Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
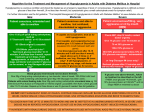
Hypoglycaemia Management of the Adult Inpatient with Diabetes Version 2 Name of responsible (ratifying) committee Formulary and Medicines Committee Nursing Midwifery Advisory Committee Resuscitation Team Date ratified 19th September 2014 Document Manager (job title) Diabetes Specialist Nurse Date issued 13th October 2014 Review date 12th October 2016 Electronic location Clinical Guidelines Related Procedural Documents Key Words (to aid with searching) Hypoglycaemia, Diabetes Version Tracking Version Date Ratified Brief Summary of Changes 2 Sept 2014 Change from using glucose 50% to glucose 20% Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 1 of 15 Author CONTENTS QUICK REFERENCE GUIDE....................................................................................................... 3 1. INTRODUCTION.......................................................................................................................... 4 2. PURPOSE ................................................................................................................................... 4 3. SCOPE ........................................................................................................................................ 4 4. DEFINITIONS .............................................................................................................................. 4 5. DUTIES AND RESPONSIBILITIES .............................................................................................. 6 6. PROCESS ................................................................................................................................... 7 7. TRAINING REQUIREMENTS ...................................................................................................... 8 8. REFERENCES AND ASSOCIATED DOCUMENTATION ............................................................ 8 9. EQUALITY IMPACT STATEMENT .............................................................................................. 8 10. MONITORING COMPLIANCE WITH PROCEDURAL DOCUMENTS ........................................ 10 Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 2 of 15 QUICK REFERENCE GUIDE This policy must be followed in full when developing or reviewing and amending Trust procedural documents. For quick reference the guide below is a summary of actions required. This does not negate the need for the document author and others involved in the process to be aware of and follow the detail of this policy. To minimise risk of hypoglycaemia: On recognition of a hypo: Patients should be assessed on admission as to: Their usual hypo signs How often and when they suffer from hypos Their usual treatment of hypos Ensure that the patient: knows the routine of the ward regarding meals and snacks Has a supply of snacks close to hand Receives their diabetic medication at the appropriate times in relation to meals MILD Alert, conscious and able to swallow MODERATE Drowsy, uncooperative and/or risk of choking Test capillary glucose if possible and initiate treatment immediately using HYPOBOX Hypoglycaemia Kit to prevent further harm to the patient. If patient is asymptomatic repeat test. SEVERE Call 2222 and Fast Blp Doctor Unconscious and potential for no gag reflex, and/or fitting, and/or NBM STEP ONE Initially administer 1x25g Glucose 40% oral gel from the hypoglycaemia kit allowing it to be swallowed STEP TWO Repeat at 5-15 min intervals as necessary depending on patient symptoms and glucose concentrations. If Glucogel unavailable use 10-20g fast acting glucose such as 2 tsp sugar in water or 200ml glass of fizzy drink or patients own remedy if appropriate If patient deteriorates move to yellow or red guidance 1. STEP THREE To prevent glucose levels falling again ensure long-acting carbohydrates such as adequate amounts of bread/potato/rice is eaten with a meal or a snack such as 2-3 biscuits, fruit, current bun is eaten if it is not a meal time. Continue regular monitoring for 24 – 48 hours and reflect on cause of hypo event STEP ONE STEP ONE Initially administer ONE or TWO tube(s) 25g Glucose 40% oral gel from the hypoglycaemia kit, inside the cheek. Massage outside of cheek allowing it to be absorbed. Check ABC Place in recovery if required Administer intramuscular injection (lateral arm or thigh) of Glucagon using GlucaGen HypoKit 1mg stored in locked ward fridge Do not leave patient STEP TWO Repeat using one tube at 5-15 min intervals as necessary depending on patient symptoms and glucose concentrations. If patient deteriorates move to red guidance STEP THREE Follow as per green step three NB: Glucagon has little effect in chronically malnourished / alcoholics / prolonged starvation / severe liver disease / renal failure If no reponse from Glucagon within 5-10 minutes, doctor to administer IV injection of 50mls of 20% glucose, administered slowly through a large vein and large gauge cannula. The remaining 50mls may be given after 10mins if blood glucose less than 4mmol/L. STEP TWO Once conscious, follow yellow step one and two STEP THREE Follow as per green step three INSULIN SHOULD NOT BE OMITTED FOLLOWING AN EPISODE OF HYPOGLYCAEMIA. If you are concerned, patients should be assessed for a smaller insulin dose rather than an omission. BGLs will be erratic following a hypoglycaemic event and patients can feel quite unwell for up to 48 hours. Refer to Diabetes Specialist Team if concerned Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 3 of 15 INTRODUCTION All people with diabetes who are administering oral anti-diabetic medications or insulin therapy have the potential to suffer from hypoglycaemic events. When combined with altered routines while an inpatient, this risk increases. Hypoglycaemic events are usually easily treated if appropriate measures are taken. If incorrect treatment is provided, or treatment is delayed, serious harm can ensue. 2. PURPOSE This guideline has been developed to assist staff in the appropriate management decisions regarding treating a person having a hypoglycaemic event. Staff will understand how to recognise a hypoglycaemic event, what the appropriate treatment options are, and subsequent monitoring of recovery to ensure patient safety and comfort. Staff will also be able to acknowledge groups of patients who standard hypoglycaemia treatment may be less effective. This guideline will assist PHT registered and unregistered nurses and medical staff. 3. SCOPE This guideline will apply to adult inpatients who have Type 1 or Type 2 diabetes requiring treatment secondary to a confirmed hypoglycaemic event; capillary blood glucose reading of approximately 4mmols/l or less, or as a result of professional judgment prior to testing and confirming blood glucose level (1) ‘In the event of an infection outbreak, flu pandemic or major incident, the Trust recognises that it may not be possible to adhere to all aspects of this document. In such circumstances, staff should take advice from their manager and all possible action must be taken to maintain ongoing patient and staff safety’ 4. DEFINITIONS Diabetes Type 1 diabetes is an autoimmune disease characterised by hyperglycaemia resulting from absolute deficiency of insulin affecting a heterogeneous group of people Type 2 diabetes is a metabolic disease characterised by hyperglycaemia resulting from relative insulin deficiency and insulin resistance affecting a heterogeneous group of people (2). Hypoglycaemia Hypoglycaemia results from an imbalance between glucose supply, glucose utilization, and insulin levels resulting in more insulin than is needed at that time (3) Hypoglycaemia is defined as a blood glucose level being equal or less than 4mmols/l, with or without symptoms (1). Hypoglycaemia can occur not only with people who are requiring insulin treatment, but also those who are taking oral anti-diabetic tablets such as gliclazide or Pioglitazone (1). Insulin and Sulphonylureas (such as gliclazide) tablets give most risk of hypoglycaemic events. Hypoglycaemic events are common but should not be a daily normality. Hypoglycaemia is a side effect of treatment for diabetes and therefore is unlikely to occur in people treated with diet and exercise alone. Patient perception of hypoglycaemia For the person with diabetes, the fear of having a hypo can outweigh the concern about the Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 4 of 15 future development of complications (4). Patient perception of hypoglycaemia may vary so it is useful to record a blood glucose level prior to giving any treatment to confirm what the patient is feeling is actually a hypoglycaemic event. Hypoglycaemia warning signs may be distorted if a person has had elevated blood glucose levels over some time. These people may experience hypoglycaemia symptoms above 4mmols/l and thus generally should not be treated at this stage (2). However, eating a small amount of complex carbohydrates will help to alleviate the hypoglycaemic symptoms without elevating the glucose level uncontrollably. Hypoglycaemia warning signs Hypoglycaemia symptoms and the level at which they start, vary from person to person. Identifying symptoms most commonly include: Shaking/ tremor/tingling Faintness/weak Feeling of hunger Anxiety Irritability/aggression Sweating Poor concentration/confusion/forgetful Headache Abnormal behaviour Palpitations/tachycardia (5) Loss of hypoglycaemia warning signs Loss of warning signs of hypoglycaemia is common among insulin-treated patients and can be a serious hazard. Very tight control of diabetes lowers the blood glucose concentration needed to trigger hypoglycaemia symptoms and an increase in the frequency of hypoglycaemic episodes reduces the warning symptoms experienced by the patient. Betablockers can also blunt hypoglycaemia awareness and delay recovery. It has been reported that conversion to human insulin from animal insulin also contributes to loss of warning signs (2) . However, it must be highlighted to the patient that any change in insulin product may give rise to altered hypoglycaemic awareness, signs and symptoms; hence the need for the person with diabetes to monitor their blood glucose levels closely in these circumstances. Common causes of hypoglycaemia Identifying precipitating factors that may lead to a hypoglycaemic event may help to prevent or limit occurrence. Precipitating factors include: Inadequate carbohydrate or delayed meal Oral anti-diabetic agents especially Sulphonylureas administered in the elderly Stress and/or hot weather Potentiating drugs such as warfarin or fibrates Too much insulin Excessive or unusual amounts of exercise or activity Hepatic and/or renal disease Change of daily routine (5) Delayed treatment for hypoglycaemia It is essential that all hypoglycaemic episodes are treated immediately. An omission of treatment or delay in treatment can at the very least result in elevated glucose levels due to metabolic changes which are known as re-bound hyperglycaemia, some hours after the event. However, omission of treatment and delays can also lead to confusion, coma, convulsions, brain damage, reduced consciousness, and in severe cases death (5) Glucagon Glucagon is a hyperglycaemic agent that mobilises hepatic glycogen, which is released into the blood as glucose. Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 5 of 15 Groups of patients which hypo treatment and glucagon may be less effective Renal impairment / failure: People with renal impairment or failure are more at risk of unpredictable and prolonged hypoglycaemia as insulin can not be cleared as effectively from the body. In the presence of renal impairment or failure, glycogen stores may be lower than usual and renal glycogen stores absent, thus glucagon therapy may have reduced effect in raising glucose levels. Liver impairment / alcoholics / prolonged starvation / malnourished: People who have liver impairment or failure will be more at risk of unpredictable or prolonged hypoglycaemia as they are unable to store sufficient amounts of glycogen. Glucagon will not be effective in patients whose liver glycogen is depleted. For that reason, glucagon has little or no effect when the patient has been fasting for a prolonged period, is malnourished, has liver impairment or failure, alcoholics or alcohol induced hypoglycaemia In the above cases consideration should be given to earlier use of intravenous glucose, especially if inadequate response to an initial glucagon injection is noted. 5. DUTIES AND RESPONSIBILITIES Registered Nurse / Midwife – Act promptly by initiating appropriate treatment as outlined in this guideline with regular follow up monitoring of glucose levels and examination of possible causes to prevent further occurrences. Doctors – All patients should be assessed for the need to prescribe GlucaGen HypoKit 1mg in addition to usual hypoglycaemia treatment options, but particular consideration should be given to those patients experiencing sudden severe hypoglycaemic episodes, or those who do not experience hypoglycaemia warning signs. Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 6 of 15 6. PROCESS To minimise risk of hypoglycaemia: Patients should be assessed on admission as to: Their usual hypo signs How often and when they suffer from hypos Their usual treatment of hypos Ensure that the patient: knows the routine of the ward regarding meals and snacks Has a supply of snacks close to hand Receives their diabetic medication at the appropriate times in relation to meals On recognition of a hypo: Test capillary glucose if possible and initiate treatment immediately using HYPOBOX Hypoglycaemia Kit to prevent further harm to the patient. If patient is asymptomatic repeat test. MILD Alert, conscious and able to swallow MODERATE Drowsy, uncooperative and/or risk of choking STEP ONE STEP ONE STEP ONE Initially administer ONE tube x 25g Glucose 40% oral gel from the hypoglycaemia kit allowing it to be swallowed Initially administer ONE or TWO tube(s) of 25g Glucose 40% oral gel from the hypoglycaemia kit, inside the cheek. Massage outside of cheek allowing it to be absorbed. Check ABC Place in recovery if required Administer intramuscular injection (lateral arm or thigh) of Glucagon using GlucaGen HypoKit 1mg stored in locked ward fridge Do not leave patient STEP TWO Repeat at 5-15 min intervals as necessary depending on patient symptoms and glucose concentrations. If Glucogel unavailable use 10-20g fast acting glucose such as 2 tsp sugar in water or 200ml glass of fizzy drink or patients own remedy if appropriate STEP TWO Repeat using one tube at 5-15 min intervals as necessary depending on patient symptoms and glucose concentrations. If patient deteriorates move to red guidance If patient deteriorates move to yellow or red guidance STEP THREE To prevent glucose levels falling again ensure long-acting carbohydrates such as adequate amounts of bread/potato/rice is eaten with a meal or a snack such as 2-3 biscuits, fruit, current bun is eaten if it is not a meal time. Continue regular monitoring for 24 – 48 hours and reflect on cause of hypo event STEP THREE Follow as per green step three SEVERE Call 2222 and Fast Blp Doctor Unconscious and potential for no gag reflex, and/or fitting, and/or NBM NB: Glucagon has little effect in chronically malnourished / alcoholics / prolonged starvation / severe liver disease / renal failure If no reponse from Glucagon within 5-10 minutes, doctor to administer IV injection of 50mls of 20% glucose, administered slowly through a large vein and large gauge cannula. The remaining 50mls may be given after 10mins if blood glucose less than 4mmol/L. STEP TWO Once conscious, follow yellow step one and two STEP THREE Follow as per green step three INSULIN SHOULD NOT BE OMITTED FOLLOWING AN EPISODE OF HYPOGLYCAEMIA. If you are concerned, patients should be assessed for a smaller insulin dose rather than an omission. Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 BGLs will be erratic following a hypoglycaemic event and patients can feel quite unwell for up to 48 hours. Review date 12/10/2016 Page 7Specialist of 15 Team if concerned Refer to Diabetes 7. TRAINING REQUIREMENTS All staff involved in clinical care of inpatients who have diabetes should have read this guideline and may have further educational input via DIPPIE. PHT staff will be informed of this guideline and may cascade down to junior staff and students 8. REFERENCES AND ASSOCIATED DOCUMENTATION 1) Diabetes UK (2011) [online] Monitoring Your Health / Glucose Levels. www.diabetes.org.uk TEL: 020 73231531 2) British National Formulary 60. Section 6.1, Drugs Used In Diabetes. BMJ Group. London 3) Turner H and Wass JA (2007). Oxford Handbook of Diabetes. Oxford University Press. Oxford 4) Drucquer MH & McNally P (1998) Diabetes Management Step by Step Blackwell Science. London, Oxford 5) Bailey C and Feher MD (2009). Diabetes Therapies,Treating hyperglycaemia. MedEd UK Ltd. Halesowen 9. EQUALITY IMPACT STATEMENT Portsmouth Hospitals NHS Trust is committed to ensuring that, as far as is reasonably practicable, the way we provide services to the public and the way we treat our staff reflects their individual needs and does not discriminate against individuals or groups on any grounds. This policy has been assessed accordingly Our values are the core of what Portsmouth Hospitals NHS Trust is and what we cherish. They are beliefs that manifest in the behaviours our employees display in the workplace. Our Values were developed after listening to our staff. They bring the Trust closer to its vision to be the best hospital, providing the best care by the best people and ensure that our patients are at the centre of all we do. We are committed to promoting a culture founded on these values which form the ‘heart’ of our Trust: Respect and dignity Quality of care Working together No waste This policy should be read and implemented with the Trust Values in mind at all times. Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 8 of 15 Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 9 of 15 10. MONITORING COMPLIANCE WITH PROCEDURAL DOCUMENTS Minimum requirement to be monitored Lead Management of patients with diabetes who are suffering from hypoglycaemic episodes Ward nursing staff, ward doctors, & specialist diabetes team Unfavorable hypoglycaemia management issues. Specialist diabetes team Management of hypoglycaemia Specialist diabetes team Tool Daily diabetes ward rounds Adverse incident reporting & ward rounds Audits Frequency of Report of Compliance Daily Reporting arrangements Policy audit report to: Quarterly Annual Specialist diabetes team Specialist diabetes team Policy audit report to: Lead(s) for acting on Recommendations Specialist diabetes team Specialist diabetes team Policy audit report to: Specialist diabetes team Specialist diabetes team This document will be monitored to ensure it is effective and to assurance compliance. Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 10 of 15 Appendix A Equality Impact Screening Tool To be completed and attached to any procedural document when submitted to the appropriate committee for consideration and approval for service and policy changes/amendments. Stage 1 - Screening Title of Procedural Document: Hypoglycaemia management for the Adult Inpatient with Diabetes Date of assessment 8th April 2011 Responsible Department Academic Department of Diabetes and Endocrine Name of person completing assessment Anita Thynne. Job Title Diabetes Specialist Nurse Does the policy/function affect one group less or more favourably than another on the basis of : Yes/No Age No Disability No Comments Learning disability; physical disability; sensory impairment and/or mental health problems e.g. dementia Ethnic Origin (including gypsies and travellers) No Gender reassignment No Pregnancy or Maternity No Race No Sex No Religion and Belief No Sexual Orientation No If the answer to any of the above questions is NO, the EIA is complete. If YES, a full impact assessment is required: go on to stage 2, page 2 More Information can be found be following the link below www.legislation.gov.uk/ukpga/2010/15/contents Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 11 of 15 Stage 2 – Full Impact Assessment What is the impact Level of Impact Mitigating Actions (what needs to be done to minimise / remove the impact) Responsible Officer Monitoring of Actions The monitoring of actions to mitigate any impact will be undertaken at the appropriate level Specialty Procedural Document: Specialty Governance Committee Clinical Service Centre Procedural Document: Clinical Service Centre Governance Committee Corporate Procedural Document: Relevant Corporate Committee All actions will be further monitored as part of reporting schedule to the Equality and Diversity Committee Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 12 of 15 Appendix B Checklist for the Review and Ratification of Procedural Documents and Consultation and Proposed Implementation Plan To be completed by the author of the document and attached when the document is submitted for ratification: a blank template can be found on the Trust Intranet CHECKLIST FOR REVIEW AND RATIFICATION TITLE OF DOCUMENT BEING REVIEWED: 1 2 4 Is the title clear and unambiguous? Yes Will it enable easy searching/access/retrieval?? Yes Is it clear whether the document is a policy, guideline, procedure, protocol or ICP? Yes Introduction 6 Is there a standard front cover? Yes Is the document in the correct format as per Policy for the Development and Management of Procedural Documents? Yes Does the scope include the paragraph relating to ability to comply, in the event of a infection outbreak, flu pandemic or any major incident? Yes Are the roles and responsibilities clearly explained? Yes Does it fulfill the requirements of the relevant NHSLA Risk Management Standard? (where applicable) Yes Evidence Base Does the document identify which committee/group has approved it? Yes Is the Ratification Checklist complete overleaf Yes Are minutes of ratification committee attached showing ratification? Yes Process to Monitor Compliance and Effectiveness Yes Dissemination and Implementation Is a completed proposed implementation plan attached? 7 Yes Review Date Is the review date identified? 6 Yes Approval Route Are there measurable standards or KPIs to support the monitoring of compliance with the effectiveness of the document? 7 Yes Content Is the type of evidence to support the document explicitly identified? 5 COMMENTS Title Are reasons for the development of the document clearly stated? 3 YES/NO N/A Yes Equality and Diversity Is a completed Equality Impact Assessment attached? Yes Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 13 of 15 If answers to any of the above questions is ‘no’, then please do not send it for ratification Checklist for the Review and Ratification of Procedural Documents and Consultation and Proposed Implementation Plan CONSULTATION AND PROPOSED IMPLEMENTATION PLAN Contact Details Name and details of key person developing information and responsible for review Development Team and Peer Review Groups /committees / individuals involved in the development and consultation process Name Anita Thynne Job Title Diabetes specialist nurse Department Diabetes and endocrinology CSC/Location Medicine Telephone Ext 6260 Email [email protected] (a) Anita Thynne Lead Inpatient Diabetes Specialist Nurse (b) peer reviewed by Diabetes Specialist Nursing team (c) peer reviewed by Diabetes/Endocrinology Consultant team (d) Badrriyya Mohamedali Rotational CHAT pharmacist Implementation Plan Author(s) This should be signed by the main author What training is required to support implementation? Education of nurses by the Diabetes team and/or pharmacy regarding change in policy and practice. Outline any additional activities to support implementation Printing of new treatment algorithm cards to reflect change in practice which will be placed in each orange hypo-box. Name Posters to be displayed in treatment rooms highlighting change in policy. Job Title Signature Anita Thynne Lead Inpatient Diabetes Specialist Nurse If, as the author, you are happy that the document complies with Trust policy, please sign above and send the document, with this paper, with the Equality Impact Assessment to the chair of the committee/group where it will be ratified. To aid distribution all documentation should be sent electronically wherever possible. Name of Ratification Committee Formulary and Medicines Group Date of Ratification (minutes enclosed) 19th September 2014 Name/Signature of Chair Dr Mike Stewart Once the committee/group is happy to ratify this document, would the chair please sign above and send the policy together with this document, the Equality Impact Assessment, and the relevant section of the minutes to the Risk Analyst. To aid distribution all documentation should be sent electronically wherever possible. Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 14 of 15 Hypoglycaemia Management of the Adult Inpatient with Diabetes Issue 2 13/10/2014 Review date 12/10/2016 Page 15 of 15