Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
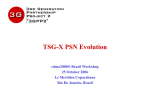
CHRONIC AND INTERVENTIONAL PAIN ORIGINAL ARTICLE A Cadaveric Study Evaluating the Feasibility of an Ultrasound-Guided Diagnostic Block and Radiofrequency Ablation Technique for Sacroiliac Joint Pain Shannon L. Roberts, BA,* Robert S. Burnham, MD, MSc,†‡ Anne M. Agur, PhD,*§ and Eldon Y. Loh, MD|| Background and Objectives: Ultrasound (US)–guided diagnostic block/radiofrequency ablation (RFA) along the lateral sacral crest (LSC) has been proposed for managing sacroiliac joint (SIJ) pain. We sought to investigate (1) ease of visualization of bony landmarks using US; (2) consistency of US-guided needle placement along the LSC; and (3) percentage of the posterior sacral network (PSN) innervating the SIJ complex that would be captured if an RFA strip lesion were created between the needles. Methods: In 10 cadaveric specimens, 3 needles were placed bilaterally along the LSC from the first to third transverse sacral tubercles (TSTs) using US guidance. The PSN, SIJ, and needles were exposed, digitized, and modeled 3-dimensionally. Ease of visualization of bony landmarks, frequency of needle placement along the LSC, and percentage of the PSN that would be captured if an RFA strip lesion were created between the needles were determined. Results: The LSC, TST2, TST3, and first to third posterior sacral foramina were easily visualized using US; TST1 was somewhat obscured by the iliac crest in some specimens. Needles were placed along the LSC in 18 of 20 specimens; in the first 2 of 20 specimens, needle 1 was placed at the L5/ S1 facet joint. On average, 93% (95% confidence interval, 87%–98%) of the PSN would be captured if an RFA strip lesion were created between the needles. Conclusions: The findings suggest that US-guided needle placement along the LSC is consistent and could capture most or all of the PSN. A clinical study evaluating the outcomes of this technique is in progress. procedures has increased over the last decade.5,6 Ultrasound eliminates exposure to radiation, increases accessibility, and lowers cost.5,6 A recent anatomical study from our laboratory found that the posterior aspect of the SIJ was innervated by the posterior sacral network (PSN), a fine nerve plexus that received contributions from the lateral branches of the posterior rami of S1–S3 ± L5/S4.7 The PSN consistently coursed over the lateral sacral crest (LSC) between the first and third transverse sacral tubercles (TSTs). Based on the findings of the anatomical study, a US-guided SIJ diagnostic block/RFA technique was proposed using these bony landmarks: the PSN lateral crest technique (Fig. 1). This technique involves creating a block/RFA strip lesion along the LSC from TST1 to TST3 using US guidance. The feasibility, consistency, and effectiveness of US-guided needle placement using the PSN lateral crest technique have not been evaluated in cadaveric specimens. Therefore, the purpose of this cadaveric study was to investigate the (1) ease of visualization of the bony landmarks used for the US-guided PSN lateral crest technique, including the LSC, TST1–TST3, and first to third posterior sacral foramina; (2) consistency of needle placement along the LSC using US guidance; and (3) percentage of the PSN that would be captured if an RFA strip lesion were created along the LSC between the needles. (Reg Anesth Pain Med 2017;42: 00–00) F luoroscopically guided lateral branch radiofrequency ablation (RFA) techniques for sacroiliac joint (SIJ) pain have had limited success.1,2 In a systematic review evaluating the evidence for the effectiveness of fluoroscopically guided lateral branch RFA in treating SIJ pain, King et al.2 concluded that “relief is limited in extent and duration.” This may be partly due to difficulty in identifying the posterior sacral foramina using fluoroscopy.3,4 The use of ultrasound (US) guidance for interventional pain From the *Division of Anatomy, Department of Surgery, University of Toronto, Toronto, Ontario; †Central Alberta Pain and Rehabilitation Institute, Lacombe; and ‡Division of Physical Medicine and Rehabilitation, University of Alberta, Edmonton, Alberta; and §Division of Physical Medicine and Rehabilitation, Department of Medicine, University of Toronto, Toronto; and ||Department of Physical Medicine and Rehabilitation, Western University, London, Ontario, Canada. Accepted for publication August 29, 2016. Address correspondence to: Shannon L. Roberts, BA, Medical Sciences Bldg, Room 1158, 1 King's College Circle, University of Toronto, Toronto, Ontario, Canada M5S 1A8 (e‐mail: [email protected]). This work was presented in part at the International Spine Intervention Society 23rd Annual Scientific Meeting, July 28 to August 1, 2015, Las Vegas, Nevada, and the 1st International Conference on Sacroiliac Joint Surgery, September 18 to 19, 2015, Hamburg, Germany. The authors declare no conflict of interest. Copyright © 2016 by American Society of Regional Anesthesia and Pain Medicine ISSN: 1098-7339 DOI: 10.1097/AAP.0000000000000515 METHODS Ten fresh cadaveric specimens (5 male/5 female) with a mean age of 79.6 ± 10.0 years were studied bilaterally (n = 20). Specimens had no visible evidence of pathology, previous surgery, or trauma. Ethics approval was received from the University of Toronto Health Sciences Research Ethics Board. A GE Healthcare Venue 40 US machine (General Electric Healthcare Inc, Little Chalfont, Buckinghamshire, United Kingdom) with a curvilinear transducer (1.8–5 MHz) was used. All procedures were performed by a physical medicine and rehabilitation physician (E.Y.L; right-handed) with 5 years of interventional US experience. Each cadaver was scanned with US to identify any musculoskeletal pathology. If any pathology was present, the specimen was excluded from the study. The US-guided PSN lateral crest technique was performed bilaterally on the specimens included in the study. To perform the PSN lateral crest technique, first, key bony landmarks were identified with US in the transverse plane. The bony landmarks included the (1) fourth posterior sacral foramen at the level of the sacral cornua and (2) first to third posterior sacral foramina and their respective TSTs (TST1–TST3) on the LSC. The clinician (E.Y.L.) placing the needles recorded if each of the bony landmarks (LSC, TST1–TST3, and first to third posterior sacral foramina) could be visualized easily or with difficulty in each specimen. Under US guidance, three 22-gauge, 3.5-inch spinal needles were placed bilaterally along the LSC from TST1 to TST3 using the TSTs as landmarks. An out-of-plane approach was used to place the needles along the LSC at TST2 and TST3. An approach Regional Anesthesia and Pain Medicine • Volume 42, Number 1, January-February 2017 1 Copyright © 2016 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited. Roberts et al Regional Anesthesia and Pain Medicine • Volume 42, Number 1, January-February 2017 surfaces of the sacrum, including the posterior sacral foramina, LSCs, and TSTs; hip bones adjacent to the SIJ; L5 vertebra; coccyx; and interosseous sacroiliac ligaments were digitized. The digitized nerve, needle, and osseoligamentous data were reconstructed 3-dimensionally using Autodesk Maya 2016 (Autodesk Inc, San Rafael, California) with custom plug-ins developed in our laboratory. A comprehensive 3-dimensional model of each specimen was constructed that demarcated needle placement relative to the PSN and LSC, as in situ. Data analysis included quantification of the (1) frequency with which each of the bony landmarks (LSC, TST1–TST3, and first to third posterior sacral foramina) was visualized easily or with difficulty, (2) frequency of needle placement along the LSC using US guidance, and (3) percentage of the PSN that would be captured if an RFA strip lesion were created along the LSC between the needles. A thermal lesion radius of 4 mm around the needle tip was assumed based on bench studies evaluating thermal lesion morphology using a multitined needle design (the design selected for the clinical study to follow the present cadaveric study).8 If a branch would be spared, its location was recorded, and distance from the midline of the RFA strip lesion quantified using the measurement tool in Maya. The data were summarized with descriptive statistics using SPSS Statistics version 23.0 (IBM Corp, Armonk, New York). RESULTS Ease of Visualization of Bony Landmarks Using US FIGURE 1. Location of SIJ block/RFA strip lesion (white line) using the US-guided PSN lateral crest technique. Posterior view of the right side of the cadaveric specimen. P indicates posterior superior iliac spine; S1–S3, lateral branches; black dots, first to third TSTs on LSC. between an out-of-plane and an in-plane approach was used to place a needle at TST1 in order to avoid the iliac crest. Ultrasound images were obtained of each needle placement in situ. To prevent movement of the needle, prior to dissection and digitization, each needle was firmly fixed in the sacrum using a small mallet. This was done to ensure that needle placement and trajectory were not altered. The skin, subcutaneous tissue, thoracolumbar fascia, and fiber bundles of the lumbar multifidus muscle were carefully removed to expose the needles and the posterior aspect of the SIJ bilaterally. The lateral branches of the posterior rami of S1–S3 were traced to the PSN, along with any contributing lateral branches from the posterior rami of L5 and S4. The nerve branches that coursed deep to the short posterior sacroiliac ligaments were separated from the overlying ligaments. Next, the short posterior sacroiliac ligaments were excised, and the nerves were traced to the long posterior sacroiliac ligament. The long posterior sacroiliac ligament and the superficial lamina of the sacrotuberous ligament were removed to complete the exposure of the PSN. All specimens were photographed. Each specimen was fixed to a wooden board with metal plates and screws to prevent movement during digitization. Three reference screws were inserted for later reconstruction of the digitized data. Digitization was carried out using a MicroScribe MLX Digitizer (Immersion Corporation, San Jose, California; accuracy: ±0.0762 mm). First, each needle was digitized and then removed. Next, the PSN and each of its contributing lateral branches were digitized at 1- to 2-mm intervals bilaterally. Then, the posterior 2 The LSC, TST2, TST3, and first to third posterior sacral foramina were easily visualized in all 10 cadaveric specimens bilaterally (n = 20). However, TST1 was difficult to visualize in 1 cadaveric specimen unilaterally (right side) and 3 cadaveric specimens bilaterally, as it was somewhat obscured by the iliac crest (Fig. 2). Frequency of Needle Placement Along the LSC Needles were placed along the LSC in 18 of 20 specimens (Table 1). Most frequently, the needles were located between TST1 and TST3 (13 specimens), followed by TST2 and TST4 (3 specimens) and TST2 and TST3 (2 specimens). High needle placement occurred in the first 2 of 20 specimens in which the procedure was performed. In both specimens, needle 1 was placed at the L5/S1 facet joint, whereas needle 3 was placed at TST2 in 1 specimen and between TST2 and TST3 in the other. In all 7 specimens in which TST1 was difficult to visualize, needles were placed between TST1 and TST3. Percentage of the PSN Captured If RFA Strip Lesion Were Created Between Needles On average, 93% (95% confidence interval, 87%–98%) of the PSN would be captured, 94% in males and 92% in females. The percentage varied depending on the location of the needles (Table 1 and Fig. 3): • TST1–TST3 (13/20 specimens): On average, 97% (95% confidence interval, 94%–100%) of the PSN would be captured, 100% in 9 specimens (Fig. 3, A–C). Four specimens had a small superior lateral branch of S1 that would be spared. In 2 of these specimens in which 91% and 92% of the PSN would be captured, this branch coursed superior to needle 1, 11.1 and 8.1 mm, respectively (Fig. 3D). In the other 2 specimens in which 89% and 90% of the PSN would be captured, this branch © 2016 American Society of Regional Anesthesia and Pain Medicine Copyright © 2016 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited. Regional Anesthesia and Pain Medicine • Volume 42, Number 1, January-February 2017 Ultrasound-Guided SIJ Block/RFA • TST2–TST4 (3/20 specimens): In 1 specimen, 100% of the PSN would be captured. In another specimen in which 89% of the PSN would be captured, the small superior lateral branch of S1 that coursed 13.4 mm superior to needle 1 would be spared. In the third specimen in which 80% of the PSN would be captured, the lateral branch of S1 that coursed 7.1 mm superior to needle 1 would be spared. • L5/S1 facet joint (2/20 specimens): In 1 specimen in which 50% of the PSN would be captured, needle 3 was placed at TST2, whereas in the other specimen in which 100% of the PSN would be captured, needle 3 was placed between TST2 and TST3. The inferior lateral branch of S2 (6.0 mm inferomedial to needle 3) and the lateral branch of S3 (14.5 mm inferior to needle 3) would be spared in the specimen in which 50% of the PSN would be captured. DISCUSSION This is the first cadaveric study to investigate the feasibility, consistency, and effectiveness of US-guided needle placement using the PSN lateral crest technique for SIJ block/RFA. The results suggest that the technique is feasible, needles can be consistently placed along the LSC using US guidance, and most or all of the PSN could be captured. This provides an anatomical basis for future clinical studies evaluating the outcomes of the US-guided PSN lateral crest technique. Bony landmark identification is fundamental to achieving precise needle placement. One of the challenges of fluoroscopically guided periforaminal lateral branch RFA techniques is identification of the posterior sacral foramina.3,4 Kapural et al3 stated that “the posterior sacral foramina are difficult to identify with certainty on most patients.” In contrast, the key bony landmarks for the PSN lateral crest technique (LSC, TST1–TST3, and first to third posterior sacral foramina) can be consistently visualized using US. Initially, TST1 was difficult to visualize in some specimens, but this was overcome by using the first to third posterior sacral foramina to localize TST1–TST3, because the TSTs are located on the LSC at the level of the foramina. These findings suggest that the PSN lateral crest technique may help to achieve greater reproducibility of SIJ block/RFA and would make it possible to perform SIJ block/RFA using US guidance, rather than fluoroscopy, thus eliminating exposure to radiation.7 This would be particularly useful for patients who experience significant pain relief with SIJ RFA but require the procedure to FIGURE 2. Needle placement, transverse US scans of TSTs. A, At the level of TST1. B, At the level of TST2. C, At the level of TST3. IC indicates iliac crest; PSF, posterior sacral foramen. TABLE 1. Percentage of the PSN That Would Be Captured by Location of Needle Placement No. of Specimens coursed medial to the strip lesion that would be created between the needles, 6.6 and 6.5 mm, respectively (Fig. 3E). Of the 7 specimens in which TST1 was difficult to visualize, 100% of the PSN would be captured in 5 specimens, and 89% and 92% in the remaining 2 specimens. • TST2–TST3 (2/20 specimens): In 1 specimen in which 86% of the PSN would be captured, 2 small branches would be spared, the superior lateral branch of S1 (14.3 mm superior to needle 1) and a branch that originated from the inferior lateral branch of S1 (8.4 mm superior to needle 1). In the other specimen in which 90% of the PSN would be captured, a small branch that originated from the lateral branch of S1 (6.9 mm superior to needle 1) would be spared. © 2016 American Society of Regional Anesthesia and Pain Medicine Needle Placement* TST1–TST3 TST2–TST3 TST2–TST4 L5/S1–TST2 L5/S1–TST2/3 Total L/R % of PSN Captured† 13 2‡ 3 1‡ 1‡ 6/7 1/1 2/1 0/1 1/0 97 (mean); CI95, 94–100 86, 90 80, 89, 100 50 100 *One attempt at needle placement with no previous practice. †If an RFA strip lesion were created between the needles. ‡First four specimens in which the procedure was performed. CI95 indicates 95% confidence interval; L, left; L5/S1, L5/S1 facet joint; R, right. 3 Copyright © 2016 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited. Roberts et al Regional Anesthesia and Pain Medicine • Volume 42, Number 1, January-February 2017 FIGURE 3. Cadaveric dissections and 3-dimensional models of US-guided needle placement along the LSC, posterior views. A–C, One hundred percent of the PSN would be captured. D, Ninety-two percent of the PSN would be captured; small superior lateral branch of S1 that coursed superior to needle 1 would be spared (solid yellow overlay). E, Eighty-nine percent of the PSN would be captured; small superior lateral branch of S1 would be spared (solid yellow overlay). F, Fifty percent of the PSN would be captured; needle 1 was placed at the L5/S1 facet joint. 4 © 2016 American Society of Regional Anesthesia and Pain Medicine Copyright © 2016 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited. Regional Anesthesia and Pain Medicine • Volume 42, Number 1, January-February 2017 be repeated every 9 to 18 months when pain recurs because of sensory reinnervation. For fluoroscopically guided periforaminal lateral branch RFA techniques, difficulty in identifying the posterior sacral foramina3,4 may result in needle placement within or directly adjacent to the foramina, risking ablation of the sacral spinal nerves.9 This could result in increased pain, incontinence, and lower limb muscle weakness.9 The current study demonstrated that needle placement using the US-guided PSN lateral crest technique is sufficiently lateral to the posterior sacral foramina to prevent placement within or directly adjacent to the foramina, yet sufficiently medial to capture most or all of the PSN. Precise needle placement is essential to optimize nerve ablation rates and therefore clinical outcomes. Another challenge of fluoroscopically guided periforaminal lateral branch RFA techniques is variations in the number and location of lateral branches as they emerge from the posterior sacral foramina.3,4,7,10,11 In a retrospective case series of the treatment of patients with chronic SIJ origin pain, Kapural et al3 concluded that as a result of anatomical variations “it is likely that in some patients lateral branches were not effectively treated.” In comparison, the US-guided PSN lateral crest technique targets the PSN more laterally, where it consistently courses over the LSC between TST1 and TST3.7 When needles were placed between TST1 and TST3 using this technique in the current study, most or all of the PSN would be captured. The current study demonstrated that needles can be consistently placed along the LSC using US guidance. There was a learning curve associated with the PSN lateral crest technique, as evidenced by high or low needle placement in the first specimens in which the procedure was performed. However, it should be noted that there was only 1 attempt at needle placement with no previous practice. High and low needle placements were not as effective as needle placement between TST1 and TST3. High needle placement beginning at the L5/S1 facet joint demonstrated the importance of extending the block/RFA strip lesion to TST3, as only 50% of the PSN would be captured when needle 3 was placed at TST2, compared with 100% when it was placed between TST2 and TST3. Low needle placement beginning at TST2 would still be sufficient to capture the majority of branches of the PSN, 89% on average, and depending on anatomical variations may capture all branches of the PSN in some individuals. Needle placement between TST1 and TST3 was most effective, as evidenced by an average of 97% of the PSN that would be captured, with 100% in the majority of specimens. The only branch that would be spared in 4 specimens was a very small superior lateral branch of S1 (diameter, <0.36 mm7) when it coursed superior to TST1 or penetrated the interosseous sacroiliac ligament medial to the LSC. To capture these branches, it is important to start the block/RFA strip lesion at or just superior to the superior border of TST1. These findings suggest that if needle placement occurs along the LSC the majority of branches of the PSN could be captured. An out-of-plane approach was used to place needles along the LSC at TST2 and TST3. The needles were inserted distally and directed proximally. To avoid the iliac crest at TST1, the needle was directed from medial to lateral in a plane slightly medial to that of the out-of-plane approach. This approach would place an RF electrode nearly perpendicular to the periosteum. If a traditional single monopolar RF electrode is placed perpendicular to the periosteum, only a relatively small perielectrode thermal lesion at the level of the periosteum would result.12,13 However, multitined electrodes, particularly if aligned in a multipolar configuration, would create a larger targeted lesion along the LSC periosteum, well suited to capture the PSN.8,14 In the current study, the consistency of US-guided needle placement along the LSC from TST1 © 2016 American Society of Regional Anesthesia and Pain Medicine Ultrasound-Guided SIJ Block/RFA to TST3 (3 needle placements) has been assessed. Assuming an ideal interelectrode bipolar burn distance for multitined electrodes is 1.5 cm,8 an average of 2 to 3 bipolar burns (3–4 electrode placements) would be required to ensure that the lesion is continuous. A parallel trajectory between electrodes would maintain a consistent interelectrode distance at the level of the periosteum. In addition, the authors suggest drawing a line on the skin along the LSC, with bisecting lines 1.5 cm apart between TST1 and TST3 (at the level of the first and third posterior sacral foramina) to assist in maintaining a consistent interelectrode distance. The limitations of the current study include a small sample size and using 1 proceduralist to perform the US-guided PSN lateral crest technique. As this was a cadaveric study, the effectiveness of the US-guided PSN lateral crest technique on clinical outcomes requires in vivo investigation. In vivo investigation would permit further stratification of pathologies to define the effectiveness of the technique in reducing pain. The findings of this cadaveric study suggest that US-guided needle placement along the LSC is consistent and could capture most or all of the PSN innervating the SIJ complex. Because the PSN lateral crest technique uses US guidance, it eliminates exposure to radiation associated with current fluoroscopically guided lateral branch RFA techniques and could be performed as an office procedure. A clinical study evaluating the outcomes of the US-guided PSN lateral crest technique is in progress. ACKNOWLEDGMENTS The authors thank William Wood for his valuable technical assistance, the members of the Parametric Human Project for their discussions and insights, and the individuals who donate their bodies and tissue for the advancement of education and research. REFERENCES 1. Aydin SM, Gharibo CG, Mehnert M, Stitik TP. The role of radiofrequency ablation for sacroiliac joint pain: a meta-analysis. PM R. 2010;2: 842–851. 2. King W, Ahmed SU, Baisden J, et al. Diagnosis and treatment of posterior sacroiliac complex pain: a systematic review with comprehensive analysis of the published data. Pain Med. 2015;16:257–265. 3. Kapural L, Nageeb F, Kapural M, Cata JP, Narouze S, Mekhail N. Cooled radiofrequency system for the treatment of chronic pain from sacroiliitis: the first case-series. Pain Pract. 2008;8: 348–354. 4. Cosman ER Jr, Gonzalez CD. Bipolar radiofrequency lesion geometry: implications for palisade treatment of sacroiliac joint pain. Pain Pract. 2011;11:3–22. 5. Peng PWH, Cheng P. Ultrasound-guided interventional procedures in pain medicine: a review of anatomy, sonoanatomy, and procedures. Part III: shoulder. Reg Anesth Pain Med. 2011;36:592–605. 6. Wilson CP, Scully MW, Rawlings CJ. Evolving role of ultrasound in therapeutic injections of the upper extremity. Orthopedics. 2015;38: e1017–e1024. 7. Roberts SL, Burnham RS, Ravichandiran K, Agur AM, Loh EY. Cadaveric study of sacroiliac joint innervation: implications for diagnostic blocks and radiofrequency ablation. Reg Anesth Pain Med. 2014;39:456–464. 8. Nimbus Multi-tined Expandable Electrode for Radiofrequency Ablation Selected Technique Summary Rev 07/13. Vancouver, WA: RS Medical; 2013. 5 Copyright © 2016 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited. Roberts et al Regional Anesthesia and Pain Medicine • Volume 42, Number 1, January-February 2017 9. Cohen SP, Chen Y, Neufeld NJ. Sacroiliac joint pain: a comprehensive review of epidemiology, diagnosis and treatment. Expert Rev Neurother. 2013;13:99–116. 10. Yin W, Willard F, Carreiro J, Dreyfuss P. Sensory stimulation-guided sacroiliac joint radiofrequency neurotomy: technique based on neuroanatomy of the dorsal sacral plexus. Spine. 2003;28:2419–2425. 11. Patel N, Gross A, Brown L, Gekht G. A randomized, placebo-controlled study to assess the efficacy of lateral branch neurotomy for chronic sacroiliac joint pain. Pain Med. 2012;13:383–398. 6 12. Bogduk N, Macintosh J, Marsland A. Technical limitations to the efficacy of radiofrequency neurotomy for spinal pain. Neurosurgery. 1987;20: 529–535. 13. Cosman ER Jr, Dolensky JR, Hoffman RA. Factors that affect radiofrequency heat lesion size. Pain Med. 2014;15:2020–2036. 14. Wright RE, Allan KJ, Bainbridge JS. In and ex vivo validation of a novel technique for radiofrequency denervation of the dorsal sacroiliac joint—including a case study [abstract]. Reg Anesth Pain Med. 2013; 38(5 suppl 1):E161–E162. © 2016 American Society of Regional Anesthesia and Pain Medicine Copyright © 2016 American Society of Regional Anesthesia and Pain Medicine. Unauthorized reproduction of this article is prohibited.