
Ca2+ ) channels .
mAChRs mediate ACh effects at postganglionic
parasympathetic synapses (mainly heart, smooth
muscle, glands including postganglionic sympathetic
neurons to sweat glands), and contribute to
ganglionic excitation. In addition, they occur in many
parts of the CNS.
Five main types of mAChR occur (M1-5).
All mAChRs are activated by acetylcholine and
blocked by atropine. There are also subtype-selective
10/17/2015
agonists and antagonists.
Dr. Naglaa F. El-Orabi
IV-Cholinergic receptors (Cont’d)
(a)Muscarinic receptors
Receptor
type
Location
MOA
Functional
Response
Stimulatory (↑IP3, DAG,
↑intracellualr Ca2+)
CNS excitation (?memory)
Gastric secretion
(neuronal)
Autonomic ganglia,
Glands ,
CNS (cerebral cortex)
M2
Myocardium, smooth
muscles, some in CNS
Inhibitory (↓cAMP, ↓K+ & Ca2+
conductance)
Cardiac inhibition
Neural inhibition
Central muscarinic effects (e.g.
tremor, hypothermia)
Exocrine glands ,
Smooth muscle (GIT,
eye, airways, bladder)
Vessels endothelium,
Stimulatory (↑IP3,
↑intracellualr Ca2+)
Gastric, salivary secretion GI
smooth muscle contraction
Ocular accommodation
Vasodilatation
CNS
Inhibitory (↓cAMP)
Enhanced locomotion
CNS: very localised in
substantia nigra,
Salivary glands, Eye
(Iris/ciliary muscle)
Stimulatory (↑IP3 Excitation)
Not known
M1
(cardiac)
M3
(glandular ,
smooth muscles)
M4
M5
10/17/2015
Dr. Naglaa F. El-Orabi
10/17/2015
Dr. Naglaa F. El-Orabi
IV-Cholinergic receptors (Cont’d)
(a)Muscarinic receptors
Physiological actions of muscarinic stimulation
Organ
Eye
Heart
Blood vessels
GIT
10/17/2015
Receptor
Action
Circular muscle of
the iris
M3
Contracts
Ciliary muscle
M3
Contracts
SA node
M2
Slows
Myocardium
(Atrium
ventricles)
M2
Negative inotropic (Reduced
contractility) action (more in
atria)
and
negative
chronotropic action
AV node
M2
Reduced conduction velocity
Endothelium
M3
Vasodilatation
Smooth muscle
walls
M3
Contraction ( motility)
Sphincters
M3
Relax
Glands
M3
Secretion
Gallbladder
&
Dr. Naglaa F. El-Orabi
M3
Contraction
IV-Cholinergic receptors (Cont’d)
(a)Muscarinic receptors
Physiological actions of muscarinic stimulation (Cont’d)
Organ
Receptor
Action
Smooth
muscles
M3
Contraction
Glands
M3
Secretion
Wall
(detrusor)
M3
Contracts
Trigone
sphincter
M3
Relax
Pregnant uterus
M3
Contracts
Penis and clitoris
M3
Erection
Glands (Salivary, Lacrimal,
Nasopharyngeal , vaginal
lubrication& Sweat ; symp.
Cholinergic)
M3
Secretion
Bronchi
Urinary bladder
10/17/2015
Dr. Naglaa F. El-Orabi
IV-Cholinergic receptors (Cont’d)
(b) Nicotinic receptors (nAChRs)
• nAChRs are ligand-gated directly coupled
to cation channels (e.g. Na+/K+ channels )
whose activation results in a rapid increase
in cellular permeability to Na+, and
mediate
fast
excitatory
synaptic
transmission at the neuromuscular
junction (Skeletal muscles, autonomic
ganglia, and various sites in CNS.)
• Muscle-type (Nm), and neuronal-type
(Nn) nAChRs are differ in their molecular
structure and pharmacology.
• Both mAChRs and nAChRs occur
presynaptically as well as postsynaptically,
and function to regulate transmitter
10/17/2015
Dr. Naglaa F. El-Orabi
release.
IV-Cholinergic receptors (Cont’d)
(b)Nicotinic receptors
Receptor
type
Location
MOA
Functional
response
Nn
Post ganglionic
neurons of
autonomic
ganglia , some
central nervous
system neurons ,
and adrenal
medulla
Opening of Na+, K+
channels,
depolarization
- Excitation of autonomic
ganglia
- Stimulate Epi, NE from
adrenal gland
- Pre- and postsynaptic
stimulation of many brain
regions
Nm
Skeletal muscle
neuromuscular
endplates
Opening of Na+, K+
channels,
depolarization
Skeletal muscle contraction
10/17/2015
Dr. Naglaa F. El-Orabi
10/17/2015
Dr. Naglaa F. El-Orabi
(α1)2β1δγ
10/17/2015
Dr. Naglaa F. El-Orabi
V- Modifying Parasympathetic Nervous
System Function
1-Parasympathomimetics
=
Cholinomimetic drugs:
Act directly or indirectly with
acetylcholine receptors (Muscarinic
& Nicotinic) and stimulates them or
enhance cholinergic transmission by
other mechanism:
• Muscarinic agonists (stimulants) e.g.
Bethanechol and Pilocarpine
• Anticholinesterases
(e.g.
Physostigmine and Neostigmine) and
other drugs that enhance cholinergic
transmission (e.g. Aminopyridines).
• Ganglion-stimulating drugs
e.g.
Nicotine and lobeline
10/17/2015
Dr. Naglaa F. El-Orabi
B
C
h
A
T
ACETYLCHOLINE
A
Muscarinic
ptors
Muscarinic
antagonists
V- Modifying Parasympathetic Nervous
System Function (Cont’d)
2-Parasympatholytics
(a) Direct cholinergic antagonists – anticholinergic
drugs: bind to acetylcholine receptors and
reduce the effects of parasympathetic
stimulation
by
preventing
endogenous
acetylcholine from binding to them:
• Muscarinic antagonists
e.g. Atropine and
Scoplamine
• ganglion-blocking drugs e.g. Mecamylamine and
Trimetaphan
• Neuromuscular-blocking drugs e.g. Tubocurarine
and Gallamine
(b) Indirect anticholinergic drugs:
•
Precursor
transport
blockade,
e.g.,
Hemicholinium
• Choline
acetyltransferase
inhibition,
…………no clinical example
• Promote transmitter release, e.g., choline,
black widow spider venom (Latrotoxin)
• Prevent transmitter release, e.g., Botulinum
toxin
• Prevent storage, e.g., Vesamicol prevents
10/17/2015
Dr. Naglaa F. El-Orabi
ACh storage
PHL 313 & 315
Pharmacology I
Parasympathetic drugs
Dr. Naglaa F. El-Orabi,
Department of Pharmacology &Toxicology
College of Pharmacy,
King Saud University,
Riyadh, KSA
10/17/2015
Dr. Naglaa F. El-Orabi
Lecture 3
cholinomimetic
drugs
Muscarinic agonists
10/17/2015
Dr. Naglaa F. El-Orabi
VI- Parasympathomimetics
1-Muscarinic receptor stimulants
Choline Esters
Direct
Cholinomimetic
alkaloids
Muscarinic
stimulants
Indirect
10/17/2015
Dr. Naglaa F. El-Orabi
Cholinesterase inhibitors
VI- Parasympathomimetics (Cont’d)
(a) Direct cholinoceptor stimulants
1-Choline esters
e.g. Acetylcholine, Methacholine, Carbachol and Bethanechol
2- Colinomimetic alkaloids
e.g. Muscarine, Oxotremorine and Pilocarpine
•
Many of these muscarinic agonists are used as experemintal tools
e.g. Acetylcholine, and Muscarine.
•
Other muscarinic agonists like Bethanechol, Methacholine,
Carbachol,and Pilocarpine are in clinical use.
•
Use of muscarinic receptor agonists, is contraindicated in patients
with asthma, coronary insufficiency, urinary incontinence and
10/17/2015
Dr. Naglaa F. El-Orabi
peptic ulcers
Drug
Receptor specificity
Hydrolysis
by AChE
Clinical
uses
Musc
Nic
Acetylcholine
+++
+++
+++
None
Carbachol
++
+++
-
None
Methacholine
+++
+
++
None
Bethanechol
+++
-
-
Bladder* and
Gl hypotonia
Muscarine
+++
-
-
None†
Pilocarpine
++
-
-
Glaucoma
Oxotremorine
++
-
-
None
• ACh itself is rnot used clinically because of its rapid hydrolysis following oral
ingestion and rapid metabolism following i.v. administration ( t ½ ᷉ 2 min)
10/17/2015
Dr. Naglaa F. El-Orabi
VI- Parasympathomimetics
(a)Direct cholinoceptor stimulants (Cont’d)
1- Bethanechol (Urecholine)
• Selectively stimulates muscarinic receptors
(with further selectivity for M3 receptors)
• Unlike acetylcholine, bethanechol is not
hydrolyzed by cholinesterase and will
therefore have a long duration of action
• Clinical uses:
1. To assist bladder emptying in non-obstructive urinary
retention resulting from general anesthetic or diabetic
neuropathy of the bladder
2. To treat gastroparesis (delayed gastric emptying), because it
stimulates GI motility and secretion
3. To stimulate salivary gland secretion in patients with
10/17/2015
Dr. Naglaa F.passages,
El-Orabi
xerostomia (dry mouth, nasal
and throat)
VI- Parasympathomimetics
(a)Direct cholinoceptor stimulants
1- Bethanechol (Cont’d)
Side Effects associated with bethanechol therapy:
1.Abdominal cramps or discomfort
2.Nausea and diarrhea
3.Excessive salivation
4.Hypotension and bradycardia
5.Urinary urgency
6.Bronchial constriction and asthmatic attacks
10/17/2015
Dr. Naglaa F. El-Orabi
VI- Parasympathomimetics
(a)Direct cholinoceptor stimulants (Cont’d)
2- Pilocarpine (Salagen)
Indications: It is more commonly used than
bethanechol to induce salivation, and also for
various purposes in ophthalmology.
1. Treatment of primary or acute glaucoma
and also to lower IOP prior to surgery for
acute glaucoma by local instillation in the
form of eye drops.
2. Treatment of symptoms of dry mouth
from salivary gland hypofunction caused
by radiotherapy for cancer of the head
and neck (xerostomia )
10/17/2015
Dr. Naglaa F. El-Orabi
VI- Parasympathomimetics
(a)Direct cholinoceptor stimulants
2- Pilocarpine(Cont’d)
Side Effects associated with pilocarpine therapy:
Most of them are related to its non-selective action as a muscarinic
receptor agonist
1.Excessive sweating
2.Excessive salivation
3.Bronchospasm and increased bronchial mucus secretion
4.Bradycardia, hypotension
5.Nausea and diarrhea
6.It may result in miosis when used chronically as an eye drop
10/17/2015
Dr. Naglaa F. El-Orabi
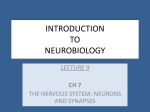
Muscarinic effects on the eye
Normal:
Accommodation:
Ciliary Muscle Relaxed
Ciliary Muscle Contracts
Suspensory Ligaments Under Tension
Reduced Tension on Suspensory Ligaments
Lens becomes Round
10/17/2015 Lens is Flattened
Dr. Naglaa F. El-Orabi
Focus on Distant Objects
Focus on Near Objects
Muscarinic effects on the eye (Cont’d)
The smooth muscles of the iris:
• The sphincter muscle is
innervated by M3 receptors. Its
contraction under the influence
of muscarinic
agonist (e.g.
pilocarpine) results in miosis,
and its blockade by muscarinic
antagonist
(e.g.
atropine)
results in mydriasis.
• On the other hand, the radial
muscle is innervated by α-1
receptor. Its contraction by an
agonist results in mydriasis and
10/17/2015
Dr. Naglaa F. El-Orabi
its blockade results in miosis.
Sphincter
muscle
Radial
muscle
Muscarinic effects on the eye (Cont’d)
What is Glaucoma?
•
Glaucoma is an eye disorder in which the optic nerve
suffers damage, permanently impacting vision in the
affected eye(s) and progressing to complete
blindness if untreated.
• It is often associated with increased pressure of the
aqueous humour in the eye (Intraocular pressure
“IOP”).
• The aqueous humour is a thick watery substance
filling the space between the lens and the cornea. It
is rich in amino acid, glucose, antioxidants , and
immunoglobulins. Its main role to maintains IOP and
keep the eyes slightly distended. In addition to
providing nutrition and protection for the occular
tissues
• Aqueous humour is secreted into the posterior
chamber by the ciliary body epithelium, it flows in
through the pupil to the anterior chamber, and then
to drain out of the eye via Schlemm's canal into the
10/17/2015
Dr. Naglaa F. El-Orabi
veins of the orbit.
Muscarinic effects on the eye (Cont’d)
• Glaucoma is a condition characterised by increased IOP either through
increased production and/or decreased outflow of aqueous humour.
• The intraocular pressure is normally 10-15 mmHg above atmospheric.
Abnormally raised intraocular pressure (associated with glaucoma)
damages the eye and is one of the commonest preventable causes of
blindness
• Increased resistance to outflow of aqueous humour may occur due to
an injury or disease of the iris.
• In acute glaucoma (closed angel glaucoma) , drainage of aqueous
humor becomes obstructed when the pupil is dilated that folding of the
iris tissue occludes the drainage angle causing the IOP to rise.
• Stimulation of iris sphincter muscle by a muscarinc agonist (e.g.
pilocarpine) in this circumstance will lead to lowering in the IOP.
10/17/2015
Dr. Naglaa F. El-Orabi
Major drugs used in treatment of Glaucoma
Drug
Ecothiopate,
Pilocarpine
Timolol,
carteolol
Acetazolamide
dorzolamide
Brimonidine
Clonidine,
apraclonidine
Pratanoprost,
Travoprost
10/17/2015
Mechanism
Cholinomimetics
Notes
work by contraction of the iris sphinctr muscle (miosis)
and ciliary muscl that tightening the trabecular
meshwork and allowing increased outflow of the
aqueous humour. Widely used as eye drops. Can cause
muscle spasm and systemic effects.
β-Adrenoceptor
decrease aqueous humor production by the ciliary
antagonist
body epithelium. Given locally as eye drops but may
still cause systemic side effects: bradycardia,
bronchoconstriction.
Carbonic anhydrase
lower secretion of aqueous humor by inhibiting
inhibitor
carbonic anhydrase in the ciliary body epithelium
Acetazolamide is given systemically. Side effects
include diuresis, loss of appetite, tingling, neutropenia.
Dorzolamide is used as eye drops. Side effects include
bitter taste and burning sensation.
α2-Adrenoceptor
work by a dual mechanism, decreasing aqueous humor
agonist
production and increasing trabecular outflow. Used
locally as eye drops
Prostaglandin
Increase aqueous humor outflow. Given locally as eye
analogue
Can cause ocular pigmentation
Dr. drops.
Naglaa F. El-Orabi
PHL 313 & 315
Pharmacology I
Parasympathetic drugs
Dr. Naglaa F. El-Orabi,
Department of Pharmacology &Toxicology
College of Pharmacy,
King Saud University,
Riyadh, KSA
10/17/2015
Dr. Naglaa F. El-Orabi
Lecture 4
cholinomimetic
drugs
Cholinesterase inhibitors
10/17/2015
Dr. Naglaa F. El-Orabi
VI- Parasympathomimetics
1-Muscarinic receptor stimulants (Cont’d)
Choline Esters
Direct
Cholinomimetic
alkaloids
Cholinoceptor
stimulants
Indirect
10/17/2015
Dr. Naglaa F. El-Orabi
Cholinesterase inhibitors
VI- Parasympathomimetics (Cont’d)
(b) Indirect cholinoceptor stimulants
• Drugs that enhance cholinergic transmission act either by
inhibiting cholinesterase or by increasing ACh release.
• Example of drugs that enhance cholinergic transmission via
increase of Ach release:
Aminopyridines, which block K+ channels and thus prolong
the action potential in the presynaptic nerve terminal.
• These drugs are not in clinical use due to lack of selectivity
for cholinergic nerves but increase the evoked release of
many different transmitters, so have too many unwanted
effects to be useful in treating neuromuscular disorders.
10/17/2015
Dr. Naglaa F. El-Orabi
VI- Parasympathomimetics
(b) Indirect cholinoceptor stimulants (Cont’d)
Cholinesterase inhibitors
• Indirect-acting agents produce their primary effects by
inhibiting
acetylcholinesterase,
which
hydrolyzes
acetylcholine to choline and acetic acid by forming a complex
with
acetylcholinesterase
enzyme
.By
inhibiting
acetylcholinesterase, the indirect-acting drugs increase the
endogenous ACh concentration in synaptic clefts and
neuroeffector junctions. The excess ACh, in turn, stimulates
cholinergic receptors to evoke increased responses. These
drugs act primarily where ACh is physiologically released and
are thus amplifiers of endogenous ACh.
• Some
cholinesterase
inhibitors
also
inhibit
butyrylcholinesterase (pseudocholinesterase).
10/17/2015
Dr. Naglaa F. El-Orabi
VI- Parasympathomimetics
(b) Indirect cholinoceptor stimulants
Cholinesterase inhibitors (Cont’d)
The inhibitory effect of anticholinesterases may be:
• Reversible: as that produced by Edrophonium,
Pyridostigmine, Physostigmine (Eserin) or
Neostigmine
• Irreversible: such as Echothiophate and
Malathion (orgonophosphorus compounds).
10/17/2015
Dr. Naglaa F. El-Orabi
VI- Parasympathomimetics
(b) Indirect cholinoceptor stimulants
Cholinesterase inhibitors (Cont’d)
Alcohols
Carbamic acid esters
Organophosphates
1- Edrophonium
1- Neostigmine
2-Pyridostigmine
2- Physostigmine (eserine)
1- Echothiophate
2-Isoflurophate(Dyflos)
3-Soman,
4-Parathion,
5- Malathion
The action of the drug is very
brief. It is used mainly for
diagnostic
purposes
(myasthenia gravis )
Neostigmine
and
Pyridostigmine are
not
absorbed and does not enter
CNS
Physostigmine is absorbed
from all sites including
conjunctiva and enters CNS
All organophosphorous compounds
are well absorbed from all sites of
administration and enter the CNS
except echothiophate
Most of these compounds developed
as war gases (e.g Sarin;nerve gas)
and pesticides (e.g. Malathion and
Parathion) as well as for clinical use
(e.g. Ecothiophate and Isoflurophate)
Reversible inhibition after 2-10
min (short-acting
anticholinesterases)
Reversible inhibition after 30
min to 6 hours (intermediateacting anticholinesterases)
Irreversible inhibition (can be
reversed by Pralidoxime)
10/17/2015
Dr. Naglaa F. El-Orabi
VI- Parasympathomimetics
(b) Indirect cholinoceptor stimulants
Cholinesterase inhibitors (Cont’d)
• Pharmacological effects:
CNS
Tertiary compounds, such as physostigmine, and the non-polar organophosphates
penetrate BBB and affect the brain
Low concentrations cause alertness. High concentrations cause initial stimulation,
restlessness, anxiety and convulsions followed by depression and coma.
Autonomic
cholinergic
synapses:
(Eye, GIT,
Bronchioles, and
urinary bladder
Cardiovascular
system,
glands…etc)
Increased secretions from salivary, lacrimal, bronchial and gastrointestinal glands;
increased peristaltic activity; bronchoconstriction; bradycardia and hypotension;
pupillary constriction; fixation of accommodation for near vision; fall in intraocular
pressure.
Acute anticholinesterase poisoning causes severe bradycardia, hypotension and
difficulty in breathing
Neostigmine and pyridostigmine tend to affect neuromuscular transmission more
than the autonomic system, whereas physostigmine and organophosphates show the
reverse pattern.
Neuromuscular
junction
Therapeutic doses increases strengh of contraction
In large doses, such as can occur in poisoning, anticholinesterases initially cause
muscle twitching and fibrilation. Later, paralysis may occur due to depolarisation
Dr. with
Naglaathe
F. El-Orabi
block, which is associated
build-up of ACh in the plasma and tissue fluids.
10/17/2015
VI- Parasympathomimetics
(b) Indirect cholinoceptor stimulants
Cholinesterase inhibitors (Cont’d)
• Therapeutic uses:
Disease
Mechanism of action
Drug
1- Glaucoma
Contraction of the ciliary muscle and circular sphinctor Physostigmine
muscle of the iris that increasing the outflow of the echothiophate
aqueous humor
(as eye drops)
2- Postoperative
To reverse the action of
neuromuscular-blocking drugs.
3- Urinary retention
Non-obstructive urine retention
4- Myasthenia gravis
a-treatment
non-depolarising
neostigmine
neostigmine
neostigmine,
pyridostigmine
b-test for myasthenia
gravis
and
to
distinguish
weakness
caused
by edrophonium
anticholinesterase overdosage ('cholinergic crisis')
from the weakness of myasthenia itself ('myasthenic
crisis'):
5- Dementia like
Alzheimer's dieases
cholinesterase inhibitors may act to reduce donepezil, tacrine
neurotoxicity by inhibiting formation of Aβ, and rivastigmine and
therefore the progression of AD as well as producing galantamine
Dr. Naglaa F. El-Orabi
symptomatic benefit
10/17/2015
VI- Parasympathomimetics
(b) Indirect cholinoceptor stimulants
Cholinesterase inhibitors (Cont’d)
Side Effects and toxicity:
Acute toxicity (cholinergic crisis):
Treated by Atropine and Pralidoxime
A- miosis, nausea, vomiting, diarrhea, salivation,
sweating, lacrimation cutaneous vasodilation, and
bronchial constriction and excessive urination
B- These manifestations are followed by:
(1)central stimulation, which cause convulsions and may
progress to coma and respiratory arrest;
(2) skeletal muscle paralysis
(3)hypertension and cardiac arrhythmias.
10/17/2015
Dr. Naglaa F. El-Orabi
What is Myasthenia gravis ?
• Myasthenia gravis (MG) is a pathological disorder affecting
skeletal muscle (NMJs).
• It is resulting of an autoimmune disorder causes production of
antibodies that decrease the number of functional nicotinic
receptors (nAChRs) on the motor end plates leading to inhibiting
the stimulative effect of the neurotransmitter acetylcholine.
10/17/2015
Dr. Naglaa F. El-Orabi
Myasthenia gravis (Cont’d)
• It is charecterized by fluctuating
muscle weakness and fatiguability.
Symptoms include ptosis, diplopia,
difficulty
in
speaking
and
swallowing, and extremity limbs
weakness
especially
during
repetitive activity. . Severe disease
may affect all the muscles,
including those necessary for
respiration.
10/17/2015
Dr. Naglaa F. El-Orabi
Myasthenia gravis (Cont’d)
Edrophonium test:
• The "edrophonium test" is infrequently performed to identify MG. An IV
dose of of edrophonium chloride (reversible anticholinesterase) is
administere. In people with myasthenia gravis involving the eye muscles,
edrophonium chloride will briefly relieve weakness that lasts about 5
minutes.
• Treatment:
(a)Pharmacotherapy:
1- Acetylcholinesterase inhibitors: like neostigmine and pyridostigmine can
improve muscle function . Side effects, like perspiration and diarrhea can
be countered by adding atropine
2- Immunosuppressant drugs: like prednisone, cyclosporine, and
azathioprine may be used. It is common for patients to be treated with a
combination of these drugs with a cholinesterase I
(b)Plasmapheresis and IVIG
In case of emergency (myasthenic crisis), plasmapheresis can be used to
remove the putative antibody from the circulation. Also, IV
immunoglobulins (IVIG) can be used to bind the circulating antibodies.
(c)Thymectomy :
It
is the surgical removal of the thymus
10/17/2015
Dr. Naglaa F.gland
El-Orabi to treat MG.