Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
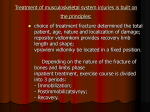
Injuries Signs and Symptoms Pain Swelling Heat Redness Loss of function Depends on severity of injury Treatment R.I.C.E. and possible NSAIDs Range of Motion (Stretching!) Strength and Endurance Neuromuscular Control & Balance Functional and Sports Specific Progressions Maintain Cardio Fitness All depend on severity. Begin rehab as soon as possible. What are the two categories of acute muscle injuries? Contusions Strains How does one receive a contusion? Sudden traumatic blow to the body a. b. c. d. What is typical in cases of severe contusions? the athlete reports being struck by a hard blow the blow causes pain and a transitory paralysis caused by pressure on and shock to the motor and sensory nerves palpation often reveals a hard area, indurated because of internal hemorrhage ecchymosis, or tissue discoloration, may take place What is a strain? A stretch, tear, or rip in the muscle or adjacent tissue such as the fascia or muscle tendon How are strains most often produced? Abnormal muscular contraction What is the cause of abnormal muscular contraction? It is fault in the reciprocal coordination of the agonist and antagonist muscles take place. The cause of this fault or un-coordination is a mystery. However, possible explanations are that it may be related to: a mineral imbalance caused by profuse sweating to fatigue metabolites collected in the muscle itself to a strength imbalance between agonist and antagonist muscles. What is a grade 1 (or 1st degree or 1°) strain? Slight over-stretching to mild tearing (20%) of the muscle fibers. It is accompanied by local pain, which is increased by tension in the muscle, and a minor loss of strength. There is mild swelling, ecchymosis, and local tenderness. What is a grade 2 (or 2nd degree or 2°) strain? Moderate tearing (20% - 70%) of the muscle fibers. It is similar to a grade 1, but has moderate signs and symptoms (moderate loss of strength, moderate swelling, ecchymosis, and local tenderness). What is a grade 3 (or 3rd degree or 3°) strain? Has signs and symptoms that are severe (severe swelling, ecchymosis, and local tenderness) with a loss of muscle function and, commonly, a palpable defect in the muscle. What does a tendon attach? Muscle to bone What does a ligament attach? Bone to bone What is a cramp? A painful involuntary contraction of a skeletal muscle or muscle group. Cramps have been attributed to what? A lack of water or other electrolytes in relation to muscle fatigue. What is a spasm? A reflexive reaction caused by trauma of the musculoskeletal system List and define the two types of spasms or cramps: a. clonic – alternating involuntary muscular contraction and relaxation in quick succession b. tonic – rigid muscle contraction that lasts a period of time. What are the four specific indicators of possible overexertion? a. b. c. d. acute muscle soreness delayed muscle soreness muscle stiffness muscle cramping a. b. List and define the two types of muscle soreness: Acute-onset muscle soreness – which accompanies fatigue. This muscle pain is transient and occurs during and immediately after exercise. Delayed-onset muscle soreness (DOMS) – becomes most intense after 24 to 48 hours and then gradually subsides so that the muscle becomes symptom-free after 3 or 4 days. (This second type of pain is described as a syndrome of delayed muscle pain leading to increased muscle tension, swelling, stiffness, and resistance to stretch). What are the possible causes for delayed-onset muscle soreness? It may occur from very small tears in the muscle tissue, which seems to be more likely with eccentric or isometric contractions. It may also occur because of disruption of the connective tissue that hold muscle tendon fibers together. What is muscle stiffness? Muscle stiffness does not produce pain. It occurs when a group of muscles have been worked for a long period of time. The fluids that collect in the muscles during and after exercise are absorbed into the bloodstream at a slow rate. As a result, the muscle becomes swollen, shorter, and thicker and therefore resists stretch. What can be done to assist in reducing muscle stiffness? Light exercise Massage Passive mobilization What is muscle guarding? Following injury, the muscle that surrounds the injured area contract, in effect, splint that area, thus minimizing pain by limiting movement. (Quite often this splinting is incorrectly referred to as a muscle spasm) The suffix “itis” means inflammation: Myositis/Fasciitis - inflammation of the muscle tissue Tendinitis – inflammation of a tendon Tenosynovitis - Inflammation of the synovial sheath surrounding a tendon Bursitis – inflammation of the bursa Periostitis – inflammation of the bone covering What are the major acute injuries that happen to synovial joints? Sprains Subluxations Dislocations What is a sprain? Stretching or total tearing of the stabilizing connective tissues (ligaments) What is a grade 1 (or 1st degree or 1°) sprain? Slight over-stretching to mild tearing (20%) of the ligament. It is characterized by some pain, minimum loss of function, mild point tenderness, little or no swelling, and no abnormal motion when tested. What is a grade 2 (or 2nd degree or 2°) sprain? Moderate tearing (20% - 70%) of the ligament. There is pain, moderate loss of function, swelling, and in some cases slight to moderate instability. What is a grade 3 (or 3rd degree or 3°) sprain? It is extremely painful, with major loss of function, severe instability, tenderness, and swelling. What is a subluxation? Partial dislocations in which an incomplete separation between two articulating bones occurs. What is a dislocation (luxation)? Total disunion of bone apposition between articulating surfaces What are several factors that are important in recognizing and evaluating dislocations? Loss of limb function Deformity Swelling Point tenderness What is an acute bone fracture? A partial or complete interruption in a bone’s continuity What is a stress fracture? Rhythmic muscle action performed over a period of time at a sub-threshold level causes the stress-bearing capacity of a bone to be exceeded What are the typical causes of stress fractures in sports? Coming back into competition too soon after an injury or illness Going from one event to another without proper training in the second event Starting initial training too quickly Changing habits or the environment Strains Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Groin Strain (Hip) Running, Jumping, Twisting (ER) Typical Typical, May need crutches, compression wrap during activity Quadriceps Strain (Thigh) Sudden stretch from knee flexion Typical Typical, May need crutches, compression wrap during activity Hamstring Strain (Thigh) Sudden stretch from knee extension Typical Typical, May need crutches, compression wrap during activity Gastrocnemius Strain (Leg) Quick starts & stops, jumping, sudden knee extension. Typical Typical, heel wedge, compression wrap during activity Achilles Tendon Strain (Ankle) Usually after ankle sprains or sudden excessive ankle dorsiflexion. Typical Typical, heel lift, compression wrap during activity Achilles Tendon Rupture (Ankle) Sudden pushing-off action of the forefoot with the knee being forced into complete extension. Typical, hears a pop, indentation at site, positive Thompson’s Test RICE, X-ray to rule out fracture, possible surgical repair, immobilization for 4 to 6 weeks, begin rehab. Heel lifts in both shoes Longitudinal Arch Strain Repetitive contact with a hard playing surface. It may appear suddenly or slowly over time. Typical Typical, Reduce weight bearing activity, possible arch support taping Metatarsal Arch Strain Excessive pronation and weak intertarsal ligaments will allow the foot to abnormally spread resulting in a fallen arch Typical Typical, orthotic or pad to elevate the fallen arch. Patellar Tendon Rupture Sudden powerful contraction of the quadriceps Typical, Defect can be palpated, athlete cannot extend the knee, swelling, initial significant pain followed by a feeling that the injury is not serious Typical, surgery Strains Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Elbow strain Excessive resistive motion, repeated microtears Typical Typical Lumbar strain Sudden extension on an overloaded, unprepared, or underdeveloped spine, usually in combination with trunk rotation; chronic strain, commonly associated with faulty posture that involves excessive lumbar lordosis. Typical Typical Neck and Upper Back strain Turn the head suddenly or forced flexion, extension, or rotation Typical, muscle guarding and reluctance to move the neck in any direction Typical, possible soft cervical collar Cervical sprain (Whiplash) Turn the head suddenly or forced flexion, extension, or rotation, but much more violently than the cervical strain Typical, muscle guarding and reluctance to move the neck in any direction; this pain may persist much longer than that of the cervical strain. Typical, X-rays to rule out fracture. and possible soft cervical Sprains Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Hip Sprain Sudden stretch from knee flexion Typical Typical, May need crutches MCL Sprain (Knee) Direct blow (valgus force), severe outward twist Typical, positive valgus stress test Typical, May need crutches LCL Sprain (Knee) Direct blow (varus force) Typical, positive varus stress test Typical, May need crutches ACL Sprain (Knee) Direct blow, rotation, hyperextension Typical, positive anterior drawer test, positive Lachman’s test Typical, crutches, immobilization, physician referral, possible surgery PCL Sprain (Knee) Direct blow, knee flexion, landing on a flexed knee Typical, positive posterior drawer test Typical, crutches, immobilization, physician referral, possible surgery Inversion (Lateral) Ankle Sprain Foot inversion, plantar flexion, adduction Typical, positive anterior drawer test, positive Talar tilt test Typical, possible crutches, possible immobilization, possible physician referral, possible surgery Eversion (Medial) Ankle Sprain Foot pronation, hypermobility, depressed medial longitudinal arch Typical, positive anterior drawer test, positive Talar tilt test Typical, possible crutches, possible immobilization, possible physician referral, possible surgery Syndesmotic (High) Ankle Sprain External rotation, forced dorsiflexion Typical Typical, may take months to heal Sprained Toes or Turf Toe Force against an unyielding object Typical, Valgus & Varus Stress Tests, Anterior & Posterior Drawer Tests Typical, tape Acromioclavicular (AC) Sprain Direct Impact Typical Typical, immobilization, possible physician referral Sprains Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Elbow sprain Hyperextension or valgus forces Typical Typical Wrist sprain Fall on hyperextended wrist; any abnormal, forced movement of the wrist Typical Typical Finger sprain Fall on hyperextended wrist; any abnormal, forced movement of the wrist Typical Typical Finger fractures Direct trauma or violent twisting Typical Typical Lumbar sprain Forward bending and twists while lifting or moving some object Typical Typical Sacroiliac sprain Twisting with both feet on the ground, stumble forward, fall backward, step too far down and lands heavily on one leg, or bends forward with the knees locked while lifting Typical, associated muscle guarding. Possible asymmetry with the ASIS and/or PSIS, difficulty with forward bending, straight leg raising increases pain after 45º, as well as side bending toward the painful side. Typical, Bracing may be helpful. Joint should be mobilized to correct existing asymmetry Bursitis Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Trochanteric Bursitis Repetitive Typical, pain may radiate to the knee causing a limp Typical, May need crutches, NSAIDs and analgesics. Patellar Bursitis Continual kneeling, overuse Typical, ballotable Typical, eliminate the cause, NSAIDs Shoulder bursitis Overuse Typical, positive impingement test Typical Olecranon Bursitis Direct force, overuse Typical Typical Dislocations and Subluxations Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Shoulder dislocation/subluxation Forced abduction, external rotation, direct blow Typical, possible deformity, unable to touch opposing shoulder (Apley’s scratch test Typical, Immediate immobilization, RICE, pillow under the arm for comfort, physician referral, x-rays to rule out a fracture Elbow dislocation Fall on the outstretched hand with the elbow in a position hyperextension; or a severe twist while it is in a flexed position. Typical, Rupturing or tearing most of the stabilizing ligaments, profuse hemorrhage and swelling. Severe pain and disability, possible radial head fracture. Typical, sling, physician referral Lunate Dislocation Forced hyperextension Typical, difficulty in executing wrist and finger flexion. There may be numbness or even paralysis of the flexor muscles because of lunate pressure on the median nerve Typical, possible physician referral Finger dislocations/subluxations Direct trauma or violent twisting Typical Typical Lumbar Vertebrae Dislocation Compression fracture may occur as a result of hyperflexion of the trunk; falling from a height and landing on the feet or buttocks; direct impact from a sudden blow Typical Typical, X-ray, physician referral, put athlete on a spine board Cervical dislocation Violent flexion and rotation of the head Point tenderness, restricted movement, cervical spasm, cervical pain and pain in the chest and extremities, numbness in the trunk and/or limbs, weakness or paralysis in the trunk and/or limbs, loss of bladder and/or bowel control C-spine, Physician referral Contusions Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Hip Contusion (Hip Pointer) Direct blow Typical, spasms, transistory paralysis, unable to rotate the trunk or to flex the thigh without pain Typical, physician referral to r/o fracture, 1 to 2 days bed rest, ice massage, ultrasound, NSAIDs Quadriceps Contusion Direct blow Typical, transitory loss of function Typical, RICE with the knee in flexion, NSAIDs Joint Contusion Direct blow Typical Typical, possible physician referral, return to activity with protective padding when initial pain and irritation subsides. Shin contusion Blow to the anterior aspect of the lower leg. Typical, rapid hematoma formation, can be associated with compartment syndrome or fracture. Typical, NSAIDs and analgesics, maintaining compression is critical (may have to aspirate hematome), ROM exercises and PRE within pain limits, doughnut padding and orthoplast shell for protection. Calcaneal Contusion Occurs by impact from running or jumping Typical Typical, moderate activity with the protection of a heel cup or doughnut may resume if pain when walking has subsided by the 3rd day, shock absorbent footwear shoe be worn. Finger contusions Direct trauma Typical Typical Rib contusion Direct blow Typical, Sharp pain during breathing, point tenderness, pain when the rib cage is compressed Typical, possible bed rest and cessation of sports activities Fractures Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Femoral Stress Fractures Repetitive Typical, Groin pain along with an aching sensation in the thigh that increases with activity and decreases with rest. Standing on one leg may be impossible Typical, Rest, for 2 to 5 months, xrays and possible bone scan, swimming Acute Femoral Fracture Direct Trauma Typical, pain over the fracture site, deformity Ice, Treat for shock, verify neurovascular status, splint, physician referral Patellar Fracture Direct or indirect trauma Typical, Hemorrhage and joint effusion Typical, physician referral Acute Leg Fracture Direct traumatic blow Typical, Soft tissue insult and hemorrhaging, intense pain and disability, leg appears hard and swollen. Splint and ice, refer to a physician Tibia or Fibular Stress Fracture Repetitive or Overuse Typical, positive percussion or compression test, positive x-ray or bone scan Typical, NSAIDs, no activity for at least 14 days, possible cast and/or crutches, weight bearing when pain subsides, correct biomechanics, running may resume when the athlete is completely pain free. Ankle Fracture (misnomer) Forced abduction or planting in combination with forced internal rotation, trauma. Typical, possible deformity Typical, x-ray examination, a walking cast or brace may be applied once swelling is reduced, for 6 to 8 weeks, PNF exercises, isometrics (during immobilization), PRE, and balance activites up to 4 weeks. Fractures (cont.) Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Talus Fracture Occurs either laterally from a severe inversion and dorsiflexion force or medially from an inversion and plantar flexion force with external rotation of the tibia on the talus. Typical, History of repeated trauma to the ankle, feels pain on weight bearing, complaint of snapping or catching, intermittent swelling, anteromedial or anterolateral joint line of the talar dome is tender when palpated. Typical, X-ray is essential for an accurate diagnosis, non-surgical management for a non-displaced sub-chondral compression fracture, protective immobilization, non-weight bearing progression to full weight bearing depending on symptoms, if conservative treatment fails surgery may be required, expect to resume activity 6 to 8 months after surgery. Calcaneal Fracture Occurs most often after a jump or fall from a height. An avulsion fracture can also occur with this injury Typical, inability to bear weight Typical, X-ray is essential for an accurate diagnosis, non-surgical management for a non-displaced fracture, protective immobilization, non-weight bearing progression to full weight bearing depending on symptoms, Calcaneal Stress Fracture Occurs from repetitive impact during heel strike and characterized by a sudden onset of constant pain in the plantar-calcaneal area. Typical, Feels pain on weight bearing, pain tends to continue after exercise stops, bone scan may be required. Typical, Conservative management for the first 2 to 3 weeks, rest, active ROM exercises of the foot and ankle, non-weight bearing cardiovascular exercises, may resume activities within pain limits when pain subsides, must wear a cushioned shoe. Jone’s Fracture Inversion and plantar flexion of the foot, direct forces, or repetitive stress. Typical, Immediate swelling and pain over the 5th metatarsal, high nonunion rate, coarse of healing is unpredictable. Typical, Crutches with no immobilization, gradually progress to full weight bearing as pain subsides, return to activity is possible in 6 weeks, non-union may cause refracture to occur. Fractures (cont.) Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Metatarsal Stress Fracture (March Fracture) Most commonly involves the shaft of the 2nd metatarsal (March fracture). Occurs in the runner suddenly changing training patterns, such as increasing mileage, running hills, or running on a harder surface. An atypical condition such as a structural forefoot varus, hallux valgus, or a short 1st metatarsal will predispose to a 2nd metatarsal stress fracture. A stress fracture of the 5th metatarsal at the insertion of the peroneous brevis tendon can occur, but should not be confused with a Jones fracture. Typical Typical, Bone scan is the best way to detect this injury, 3 or 4 days of partial weight bearing after two weeks of rest, return to running should be gradual, orthotics can help to reduce stress Phalanges Occurs by either kicking an object, stubbing a toe, or being stepped on. Dislocations are less common than fractures. Typical, deformity. Stiffness and residual pain may last for several days Typical, buddy tape, possible physician referral Clavicular Fracture Fall on the outstretched, a fall on the tip of the shoulder, or direct impact. Typical, Clavicle appears slightly lower than the opposite side. possible deformity Typical, Sling and swathe, treat for shock, X-ray, immobilization for 6 to 8 weeks. After immobilization, begin gentle isometrics and mobilization exercises. May require surgery. Scapular Fracture Direct impact or force transmitted through the humerus to the scapula. Typical, Pain during shoulder movement Typical, Sling, x-ray, begin overhead strengthen in 1 week. Fracture of the Humerus Direct blow or fall on the outstretched arm Typical, inability to move arm Typical, Sling and swathe, treat for shock, physician referral, immobilization for 6 to 8 weeks Fractures (cont.) Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Forearm fracture Direct trauma or fall on the outstretched arm Typical, Audible pop or crack Typical, sling, physician referral Colle’s Fracture Fall on an outstretched armforcing the radius and ulna into hyperextension, or falling on the backward hand Typical, Possible silver fork deformity, and possible median nerve damage Typical, sling, physician referral Scaphoid (Navicular) Fracture Force on the outstretched arm Typical Typical, splint, physician referral Hamate fracture Fall or from contact from a sports implement Typical Typical, splint, physician referral Lumbar Vertebrae Fracture Compression fracture may occur as a result of hyperflexion of the trunk; falling from a height and landing on the feet or buttocks; direct impact from a sudden blow Typical Typical, X-ray, physician referral, put athlete on a spine board Cervical fracture Axial loading; sudden forced hyperextension Point tenderness, restricted movement, cervical spasm, cervical pain and pain in the chest and extremities, numbness in the trunk and/or limbs, weakness or paralysis in the trunk and/or limbs, loss of bladder and/or bowel control C-spine, Physician referral Rib Fracture Direct or indirect trauma, violent muscular contractions Typical, Sharp pain during inspiration, possible crepitus during palpation Typical, physician referral, rest and immobilization Tendinitis Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Osgood-Schlatter repetitive stress at the tibial tuberosity Typical, hemorrhage, gradual degeneration, severe pain when kneeling, running, or jumping, point tenderness Typical, reduce irritating activities, cast may be required, isometric strengthening for quads and hamstrings Larsen Johansson repetitive stress at the inferior patellar pole Typical, hemorrhage, gradual degeneration, severe pain when kneeling, running, or jumping, point tenderness Typical, reduce irritating activities, cast may be required, isometric strengthening for quads and hamstrings Patellar Tendinitis (Jumper’s or Kicker’s Knee) Repetitive running, jumping, and kicking Typical, Pain and tenderness at the posterior, inferior patellar pole Typical, thermal agents, ultrasound, brace (counter-force) massage Runner’s (Cyclist’s) Knee Repetitive, overuse Typical, Malalignment and structural asymmetries of the foot and lower leg. Contributes to iliotibial band friction syndrome and pes anserinus tendonitis or bursitis Typical, Correction of foot and leg alignment problems, RICE, proper warm-up and stretching, avoidance of aggravating activities, NSAIDs. Achilles Tendinitis Excessive tensile stresses placed on it during repetitive movements and presents with a gradual onset. Typical, uphill running and hill workouts aggravate the condition, weak gastrocnemius-soleus complex, morning stiffness, discomfort walking after prolonged sitting, tendon is warm and painful upon palpation, palpable crepitus with active plantar and dorsiflexion, pain on passive stretching, chronic inflammation. Typical, may be resistant to quick resolution, address structural faults (i.e. footwear, orthotics, etc.) ultrasound to increase blood flow, friction massage may be helpful, strengthening of the gastrocnemiussoleus unit. May be resistant to quick resolution, address structural faults (i.e. footwear, orthotics, etc.) RICE, ultrasound to increase blood flow, friction massage may be helpful, strengthening of the gastrocnemiussoleus unit. Tendinitis (cont.) Injury Mechanism of Injury (Etiology) Signs & Symptoms Treatment Anterior Tibialis Tendinitis Common when running downhill for extended periods of time. Typical Typical, avoid hills Posterior Tibialis Tendinitis Overuse injury among runners with hypermobility or pronated feet Typical, Swelling of the medial malleolus area, edema and point tenderness behind the medial malleolus area, pain can become more intense during resistive inversion and plantar flexion Typical, non-weight bearing short-leg cast with the foot in inversion may be used, Low Dye taping or orthotic can be used to correct pronation. Peroneal Tendinitis Problem in athletes with pes cavus where the foot tends to excessive supinate. Typical, Pain of the lateral malleolus area when rising on the ball of the foot, tenderness behind the lateral aspect of the calcaneous distally beneath the cuboid. Typical, tape with elastic tape, appropriate warm-up and flexibility exercises, Low Dye taping or orthotic can be used to prevent excessive supination. Wrist tendinitis Repetitive pulling movements Typical Typical Chondramalacia (Patellofemoral Arthralgia) Etiology: Abnormal patellar tracking Signs & Symptoms: Pain in the anterior aspect while running, walking, ascending stairs, and squatting. Recurrent swelling, grating sensation during flexion and extension, patellar grind test produces crepitus. Treatment: Avoid irritating activities, pain-free isometric exercise to strengthen the quads, anti-inflammatories, orthotics to correct pronation and reduce tibial torsion, possible surgery. Patellofemoral Stress Syndrome (PFSS) (Patellofemoral Arthralgia) Etiology: Hamstrings, gastrocnemius, IT band, or lateral retinaculum tightness; increased Q angle, foot pronation, patella alta, VMO insufficiencies Signs & Symptoms: Tenderness over the patellar lateral facet, swelling, dull ache in the center of the knee, patellar compression will elicit pain and crepitis, positive apprehension test Treatment: Strengthen VMO; stretching for hamstrings, gastrocnemius, and IT band; orthotics and/or taping to correct alignment Cramps and Spasms Etiology: Excessive loss of fluids through sweating, inadequate muscle coordination. Signs & Symptoms: Pain, tonic contraction. Treatment: Athlete should relax, gradual stretching, ice or gentle ice massage. Medial Tibial Stress Syndrome Etiology: Repetitive microtrauma, weak leg muscles, inadequate footwear, inappropriate training, malalignment problems. Signs & Symptoms: Grade 1: pain after activity Grade 2: pain before and after activity, but does not affect performance Grade 3: pain before, during, and after activity, affects performance Grade 4: constant pain that makes performance impossible Pain is along the lower medial anterior tibialis. Treatment: Physicians referral to rule out other problems, RICE, NSAIDs and analgesics, ice massage, modify activity, correct biomechanics, orthotics and/or arch taping. Lateral Epicondylitis (Tennis Elbow) Etiology: Repetitive microtrauma, hyperextension activities Signs & Symptoms: Aching pain over the region during and after exercise, pain worsens with continued activity, weakness in the hand and wrist Treatment: RICE, NSAIDs and analgesics, immobilization, strengthening and stretching exercises, correct biomechanics, counterforce brace Medial Epicondylitis (Pitcher’s Elbow, Racquetball Elbow, Golfer’s Elbow, Javelin-Thrower’s Elbow) Etiology: Repeated forceful extension of the wrist and valgus torques of the elbow. Signs & Symptoms: Pain, possible radiating pain, point tenderness, mild swelling, AROM produces pain. Treatment: RICE, NSAIDs and analgesics, immobilization (sling), strengthening and stretching exercises, correct biomechanics, counterforce brace. For severe cases, splint and complete rest for seven to 10 days. Carpal Tunnel Syndrome Etiology: Repetitive wrist flexion, direct trauma Signs & Symptoms: Sensory or motor deficits; tingling, numbness, and paresthesia over the thumb, index and middle fingers, and palm of the hand; muscular weakness Treatment: RICE, immobilization, and NSAIDs. Surgical decompression may be necessary de Quervain’s Disease (Hoffman’s Disease) Etiology: Constant wrist movement Signs & Symptoms: Aching pain which may radiate into the hand or forearm, positive Finklestein’s test; point tenderness and weakness during thumb extension and abduction; there may be a painful snapping and catching of the tendons Treatment: Immobilization, rest cryotherapy, NSAIDs, ultrasound, ice massage Wrist Ganglion Etiology: Appears slowly after a wrist sprain Signs & Symptoms: Occasional pain with a lump at the site. Pain increases with use Treatment: RICE, pressure with a felt pad, ultrasound, possible surgical removal Sciatica Etiology: Torsion or direct blow to the back causing inflammation or compression of the sciatic nerve Signs & Symptoms: Pain may be abrupt or gradual, produces a sharp shooting pain that follows the nerve pathway along the posterior and medial thigh; there may be tingling and numbness along its path; nerve may be extremely sensitive to palpation; straight leg raises intensifies pain. Treatment: Rest is essential. Stretching of a tight piriformis muscle may decrease symptoms; NSAIDs and RICE, surgery may be necessary. Brachial Plexus Neurapraxia (Burner or Stinger) Etiology: Stretching or compression of the brachial plexus Signs & Symptoms: Burning sensation, numbness, tingling, and pain extending from the shoulder down to the hand with some loss of function of the arm and hand that lasts for several minutes. Treatment: RICE; strengthening exercises; Athlete may return to full activity once symptoms have completed resolve and there are no associated neurological symptoms.