Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
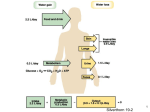
Disorders of Water Balance Polyuria-Polydipsia and Hypodipsia Wendy Blount, DVM PU-PD (PU=>PD & PD=>PU) • Diabetes – secretion of a large amount of urine • Insipid – tasteless • Mellite – pharmaceutical containing honey • Polydipsia = – >100 ml/kg/day water intake – Diabetes insipidus (DI) and primary polydipsia (PP) are particularly profound – often >200 ml/kg/day • Normal urine production – 1-2 ml/kg/hr – 12-45 ml/kg/day • Polyuria = – >50 ml/kg/day • Urine SG – Always <1.020, often < 1.012 Causes of PU/PD PU => PD 1. Renal Disease – fluid Loss 2. Problem with ADH – – not produce (central DI) Kidneys don’t respond 3. Drugs PD => PU 1. Primary Polydipsia 2. Psychogenic Polydipsia Causes of PU => PD • Osmotic diuresis – Diabetes mellitus, Renal glycosuria • Osmotic diuresis + medullary washout – Chronic renal failure, Polyuric acute renal failure – Post-obstructive diuresis, Diuretic therapy • • Lack of ADH production – central diabetes insipidus Lack of response to ADH – Primary nephrogenic diabetes insipidus – Secondary nephrogenic diabetes insipidus • Pyometra, septicemias, pyelonephritis • Hypercalcemia, liver failure, hyperadrenocorticism • Hyperaldosteronism, hypokalemia, hyperthyroidism • Hypoadrenocorticism, acromegaly, polycythemia Causes of PU => PD • Drug Therapy – – – – – – – – – – – – Anticonvulsants Glucocorticoids DOCP – deoxycorticosterone pivalate Diuretics Mannitol Thyroxine Amphotericin B Lithium Methoxyflurane Sodium bicarbonate *Sodium (treats)* Vitamin D toxicity Causes of PD => PU • Primary Polydipsia – Defect in the thirst center • Psychogenic Polydipsia – Mental illness in people – Learned behavior in response to environment in the dog – Not reported in the cat Confirming PU-PD • Have owner collect urine samples – 2-3 different times in the day – For 2-3 days – do not withhold water • All <1.012 - confirms PU-PD • All 1.012-1.020 - equivocal • All >1.020 - PU-PD ruled out • If PU-PD is not confirmed with USG despite it being the CC, consider alternative syndromes – Pollakuria, stranguria – Urinary incontinence – Dehydration and appropriate increased thirst Work-Up • Most common causes of PU-PD in the dog (5) – – – – – Chronic renal failure Diabetes mellitus Hyperadrenocorticism Liver failure Hypercalcemia • Most common causes of PU-PD in the cat (3) – Chronic renal failure – Diabetes mellitus – Hyperthyroidism Work-Up Hints on the history & physical exam • Intact female + vulvar discharge – rule out pyometra • Lymphadenopathy – rule out lymphoma (hypercalcemia) • Anal sac mass – rule out apocrine gland carcinoma (hypercalcemia) • Weight loss in the cat – rule out hyperthyroidism and diabetes • Endocrine alopecia – Hyperadrenocorticism (dog > cat) – Acromegaly (cat >> dog) – diabetes mellitus (both) Work-Up Hints in the urine • All USGs <1.005 – Post-obstructive diuresis, aggressive IV fluids – Primary polydipsia, central or nephrogenic DI – hyperadrenocorticism • All USGs 1.005 - 1.008 – many possibilities – Liver failure, early CRF and all above • USGs 1.008 – 1.015 + proteinuria – Renal disease most likely – Make sure to get a urine culture – If negative, do urine protein:creatinine • USGs 1.020’s with azotemia – Hypoadrenocorticism and pyelonephritis most likely Any USG >1.020 - diabetes insipidus is ruled out • • *USG ranges from <1.008 - >1.030* – Psychogenic polydipsia most likely Work-Up • First Tier Tests – – – – – CBC, panel, lytes HW Test for dogs, FeLV/FIV tests for cats urinalysis Urine culture (cystocentesis) TT4 for cats >5 years old. • Second Tier Tests – – – – – thoracic radiographs Abdominal US + radiographs Bile acids (pre- and post-prandial) ACTH stim Urine protein:creatinine Work-Up • Third Tier Tests – – – – Vasopressin challenge Plasma osmolality with free choice water Modified water deprivation test NEVER DO A WATER DEPRIVATION TEST BEFORE RULING OUT ACQUIRED NDI, ESPECIALLY RENAL DISEASE – Proceed with caution if *none* of the serial USG are <1.008 • Isosthenuria + PU-PD is most commonly caused by renal disease • Isosthenuria + azotemia = renal disease with few exceptions • Pyelonephritis is one of the two most common causes of PU-PD + USG in the 1.020’s Work-Up More pattern recognition • Central DI or congenital Nephrogenic DI – – – – – +Neurologic deficits Sodium high normal, as with all PU => PD USG usually <1.008 if complete DI USG can be 1.008-1.018 if partial CDI Dehydration to 3-5% within a few hours of water deprivation • Psychogenic polydipsia – – – – behavioral issues Sodium low normal Fluctuating USG 1.005 – 1.030 Prolonged time to dehydration with water deprivation Central Diabetes Insipidus (CDI) Deficiency of vasopressin from the hypothalamus Vasopressin = ADH = antidiuretic hormone = AVP = arginine vasopressin • No ADH to allow kidneys to concentrate urine • USG remains below 1.008 (often below 1.005) despite severe dehydration, if complete • USG may increase to 1.008-1.015 if partial • USG >1.020 at any time rules it out • Usually acquired rather than congenital – – – – – Idiopathic (most common) Head trauma or surgery (can be transient) Neoplasia/cysts LP inflammatory destruction Parasite migration (*deworm*) Primary Nephrogenic DI (NDI) Kidneys are unable to respond to ADH at birth • Rare disorder in dogs – Familial in the Husky • Not reported in cats • Apparent at 8-12 weeks of age • Plasma ADH normal to increased – No commercially available assay in the US Primary Polydipsia (PP) Compulsive water consumption • PP caused by a hypothalamic lesion to the thirst center has been reported in people, but not in dogs or cats • Insufficient ADH secretion in response to hypertonicity has been reported in the dog (Hypodipsic Hypernatremia – HH) • Because Psychogenic Polydipsia (PsP) is the only kind of PP reported in the dog, these terms are essentially interchangeable Primary Polydipsia (PP) Psychogenic Polydipsia (PsP) is idiopathic PP • Has not been reported in the cat • Affected dogs are usually very active dogs who do not get enough activity – attention seeking behavior • Often there are changes in the environment at the time of onset • Onset at any age, but usually puppy to young adult – Temporary psychogenic polydipsia in puppies that seems to resolve at they mature is not uncommon • USG varies widely over time – 1.005 – 1.030 • ADH response to dehydration or hypertonic saline is appropriate (increased) Secondary NDI kidneys lose ability to respond to ADH Secondary NDI = acquired NDI • Plasma ADH normal to increased Pyometra and Sepsis • Bacterial endotoxins compete with ADH for aquaporin receptors on the renal tubules Hypercalcemia • Decreased response to ADH by the kidneys Liver failure – not well understood • Impaired urea production resulting in medullary washout • Vasoactive effects – altered renal blood flow Secondary NDI Hyperadrenocorticism • • • • Glucocorticoids inhibit ADH release Increase osmotic threshold Decreased renal response to ADH Rarely, physical disruption by macroadenoma Hyperaldosteronism – poorly understood • Mineralocorticoids reduce ADH release • Decreased renal response to ADH Pyelonephritis – see renal failure and sepsis Hypokalemia • Decreased renal response to ADH • Blunting of the medullary urea gradient Secondary NDI Hypoadrenocorticism - **ACTH Stim > LDD** • Mineralocorticoid deficiency results in sodium wasting and medullary washout • See hypercalcemia • Look at USG to distinguish from renal failure Hyperthryoidism – poorly understood • Increased renal perfusion • Thyrotoxicosis results in PsP • Concurrent renal insufficiency in older cats Acromegaly • Glucosuria • renal insufficiency Polycythemia • Hyperviscosity stimulates thirst CDI and PsP History and physical exam • Weight loss is not uncommon • Water intake often exceeds 200 ml/kg/day • PU-PD often present for 1-6 months prior to seeking veterinary care • BAR, not lethargic – Unless CDI is secondary to large tumor – Inappetance, stupor – Cerebral signs – pacing, disorientation, pacing, ataxia, seizures, head pressing, getting stuck in corners • Hydration normal if water not restricted • No vomiting, regurgitation, diarrhea, coughing • Urinary incontinence not uncommon, especially when sleeping CDI and PsP Diagnostics • CBC – mild polycythemia not uncommon – Owners often withhold water to some degree out of desperation • Serum panel, electrolytes – – – – BUN may be low when free choice water BUN may be high if water withheld May have mildly low Na+ and K+ when free choice water May have high Na+ and K+ if water withheld • UA – urine osmolality often < 300 mOsm/kg – USG for PP often varies from <1.008 to >1.030 – USG for CDI and NDI usually <1.008 and always <1.020 – USG for partial CDI can be 1.008-1.018, if water withheld CDI and PsP Confirm and differentiate CDI, NDI, PP 1. Rule out acquired NDI 2. Response to DDAVP 3. Plasma osmolality with free access to water 4. Modified water deprivation test Rule out acquired NDI prior to water deprivation!! • • • • CBC, panel, lytes, UA, urine culture and sensitivity (cystocentesis > mid-stream catheter) TT4 on the cat > 5 years Urine protein:creatinine + cortisol:creatinine In addition to negative urine culture, rule out pyelonephritis with either: 1. 2. • • Abdominal US *or* Trial of antibiotics PU-PD that responds to antibiotics is strong evidence for pyelonephritis, regardless of a negative urine culture Water deprivation + renal disease = disaster Plasma Osmolality • Can identify PP • Done with free access to water • • • • • Normal dog – 280-300 pOsm Complete CDI – 285-340 pOsm - high normal to high NDI – 285-340 pOsm – high normal to high Partial CDI – 280-320 pOsm – normal to high PP – 275-305 pOsm – low to normal, rarely mildly high Response to DDAVP DDAVP = D-Desmopressin Acetate VasoPressin Tablets, injection, nasal drops uses as eye drops 1. Oral tablets or drops BID x 7 days 2. Collect urine daily on days 5-7 and test USG – Medullary washout will resolve in 1-3 days, allowing you to assess response at 5-7 days 3. Increase in USG by 50% or more, especially >1.030, indicates response to DDAVP • • • • CDI – excellent and durable response to DDAVP Acquired NDI – temporary response to DDAVP PP – mild response to DDAVP Primary NDI – no or minimal response to DDAVP, unless exceedingly high doses are used Modified Water Deprivation Test To determine if endogenous ADH is released in response to dehydration And whether kidneys respond to the ADH 3 Steps: 1. Patient Preparation 2. Phase I – water restriction until 3% weight loss – – Normal response is USG >1.030 in the dog and >1.035 in the cat Partial and complete CDI – inadequate response 3. Phase II – continue only if inadequate response – Assess response to ADH analog Modified Water Deprivation Test Patient Preparation – progressive water restriction to minimize interference of medullary washout • Decrease water intake to 100 ml/kg/day prior to the start of the test 1. 2. Allow unrestricted water intake for 3 days, and measure Decrease water intake by 10% every 1-2 days until intake of 100 ml/kg/day is reached Divide daily water intake into 6-8 aliquots and give some during the night No food for 12 hours prior to starting the test 3. 4. Abort if : • animal becomes aggressive for water • Evidence of hypertonic dehydration – Change in mentation or demeanor Modified Water Deprivation Test Phase I - determines the effect of endogenous ADH on the kidneys • Start at the beginning of the work day • Observe and evaluate patient frequently • End point is 3% weight loss or USG >1.030 or clinically dehydrated or ill – – – • • Most with CDI or primary NDI will reach the endpoint in 3-10 hours Partial CDI and PP will take 10-24 hours to reach end point Normal dogs will take 24 hours or more to reach the endpoint Leaving a DI patient unattended for several hours can result in severe complications, including death Phase I may require 24 hours or more Modified Water Deprivation Test Phase I 1. Time 0 – – – – – Confirm neurologic status normal Make sure no access to food or water Empty the bladder by walking or catheterization for dogs and indwelling catheter for cats, and weigh Save sample for urine USG and ideally osmolality Take blood for serum osmolality, BUN, Electrolytes 2. Repeat every 1-2 hours – Empty the bladder by walking or catheterization for dogs and indwelling catheter for cats, and weigh 3. Every hour – Weigh and assess for dehydration and change in mentation 4. Take blood sample for BUN and sodium if dehydration, or periodically Modified Water Deprivation Test Phase I • • Abort if BUN >30, hypernatremia, severe dehydration or changes in mentation If endpoint not reached in 10 hours – – • Refer for 24 hour testing or repeat Phase I with water withheld after midnight the night before starting Urine concentration plateaus may be seen – – – Indicates maximal renal response to water deprivation Three consecutive urine samples with the same osmolality (+ 5% USG or 30 mOsm/kg) USG is less reliable for detecting plateaus Modified Water Deprivation Test Phase II - determines the effect of exogenous ADH on the kidneys in the face of dehydration Differentiates CDI from NDI 1. Time 0 (= end point of Phase I) – – – Empty bladder, keep urine for USG/osmolality, weigh Take blood for ADH if available BUN, electrolytes, serum osmolality 2. Administer vasopressin – – aqueous vasopressin (Pitressin) 0.2-0.4U/kg IM, maximum dose 5U DDAVP injection 5 mcg SC 3. Empty bladder, keep urine and weigh – – – If Pitressin - at 30, 60 and 120 minutes post injection If DDAVP – at 2 and 4 hours post injection Run USG and ideally osmolality on urine Modified Water Deprivation Test Phase II 5. Weigh every hour and assess for dehydration and change in mentation 6. Take blood sample for BUN, sodium, plasma osmolality if dehydration, and at end 7. Offer small amounts of water (10-20 ml/kg) over the next 2 hours, to avoid water intoxication 8. Then gradually return to free choice water over several hours • • Abort if BUN >30 mg/dl, hypernatremia, severe dehydration or changes in mentation Less likely to abort in Phase II than Phase I Modified Water Deprivation Test Interpreting the Modified Water Deprivation Test Normal • USG >1.030 for dogs and >1.035 for cats in Phase I • Urine osmolality >1100 mcOsm in Phase I Complete CDI • Urine osmolality will not exceed plasma osmolality (280310 mOsm/kg) in Phase I • Urine osmolality will increase in Phase II by 50-600% Hyperadrenocorticism, Partial CDI and some PP • Urine osmolality increase above 300 mOsm/kg in Phase I • Further 10-50% increase in Phase II Modified Water Deprivation Test Interpreting the Modified Water Deprivation Test Primary (congenital) and secondary (aquired) NDI • Urine osmolality will not exceed plasma osmolality (280310 mOsm/kg) in Phase I and Phase II • Dogs with primary NDI are young and otherwise normal • Dogs with secondary NDI usually have significant concurrent disease Primary Polydipsia • Given enough time, USG will exceed 1.030 in Phase I • Could take 24 hours or longer • Phase II is rarely needed, but if carried out, will produce little change Modified Water Deprivation Test Pitfalls • Easily differentiates complete CDI from primary NDI, but may not differentiate partial CDI from PP, Cushing’s Disease or many other causes of secondary NDI • Confounding variables – Chronic polyuria results in medullary washout, which in turn reduces maximal urine concentration – Partial CDI patients can have an enhanced response to ADH early on due to up regulation of receptors Modified Water Deprivation Test The Dehydrated Patient • The most common cause of dehydration in the PU-PD patient is owner withholding water • If no neurologic signs – proceed with Phase I if BUN <30, sodium normal and USG <1.030 – Proceed with Phase II if USG >1.030 • If neurologic signs – Careful fluid therapy – see next slide – adjust patient preparation to prevent dehydration the next time around Modified Water Deprivation Test Treating the Clinically Dehydrated Patient • There are three forms of dehydration 1. Isotonic – proportional loss of water and electrolytes • GI loss a common example • Sodium usually normal • Clinical signs proportional to hypovolemia 2. Hypotonic – loss of electrolytes > water loss • Hypoadrenocorticism an example • Sodium usually low, pre-renal azotemia common • Clinical signs pronounced relative to hypovolemia 3. Hypertonic - loss of free water > electrolytes • Water deprivation + PU-PD an example • Cell dehydration > plasma hypovolemia • Severe hypernatermia with hyposthenuria • Weight loss shows dehydration prior to symptoms Modified Water Deprivation Test Treating the Clinically Dehydrated Patient • Signs of hypertonic dehydration – Neurologic signs – hypertonic brain cell shrivel • Mild – irritability, weakness, ataxia • Moderate – stupor • Severe – coma and seizures • Treatment goal - Restore hydration slowly, with minimal brain cell damage & cerebral edema Modified Water Deprivation Test Treating the Hypertonic Dehydrated Patient Correct dehydration with IV 0.9% NaCl + K+ as needed (potassium chart) over 4-6 hours – Sodium should decline no more than 1 mEq/L/hr – If neurologic signs worsen, slow rate and treat for cerebral edema with hypertonic saline or mannitol 2. Once rehydrated, correct water deficit if still hypernatremic – 0.45% NaCl + 2.5% dextrose – or half strength LRS + 2.5% dextrose 1. L=( 3. current Na+ normal Na+ - 1 ) x (0.6 x weight-kg)2 • oral route preferred, IV if PO not possible • Replace 50% in the first 24 hours • Remainder over the next 24-48 hours If hypernatremia persists after 12-24 hours • Switch to 5% dextrose IV until sodium normal Referral – MRI/CT • Consider neoplasia in the older dog with CDI – if client would consider radiation therapy • T1-weighted images 80% diagnostic for CDI in people Treatment of CDI DDAVP Intranasal drops 100 mcg/ml (2.5 ml & 5ml) • • • • $150-200 Transfer to a sterile eyedropper bottle 1 drop = 1.5-4 mcg DDAVP Start at 1-2 drops in either eye SID-BID, alternate eyes DDAVP 0.1mg and 0.2 mg tablets • • • • • • bioavailability 5-15% that of nasal drops 0.05 mg PO BID for cats and dogs < 5 kg 0.1 mg PO BID for dogs 5-20 kg 0.2 mg PO BID for dogs > 20 kg Increase to TID if not effective If TID not effective, switch to eyedrops Once symptoms are controlled, wean down to lowest effective dose Treatment of CDI DDAVP injection 4 mcg/ml (2 ml) • • • • 5-20x as potent as nasal drops in people Start at 0.2-0.25ml SC SID Increase dose & frequently as needed to control symptoms Hyponatremia a possible side effect • Onset within 2 hrs, regardless of route of administration • Duration of action 6-18 hours – Higher doses prolong duration of action • Expense is often the limiting factor • Administration in the evening can allow the family to get proper sleep Treatment of CDI Other oral treatments Chlorpropamide (oral hypoglycemic) • • • • Reduces urine output 30-70% in people with CDI Seems to be more effective for partial CDI in dogs and cats 10-40 mg/kg/day Hypoglycemia can be a side effect, managed by offering multiple small meals Thiazide diuretics – 20-40 mg/kg PO BID along with low sodium diet • CDI and *NDI* – reduces urine output by 30-50% in people • Inhibits renal sodium resorption > contracts ECF > increases salt and water absorption in the renal tubule > reduces osmotic diuresis • Occasional hypokalemia can be a side effect • Check electrolyte panel every 3 months Treatment of CDI Other oral treatments Low salt diet • May be helpful for CDI and NDI • < 1g Na/Mcal • Hill’s H/D Prognosis of CDI • Prognosis is good for if medication given daily • Eye irritation is an infrequent side effect of eye drops • Not uncommon for CDI to be part of a polyendocrine syndrome – Look especially for hyperadrenocorticism if PU-PD recurs • Progressive neurologic signs may indicate a macrodenoma that carries a grave prognosis without surgery or radiation therapy – CDI persists even if tumor shrinkage is achieved, because PU-PD develops when 90% of magnocellular neurons are gone – Chemo with BCNU can be tried, but has variable outcome Prognosis of NDI • Extremely high doses of injectable DDAVP (0.33 U/kg IM TID) can sometimes control primary NDI • But therapy is very, very expensive • Thiazide diuretics are sometimes the only viable option for treatment • Long term prognosis generally poor Prognosis of Untreated DI • Dogs with CDI and NDI can do fine if they have unlimited access to water, and live in and environment where multiple urinations per hour are not a problem • In most cases, untreated animals are outdoor animals • Many discontinue treatment after a few months due to expense • Some will administer medications periodically when needed, or only at night time. • Lack of access to water of illness that causes adipsia or vomiting can be life threatening within hours – guarded prognosis • Large water receptacles are needed • Mean survival about 2 years Treatment of PsP Water Restriction • Measure free choice water intake • Gradually restrict water intake by 10% per week until 60-80 ml/kg/day is reached • Divide into several aliquots and give the last at bedtime • Rapid water restriction can result in anxiety and/or dehydration • NaCl 1 g/30kg BID or NaHCO3 0.6g/30kg PO BID x 3-5 days to help resolve medullary washout, if needed Treatment of PsP Behavior Modification • Daily exercise • Con-specific play, if the patient likes it • Environmental enrichment with interactive toys • Increased contact with people during the day Prognosis PsP – generally excellent, though relapse can occur SIADH Syndrome of Inappropriate ADH • Sustained release of ADH Etiology • Functional neoplasia – CNS or paraneoplastic – Especially bronchogenic adenocracinomas • CNS disease - Head trauma, demyelinating disease, infection/inflammation • Porphyria • Endocrine disease – hypoadrenocorticism, pituitary dwarf, profound hypothyroidism • Pulmonary disease – acute respiratory failure, aspergillosis, pneumonia, tuberculosis • Drugs SIADH Drugs that cause SIADH • ACE inhibitors • Chlorpropamide • Cyclophosphamide, vincristine • Omeprazole • SSRIs • Thiazides SIADH Clinical Presentation – water intoxication • Hyponatremia <130 for 48 hours or longer – Lethargy, weakness, muscle fasciculation – anorexia, vomiting – Obtundation, disorientation, seizures, coma (Na <120) • Plasma osmolality < 275 pOsm • Urine osmolality inappopriately high Diagnosis • Hyponatremia with plasma osmolality >275 pOsm • Inappropriately high urine osmolality • Normal renal and adrenal function • No hypovolemia • Correction by water restriction • Plasma ADH normal to high SIADH Treatment of the hypotonic dehydrated patient 1. Increase sodium to 125 mEq/L – IV 0.9% NaCl or hypertonic (3-5%) saline, start at 0.5-1 ml/lb/hr – Increase Na+ no more than 0.5-1.0 mEq/L per hour 2. When sodium >125mEq/L, Further correction by water restriction – – – – Identify the daily water intake that maintains sodium at low end of normal range Divide into 6-8 aliquots per day Never allow free access to water Can’t go swimming or have access to ponds or swimming pools or rain • Discontinue any drugs that may be causing SIADH • Some have tried tolvaptan 3 mg/kg PO BID (ADH receptor antagonist) Hypodipsic Hypernatremia • Neurologic disorder causing decreased thirst and diminished ADH release in response to hyperosmolality • HH = chronic hypernatremia & hyperosmolality due to decreased water intake, and even when euvolemic due to abnormal ADH secretion • Normal kidney function, but inappropriately dilute urine for the hypernatremia • Most common in Miniature Schnauzers • Causes in dogs: – – – – Neoplasia hydrocephalus and other degenerative CNS diseases congenital hypothalamic dysplasia inflammatory CNS disease Hypodipsic Hypernatremia Treatment: • If possible, treat underlying disease • Treat hypernatremia per previous instructions for hypertonic dehydration • Increase water intake – Add water/broth to food – Offer flavored broths multiple times daily – SC fluids at home • Some dogs do well only with increased water intake after correction of hypernatremia, and some are still hypernatremic with euvolemia – Chlorpropamide (33 mg/kg/day) has been tried with inconsistent results