Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Cell encapsulation wikipedia , lookup
Drug interaction wikipedia , lookup
Discovery and development of tubulin inhibitors wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Drug design wikipedia , lookup
Plateau principle wikipedia , lookup
Neuropharmacology wikipedia , lookup
Theralizumab wikipedia , lookup
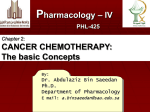
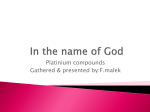
SUPPLEMENTARY MATERIAL, Kanigel Winner et al, 2015 Model Assumptions: Time simulated in the OvTM model replicates the length of patient data sets, even if those times are shorter than drug half-life, as in the case of therapeutic antibodies. Time simulated is also limited by the diffusion rates of drugs. In order to track all contacts between a molecule and any cell within its diffusion trajectory, time steps are set so that the diffusion length of the drug is one cell diameter. The resulting number of steps to simulate a drug time course requires 6 to 9 days per simulation. Because our biological model is of SKOV3.ip1 cells, wherever possible, parameters experimentally derived from this cell line are used in the model. If, in a given paper, explicit data for SKOV3 or SKOV3.ip1 cells is not included, but SKOV3.ip1 is described as similarly resistant or in the same class as another cell line, then data for the similar cell line is used. Fits of cisplatin extracellular exposure to cancer cell lines from El-Kareh, 2004 (1) approximate the IC50 for the most sensitive cell line tested by Mistry et al., 1992 (2). Factors affecting drug distribution in peritoneal fluid, blood, and tissue (pharmacokinetics) We use data for unbound concentration of drug rather than total drug, as "the action exerted by drugs is generally more closely related to unbound than total concentration of drugs" (3). “Effective” penetration rates in tumor tissue or spheroids, which include all processes that might alter penetration from the rate found in water, are used to parameterize diffusion for cisplatin and pertuzumab. We parameterize diffusion from empirically derived effective diffusion coefficients for non-binding molecules in tumor tissue in vivo. Sodium fluorescein (molecular weight 376 Da (4)) is used to represent cisplatin (molecular weight 300.5 Da). Pertuzumab effective diffusion in avascular tumors is represented by non-binding IgG either measured directly by FRAP in SKOV3.ip1 spheroids in vitro, or penetration in vascularized tumors by non-binding IgG measured in vivo (5, 6). These coefficients are affected by unmeasured events of convection, binding by target and non-target molecules, tortuosity of interstitial space, inhibition by the fiber mesh of the extracellular matrix (antibodies are ~20 nm at their widest (7)), and other barriers to penetration. We find the rough FRAP in vitro estimate of 13 µm2/sec to be nearly identical to the in vivo estimate of 10 µm2/sec (5) and 13 µm2/sec (6). Penetration rates and accumulation patterns of drugs in spheroids grown in vitro can be significantly different depending on the drug (8). We use penetration rates of therapeutic antibodies in SKOV3.ip1 spheroids to calculate effective passive diffusion coefficients from the IP surface of ovarian tumors, and compare these to rates derived for tumor tissue in the literature. Target-specific effective diffusion coefficients of pertuzumab in SKOV3.ip1 spheroids was 1000-fold slower than in vivo penetration rates of non-specific IgG from the literature (6), (6.2 E-10 cm2/sec vs. 1.33 E-07 cm2/sec), implicating a slowdown of penetration caused solely by binding to target proteins. We add the physical barrier of low-permeability vascular endothelium to the penetration of non-specific antibodies, as recommended by Thurber, et al., 2011 (5). We decrease the percentage of IV antibody available at the vessel surface from the plasma concentration by the ratio called the Biot number by Thurber et al (5). (For this paper, the Biot number = 0.0225 for the average diameter of vessels found in our human ovarian tumors (Table 1). This is similar to the value 0.024 calculated in (5)). This number concurs with a reflection coefficient of 0.95-0.98 for antibodies inside of vessels (9), and will likely be higher for “leaky” vessels often found in tumors. We therefore assume relatively intact, non-leaky vessels in simulations, unless explicitly stated for our leaky simulations. We use effective penetration and cell uptake as the sole barriers to small-molecule drug penetration on the assumption that tumor vessels are well-perfused, as discussed by Thurber et al. (5) and do not explicitly model cisplatin depletion along the length of blood vessel segments, although this could be addressed in later models. IV and IP primary compartment drug concentrations are derived directly from patient data, removing the need to account for dilution by blood in the IV case or a delivery volume (liters of saline) in the IP case. Drugs have a half-life in the body that is affected by binding to the total cell population, to soluble components in the plasma, and filtering in the liver and kidneys. We do not add any further decay processes in blood or peritoneal fluid, again using only empirically measured concentrations in patients. Our parameters for exchange of cisplatin between the blood (IV) and peritoneal (IP) compartments are based on Casper et al., who simultaneously measured the concentration of platinum in plasma and ascites after administration of cisplatin by either route (10). Because we do not have such simultaneous measurements from patients for IV delivery of pertuzumab, the pertuzumab simulations base the concentrations in the primary compartment on patient data, while concentrations in the secondary compartments rely on IP/IV and IV/IP ratios determined experimentally in rats (11). Fits calculated for cisplatin (10) and mitomycin C (12) of IP-post-IV ratios in patients show similar shapes to that of the fit for the IP-post-IV ratio for IgG in rats (11) (a fourth-order fit in which the ratio drops slightly as drug in the two compartments approaches equilibrium). Due to the similarity in curve shape between human and rat ratios IP-post-IV, and for consistency of the pharmacokinetic environment in the simulations, we use antibody ratios from rats both IV-post-IP and IP-post-IV. It is notable that analysis of IV-post-IP ratios over time shows a 20-fold increase in slope when comparing IgG in rats (11) with IgGimmunoconjugate in humans (0.04429 vs. 0.001922, respectively) (13); this means that our model may over-estimate IV concentration of pertuzumab post-IP injection. However, for comparison between the primary IP and primary IV simulations, compartment ratios will be consistent. IP and IV administration time courses for cisplatin are fit to curves for a 60 mg/m2 dosage (10). IP administration time course of antibody is fit to a curve for 5 mg/kg of immunotoxin conjugate in 2 liters of saline, and IV administration is fit to a curve for 5 mg/kg pertuzumab (14). The complete curves for drug concentrations are comprised of one to three fits used in sequence that may include 1) an infusion period, 2) a post-infusion plateau period, and 3) a decay period. Supplementary Table 2 details all fits for each of the four drug delivery scenarios: cisplatin IP, cisplatin IV, pertuzumab IP, and pertuzumab IV. In the case of pertuzumab IP, one fit describes the complete drug delivery period. The range of R2 for fits in Table 1 and Supplementary Table 1 is 0.80 to 0.99, and the majority of fits have R2 > 0.95. R2 values along with examination of the plots of residuals for overand under-fitting indicated good to excellent fits to data sets in all cases. The cisplatin threshold for 50% SKOV3 cell death (IC50) is 52.1 µM accumulated per cell during a 2hour exposure to a 38.3µM solution based on (2). Accumulation over 2 hours is described as linear in all cell lines at concentrations up to 50µM cisplatin. However, we use our own exponential fit to data in (2) on accumulation in SKOV3 cells during 2-hour exposures to a range of concentrations, R2 = 0.9999, in the model. Accumulation is discrete, calculated as the amount of cisplatin that would have accumulated at the current concentration over 2 hours x the time step duration relative to 2 hours. Cisplatin accumulation was modeled in micromolar (μM) units of concentration, and results were converted to molecules per cell accumulated. We consider pertuzumab binding to ErbB2 irreversible once antibody levels drop enough to allow a net loss of antibody from the cell surface. Irreversible binding of antibody is observed in (15). This “irreversible binding” includes rapid internalization of antibody-tagged ErbB receptors that can occur in minutes (16, 17). Aside from any released antibody implicit in the net accumulation resulting from Kd calculations (while concentrations are high enough to cause net positive binding at the cell), we do not model release of antibodies from ErbB2. The Kd (equilibrium coefficient, or inverse affinity) of pertuzumab is 9.1nm, making it a high-affinity antibody (16, 17). Antibody bound after each time step is calculated as: (𝐸𝑟𝑏𝐵2𝑇 + 2 ∗ 𝐼𝑔𝐺𝑇 + 𝐾𝑑𝑃𝑒𝑟𝑡 ) − ( ) (√((𝐸𝑟𝑏𝐵2𝑇 + 2 ∗ 𝐼𝑔𝐺𝑇 + 𝐾𝑑𝑃𝑒𝑟𝑡 )2 − 8 ∗ (𝐸𝑟𝑏𝐵2𝑇 ∗ 𝐼𝑔𝐺𝑇 ))) 𝐼𝑔𝐺𝑁𝑒𝑤𝑙𝑦 𝐵𝑜𝑢𝑛𝑑 = 4 where ErbB2T = total receptors (bound and unbound), IgGT = total pertuzumab (bound and unbound) after the influx of new, unbound pertuzumab, but before binding, and KdPert is the dissociation constant for pertuzumab (9.1nM) in which antibody is bound bi-valently (18). Thresholds for tumor cell color changes in the model for pertuzumab are at 100,000 receptors bound for initiation of antibody-dependent cell-mediated cytotoxicity, and 95% of 2 million total on the cell surface, to mark near-complete saturation. Cisplatin accumulation was modeled in micromolar (μM) units of concentration, and results were converted to molecules per cell accumulated for discussion in the text and figures. Statistical significance of vascular density measurements Percent vascular area for the two tumor sites, bowel (n=9) and omentum (n=9), came from the same continuous distribution (p=0.60 for the two-sample KS goodness-of-fit hypothesis test). A oneway analysis of variance test (ANOVA) showed no statistical difference among any patient's mean % vascular area (p = 0.318. Finally, the linear regression between the points for paired bowel and omentum tumors for each patient is not significant (p=0.79, R2=0.01) indicating no statistical correlation between percent vascular area at the two sites (Supplementary Figure 1). Each patient is represented by a point on the graph. (All tests were conducted in Matlab 2014b for 64-bit OSX.) Based on these tests, we calculate that the sample mean for n=18 tumors is 4.85% vascular area, with standard deviation=2.43% and 95% confidence interval=3.64% to 6.05%. Although our data sample sizes are small and are not normally distributed (for the one-sample KS goodness-of-fit hypothesis test for continuous distributions, p=0.01 for bowel, p=0.01 for omentum, p=7.8 e-05 for pooled bowel and omentum (n=18), where a significant p value indicates rejection of a standard normal distribution), the ANOVA is usually robust to such violations of its assumptions. In our models we consider percent vasculature areas from 2% to 10% which represent the extremes of observations in the patient tumors. Supplementary Figure 2 shows box plots indicating the means, quartiles, and farthest outliers for bowel, omentum, and pooled bowel and omentum samples. Supplementary Figure 1. Vascular Densities in Bowel and Omentum Metastatic Sites for Individual Patients Do Not Correlate (Linear Regression Analysis) Supplementary Figure 1. Percent vascular area in the omental metastatic tumor vs. percent vascular area in the bowel metastatic tumor from the same patient. A linear regression shows no correlation between percent vascular area in these two tumor sites within patients (p = 0.79). Supplementary Figure 2: Box Plots of Vascular Density in Patient Tumor Samples Supplementary Figure 2. Box Plots of Vascular Density in Patient Tumor Samples Box plots of the vascular densities in bowel, omentum, and all tumors, demonstrate that omentum and bowel percent vascular area have similar distributions. This is also true according to the 2-sample KolmogorovSmirnoff goodness-of-fit test, which shows that the two tumor populations come from the same distribution (p=0.60). Supplementary Table 1: Concentration Fits for IP and IV Compartments Concentration over time Fit Units Cisplatin IV concentration during 15-minute IV infusion [𝐶𝐼𝑉𝐼𝑛𝑓𝑢𝑠𝑖𝑜𝑛 ](𝑡) = 0.3725 ∗ 𝑡 μM, t = 0 to 15 min Cisplatin IV plateau concentration between end of described infusion and first data point [𝐶𝐼𝑉𝑃𝑜𝑠𝑡−𝑖𝑛𝑓𝑢𝑠𝑖𝑜𝑛,𝑃𝑟𝑒−𝑑𝑎𝑡𝑎 ] = 5.59 μM, t = 15 to 20.7 min Cisplatin IV concentration (dosage = 60 mg/m2) 3 μM, t = 20.7 min to end of data set [𝐶𝐼𝑉 ](𝑡) = −0.000001154 ∗ 𝑡 + 0.0005737 ∗ 𝑡 2 − 0.09922 ∗ 𝑡 + 5.973 3 Source (10) (10) (10) Cisplatin IP-post-IV delivery concentration [𝐶𝐼𝑃−𝑝𝑜𝑠𝑡−𝐼𝑉 ](𝑡) = −1.154𝐸 − 06 ∗ 𝑡 + 0.0005737 ∗ 𝑡 2 − 0.09922 ∗ 𝑡 + 5.973 μM, t = 0 min to end of data set Cisplatin intraperitoneal concentration (first data point) [𝐶𝐼𝑃𝑃𝑟𝑒−𝑑𝑎𝑡𝑎 ] = 64.63 μM, t = 0 min to 22.4 min (10) Cisplatin intraperitoneal concentration (dosage = 60 mg/m2) [𝐶𝐼𝑃 ](𝑡) = 163.3 ∗ 𝑡 −0.2859 − 28.31 μM, t = 22.4 min to end of data set (195.4 min total) (10) (10) 4 Cisplatin IV-post-IP concentration ratio [𝐶𝐼𝑉−𝑝𝑜𝑠𝑡−𝐼𝑃 ](𝑡) = [𝐶𝐼𝑃 ](𝑡) ∗ ( −7.245𝑒 − 09 ∗ 𝑡 + 2.772𝐸 − 06 ∗ 𝑡 3 − 0.0003881 ∗ 𝑡 2 + 0.02126 ∗ 𝑡 + 0.1941) μM, t = 15 min to end of data set Pertuzumab intravenous concentration during infusion [𝑃𝐼𝑉𝐼𝑛𝑓𝑢𝑠𝑖𝑜𝑛 ](𝑡) = 2.358𝑒 + 04 ∗ 𝑡 + 147.8 molecules/ cell volume, t = 0 to 3.68 hr (first time point) (14) Pertuzumab intravenous concentration (dosage =5 mg/kg) [𝑃𝐼𝑉 ](𝑡) = 200700 ∗ 𝑡 − 0.1025 – 91370 molecules/ cell volume, t = 3.68 hr to end of data set (14) Pertuzumab IP-post-IV concentration ratio in rats* Pertuzumab IP-post-IV delivery concentration Pertuzumab (immunotoxin conjugate) intraperitoneal concentration (dosage = 5 mg/kg)* Pertuzumab IV-post-IP concentration ratio in rats* Pertuzumab IP-post-IV delivery concentration [𝑃𝐼𝑃𝑟𝑎𝑡 ] (𝑡) = −0.00001042 ∗ 𝑡 4 + 0.0004965 [𝑃𝐼𝑉𝑟𝑎𝑡 ] ∗ 𝑡 3 − 0.006146 ∗ 𝑡 2 + 0.0355 ∗ 𝑡 + 0.0005605 [𝑃𝐼𝑃𝑟𝑎𝑡 ] (𝑡) [𝑃𝐼𝑃−𝑝𝑜𝑠𝑡−𝐼𝑉 ](𝑡) = [𝑃𝐼𝑉 ](𝑡) ∗ [𝑃𝐼𝑉𝑟𝑎𝑡 ] t = 0 to 27 hrs (11) molecules/ cell volume, t = 0 to 27 hrs molecules/ cell volume, t = 0 hr to end of data set [𝑃𝐼𝑃 ](𝑡) = 0.02679 ∗ 𝑡 2 + −2.1 ∗ 𝑡 + 92.16 [𝑃𝐼𝑉𝑟𝑎𝑡 ] (𝑡) = 3.913𝑒 − 06 ∗ 𝑡 4 − 0.0002103 ∗ 𝑡 3 [𝑃𝐼𝑃𝑟𝑎𝑡 ] + 0.003897 ∗ 𝑡 2 + 0.01503 ∗ 𝑡 + 0.0004171 [𝑃𝐼𝑃−𝑝𝑜𝑠𝑡−𝐼𝑉 ](𝑡) = [𝑃𝐼𝑉 ](𝑡) ∗ * Value estimated based on data obtained with other IgGs. [𝑃𝐼𝑉𝑟𝑎𝑡 ] (𝑡) [𝑃𝐼𝑃𝑟𝑎𝑡 ] (10) (13) t = 0 to 27 hrs (11) molecules/ cell volume, t = 0 to 27 hrs References for Supplementary Materials 1. El-Kareh AW, Secomb TW. A Theoretical Model for Intraperitoneal Delivery of Cisplatin and the Effect of Hyperthermia on Drug Penetration Distance. Neoplasia (New York, NY). 2004;6:117-27. 2. Mistry P, Kelland LR, Loh SY, Abel G, Murrer BA, Harrap KR. Comparison of cellular accumulation and cytotoxicity of cisplatin with that of tetraplatin and amminedibutyratodichloro(cyclohexylamine)platinum(IV) (JM221) in human ovarian carcinoma cell lines. Cancer Res. 1992;52:6188-93. 3. Henningsson A, Karlsson MO, Viganò L, Gianni L, Verweij J, Sparreboom A. Mechanism-based pharmacokinetic model for paclitaxel. Journal of clinical oncology. 2001;19:4065-73. 4. Nugent LJ, Jain RK. Extravascular diffusion in normal and neoplastic tissues. Cancer Res. 1984;44:238-44. 5. Thurber GM, Weissleder R. A systems approach for tumor pharmacokinetics. PLoS One. 2011;6:e24696. 6. Berk DA, Yuan F, Leunig M, Jain RK. Direct in vivo measurement of targeted binding in a human tumor xenograft. Proc Natl Acad Sci U S A. 1997;94:1785-90. 7. Kienberger F, Mueller H, Pastushenko V, Hinterdorfer P. Following single antibody binding to purple membranes in real time. EMBO reports. 2004;5:579-83. 8. Nederman T, Carlsson J, Malmqvist M. Penetration of substances into tumor tissue--a methodological study on cellular spheroids. In Vitro. 1981;17:290-8. 9. Wang W, Wang EQ, Balthasar JP. Monoclonal antibody pharmacokinetics and pharmacodynamics. Clin Pharmacol Ther. 2008;84:548-58. 10. Casper ES, Kelsen DP, Alcock NW, Lewis JL, Jr. Ip cisplatin in patients with malignant ascites: pharmacokinetic evaluation and comparison with the iv route. Cancer treatment reports. 1983;67:235-8. 11. Wahl RL, Barrett J, Geatti O. The intraperitoneal delivery of radiolabeled monoclonal antibodies: studies on the regional delivery advantage. Cancer Immunology, …. 1988:187-201. 12. Sugarbaker PH. Pharmacokinetics of the peritoneal-plasma barrier after systemic mitomycin C administration. 1996. 13. Pai LH, Bookman MA, Ozols RF, Young RC, Smith JW, 2nd, Longo DL, et al. Clinical evaluation of intraperitoneal Pseudomonas exotoxin immunoconjugate OVB3-PE in patients with ovarian cancer. J Clin Oncol. 1991;9:2095-103. 14. Song P, Krudys K, Grimstein C, Liu Q, Garnett C, Zineh I, reviewers. BLA 125409 Clinical Pharmacology Review - Pertuzumab [Internet]. Washington: U.S. Food and Drug Administration Center for Drug Evaluation and Research; 2011 [cited 2014 October 11]. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/125409Orig1s000TOC.cfm 15. Mattes MJ, Griffiths GL, Diril H, Goldenberg DM, Ong GL, Shih LB. Processing of antibody-radioisotope conjugates after binding to the surface of tumor cells. Cancer. 1994;73:787-93. 16. Thurber GM, Schmidt MM, Wittrup KD. Factors determining antibody distribution in tumors. Trends in pharmacological sciences. 2008;29:57-61. 17. Thurber GM, Schmidt MM, Wittrup KD. Antibody tumor penetration: transport opposed by systemic and antigenmediated clearance. Adv Drug Deliv Rev. 2008;60:1421-34. 18. Li B, Meng Y, Zheng L, Zhang X, Tong Q, Tan W, et al. Bispecific antibody to ErbB2 overcomes trastuzumab resistance through comprehensive blockade of ErbB2 heterodimerization. Cancer Res. 2013;73:6471-83.