Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
ANTICOAGULANT
BY :DR ISRAA OMAR
Definition of Anticoagulation
• Therapeutic interference with the clotting
mechanism of the blood ("blood-thinning") to
prevent or treat thrombosis and embolism.
Indications of Anticoagulant Therapy
• Treatment and Prevention of Deep Venous
Thrombosis
• Pulmonary Emboli
• Prevention of stroke in patients with atrial
fibrillation, artificial heart valves, cardiac thrombus.
• During procedures such as cardiac catheterisation
Enhances
Antithrombin Activity
Standard Heparin
•
•
•
•
Heterogeneous mixture of polysaccharide chains
MW 3k Da to 30k Da
Active in vitro and in vivo
Administration - parenteral- Do not inject IM - only IV
or deep s.c.
• Half-life 1 - 2 hrs - monitor APTT
• Adverse effect - haemorrhage
• antidote - protamine sulphate
Heparin mechanism of action
Heparin
Antithrombin III
Thrombin
Monitoring Heparin
• Activated Partial Thromboplastin Time (APTT)
• Normal range: 25-40 seconds
• Therapeutic Range: 55-70 seconds
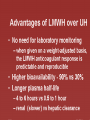
Low Molecular Weight Heparin
• Changed management of venous
thromboembolism
• Standard (Unfractionated) heparin 30k
• LMWH contains polysaccharide chains MW 5k
• Enriched with short chains with higher antiXa:IIa ratio
Differences in Mechanism of Action
• Any size of heparin chain can inhibit the action of
factor Xa by binding to antithrombin (AT)
• In contrast, in order to inactivate thrombin (IIa), the
heparin molecule must be long enough to bind both
antithrombin and thrombin
• the chains of LMWH are not long enough to bind
antithrombin and thrombin
Complications of Heparin
• Hemorrhage(can be reversed by using protamine
sulfate as an antidote)
• Heparin-induced thrombocytopenia (HIT) and
thrombosis
• Osteoporosis (long-term only)more than 6 month
;the explanation of this side effect is unknown
• Hyperkalemia
• Hypersensitivity reaction
Heparin-Induced Thrombocytopaenia
• Most significant adverse effect of heparin after
haemorrhage
• Most common drug-induced thrombocytopenia
Trreatment of HIT
• Discontinue all heparin
• If need to continue anti-coagulation, use
danaparoid (orgaran).
• Avoid platelet transfusions
• Thrombosis: use danaparoid or thrombin
inhibitor (Hirudin)
Oral anticoagulant
• Warfarin is an oral anticoagulant that prevent
thrombosis
• It inhibit the enzymatic reduction of vitamin K
(vitamin K epoxide reductase)to its
hydroquinone form, interfering with the post
transtional modification (carboxylation) of
glutamic acid residues in clotting factors 2, 9,
7, 10.
• Warfarin acts only in vivo
Vitamin K-Dependent Clotting Factors
Vitamin K
VII
IX
X
II
Synthesis of
Functional
Coagulation
Factors
Warfarin Mechanism of Action
Vitamin K
Antagonism
of
Vitamin K
VII
IX
X
II
Warfarin
Synthesis of Non
Functional
Coagulation
Factors
Warfarin
Side effects of warfarin
• Bleeding
• Hepatotoxicity
• Warfarin induced skin
necrosis (can be
reduced by starting
heparin and warfarin
concomitantly)
Warfarin: Major Adverse Effect—
Haemorrhage
• Factors that may influence bleeding risk:
– Intensity of anticoagulation
– Concomitant clinical disorders(liver disease ,thyrotoxicosis
and fever )
– Quality of management
– Concomitant use of other medications
1. Cimetidine and other enzyme inhibitors increase its action
while rifampicin and other enzyme inducers inhibit the
action of warfarin
2. aspirin increase its bleeding risk by working in synergistic
fashion(PLATELETS INHIBITION) .
3. NSAIDS and chloral hydrate displace it from binding sites
4. Antibiotic eliminate the intestinal flora that produce
vitamin k this will increase the risk of bleeding
Prothrombin Time (PT)
• Historically, a most reliable and “relied upon” clinical
test
However:
– Proliferation of thromboplastin reagents with
widely varying sensitivities to reduced levels of
vitamin K-dependent clotting factors has occurred
– Problem addressed by use of INR (International
Normalized Ratio)
Changing over from Heparin to
Warfarin
• May begin concomitantly with heparin therapy
• Heparin should be continued for a minimum of four
days
– Time to peak antithrombotic effect of warfarin is
delayed 96 hours (despite INR)
• When INR reaches desired therapeutic range,
discontinue heparin (after a minimum of four days)
Warfarin: Dosing & Monitoring
• Start low
– Initiate 5 mg daily
– Educate patient
• Stabilize
– Titrate to appropriate INR
– Monitor INR frequently (daily then weekly)
• Adjust as necessary
• Monitor INR regularly (every 1–4 weeks) and adjust
Contraindications to Warfarin Therapy
• Pregnancy (it is a erotogenic drug can cause maxillofacial
abnormality if given in the first trimester and increase
the incidence of bleeding in the new born baby in the
last trimester; but it can be given in the middle trimester
of pregnancy but with higher doses to achieve the target
INR because there is hyper-coaguability state during
pregnancy
• Situations where the risk of hemorrhage is greater than
the potential clinical benefits of therapy
– Uncontrolled alcohol/drug abuse
– Unsupervised dementia/psychosis
Signs of Warfarin Overdosage
• Any unusual bleeding:
– Blood in stools or urine
– Excessive menstrual bleeding
– Bruising
– Excessive nose bleeds/bleeding gums
– Persistent oozing from superficial injuries
– Bleeding from tumor, ulcer, or other lesion
Reversing action of warfarin
• Plasma(fresh frozen plasma or clotting factors)
– Rapid but short-lasting, used mainly for life
threating bleeding
• Vitamin K
– Not rapid, but lasts 1-2 weeks. Do not use if
wishing to restart warfarin within next week.
In some cases only stopping the drug can be enough
Thank you